Download presentation
Presentation is loading. Please wait.

1
Leon G. Josephs, MD,FACS Chief of Surgery St. Vincent Hospital Worcester, MA

2
Retained Surgical Sponges Define the scope of the problem Discuss impetus for improvement Discuss the process improvement challenges Review St Vincent data Outcomes and summary

3
Retained Sponges Scope 1/1000-1500 abdominal cases 1500 cases per year in US 67% require reoperation Medical-legal cost to hospital is ~$150,000 Stawicki, Scientist, 2008

4
Goals of Process Improvement No SRE No RFB No wrong site No wrong side No wrong patient

5
Impetus for Improvement Retained Sponge January 2007 named Chief of Surgery Early on, two Retained Sponge cases One acute, one delayed 10/07 Dr. Gibbs ACS Clinical Congress Focus on why it occurs via RCA Process Improvement

6
Retained Sponges Impetus for Improvement Counts aren’t perfect-80% “correct” X-rays aren’t perfect SRE Nonpayment events

7
Retained Sponges Why Unmarked towels Poor quality x-rays Poor nursing standards Poor wound exam Poor communication 80% have normal counts Gibbs,Current ProbsSurg, 2007

8
Retained Sponges Risk Factors Risk Factor Emergency surgery Unexpected change High BMI Multivariate analysis Risk Ratio 8.8 4.1 1.1 Gawande, NEJM, 2003

9
Retained Sponges 69% of all RFBs 7% had >1 54% in abdomen 22% in vagina 7% in thorax Gawande, 2003, NEJM

10
Retained Sponges Challenges to Improvement Infrequent event “never happened to me” Surgeons dislike change Skeptics among nursing and physicians Cost

11
Goals of Process Improvement Zero Retained Sponges Reduce Anesthesia Time Reduce Risk to Nursing “sponge search” Eliminate X-ray Improve OR efficiency Liability

12
Process Changes Revise Counts-AORN standards Educate nursing and MD staff Define High Risk Patients for RS Emergency Major change in procedure BMI>30 Multiple sites/cavity

13
MD and Staff Education On line presentation with post test Hands on demonstrations with equipment and wands in all applicable areas – OR, OB and Cath Lab

14
Retained Sponges Detection Methods Wound exam Counts X-ray RF RFID Bar coded

15
Retained Sponge Detection Study St Vincent Hospital 300 beds 17 ORs and four OB rooms 16,000 operations annually Teaching hospital Modern, state of the art facility

16
Retained Sponges Detection Study All high risk patients Counts X-ray RF Surgical Detection System Wanding

17
Detection Study Why RF ? Easy to Use Fast and Accurate Not cost prohibitive Good experience at HUP

18
RF Protocol PROCEDURE/PROTOCOL: Items needed R.F. sponges R.F. console R.F. Sterile wand Place console within 4 feet of the patient’s chest, just outside the sterile field. Connect supplied power cord to back of console. Set the power switch in back of the console to “ON”. Do not disconnect power or turn off the power switch until the scanning is completed. When the power is on, the console will conduct a self-check.

19
RF Protocol When the system ready LED light is illuminated, the wand can be connected. Dispense the wand unto the sterile field and have the scrub person remove it from the wrappings. Pass the silver connector end of the wand off the field to the circulator and then the circulator will connect to the R.F. console. The scrub will then hold the wand up in the air to allow the wand to do a self –check. Indication of scanning will automatically be indicated by the circular array of “Scan” LED’s illuminated green in a clockwise sequence. After a successful wand check, the wand ready LED will illuminate green.

20
RF Protocol The wand will be tested by scanning a R.F. sponge that is on the back table (not on or in the patient). A solid tone and “Scan” LED’s and “Detect” will illuminate yellow. After a successful wand test, scanning of the patient can proceed. If a tag is not detected after completing scanning pattern or if scanning must be stopped, press the “Start-Stop” button. Press the “Start-Stop” button to reinitiate scanning. Console will time out after 4 minutes; to reinitiate scanning press “Start-Stop” button
. A solid tone and Scan LED’s and Detect will illuminate yellow. After a successful wand test, scanning of the patient can proceed. If a tag is not detected after completing scanning pattern or if scanning must be stopped, press the Start-Stop button. Press the Start-Stop button to reinitiate scanning. Console will time out after 4 minutes; to reinitiate scanning press Start-Stop button.")
21
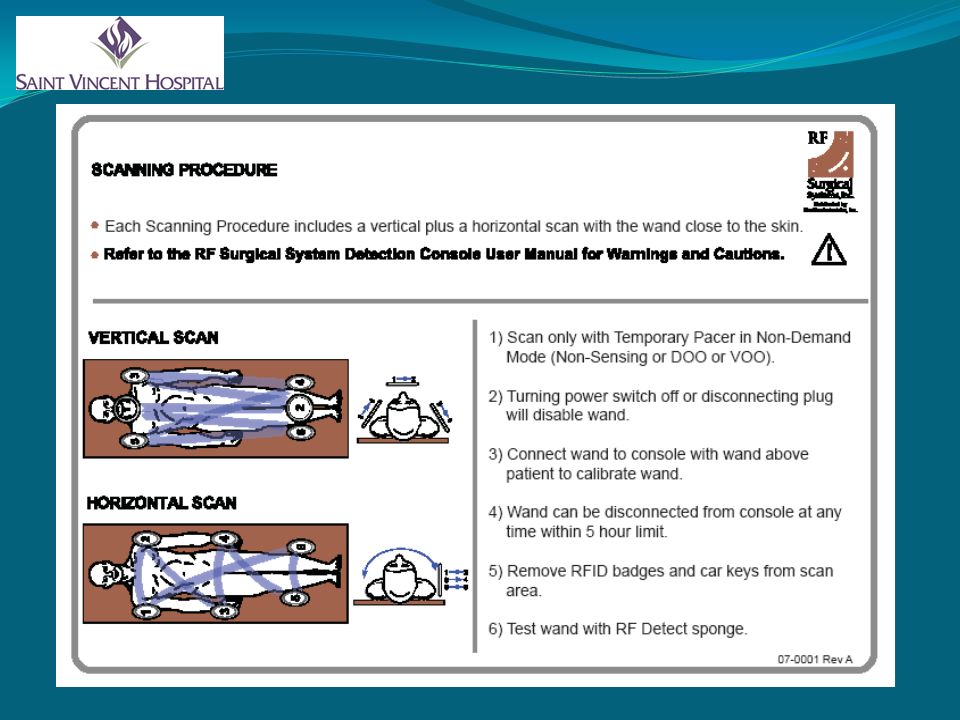
RF Scan Procedure Position wand as close as possible to the body at the neckline. With wand remaining parallel to body, move wand distally to the knees, reverse direction back up to the right shoulder. Start the lateral scan down the right side to the knees and then up to the left shoulder Scan lateral from the left shoulder and back to the knees. Do this at a rate of 3 seconds per pass.

22
RF Scan Procedure Start the horizontal scan by placing the wand lateral on the left shoulder and across chest to the right shoulder. Across the body to the left hip, then across pelvic area to right hip. Proceed across the legs to the left knee and then across the lower legs to the right knee. Proceed then across the whole body to the left shoulder.

24
Retained Sponges Study Design Measured time to get x-ray and reading Measured time to prepare and use RF Detection Reviewed cost and effectiveness 180 consecutive high risk patients

25
Retained Sponge Detection Study Results Patient- 11/7-6/08 Call xray (min) Result (min) Total (min) Wand (min) BMI 1-3015.618.233.81.837.1 31-6011.614.125.71.436.6 61-9010.416.326.71.235.1 91-12010.41424.41.235.8 121-15011.514.826.31.136.4 151-18013.815.329.11236
 Result (min) Total (min) Wand (min) BMI")
26
Retained Sponge Detection No retained sponges RF decreases anesthesia time by approximately thirty minutes High satisfaction with surgeons and nurses

27
Retained Sponges Detection Cost Analysis Reading, tech, film, OR time= $206/case RF with single use and sponge cost of 30 sponges =$55/case Margin is $150,000/1000 cases

29
Retained Sponges Improved patient safety MD and Nursing staff satisfaction Improved OR and hospital efficiency RF is an adjunct to good nursing practice and wound exam by surgeon RF is safer, faster and more cost effective compared to X-ray for retained sponges Considering use of RF instruments

Similar presentations








 for Children Royal Children’s Hospital Melbourne Australia.>")












