Download presentation
Presentation is loading. Please wait.

1
DRUG TREATMENT IN THE ELDERLY

2
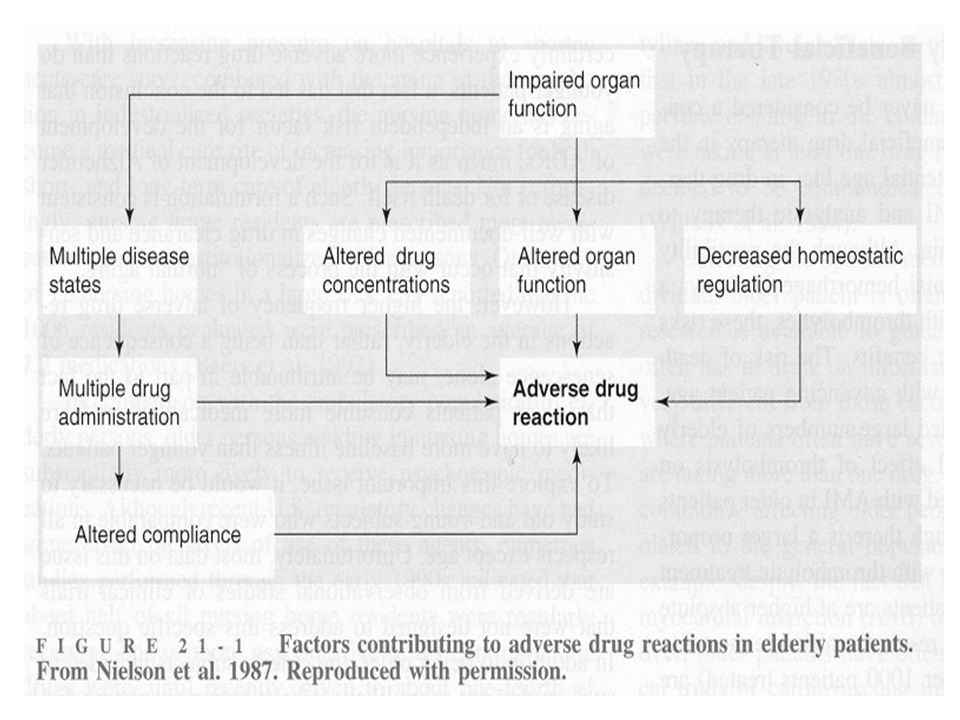
THE BASIC PROBLEM Drug treatment increases (almost exponentially) with age The elderly are presumed to be - because of pharmacodynamic and pharmacokinetic changes with age - more vulnerable to side effects and toxicity of drugs Drug treatment is more risky in the elderly
 with age The elderly are presumed to be - because of pharmacodynamic and pharmacokinetic changes with age - more vulnerable to side effects and toxicity of drugs Drug treatment is more risky in the elderly")
3
DRUG TREATMENT IN THE OLD AGE: Defining the problems "Extrinsic" problems prescribing patterns excessive amounts inadequate indications excessive duration inappropriate regimens drug compliance

4
DRUG TREATMENT IN THE OLD AGE: Defining the problems "Intrinsic" problems pharmacokinetics absorption distribution metabolism excretion pharmacodynamics

5
DRUG SENSITIVITY IN ELDERLY PATIENTS Reduced responsiveness adrenergic drugs Unchanged responsiveness most drugs Increased responsiveness benzodiazepines warfarin

6
DRUG SENSITIVITY IN ELDERLY PATIENTS Loss of homeostatic reserve postural stability ortostatic responses thermoregulation reserve of cognitive functions bowel and bladder function

7
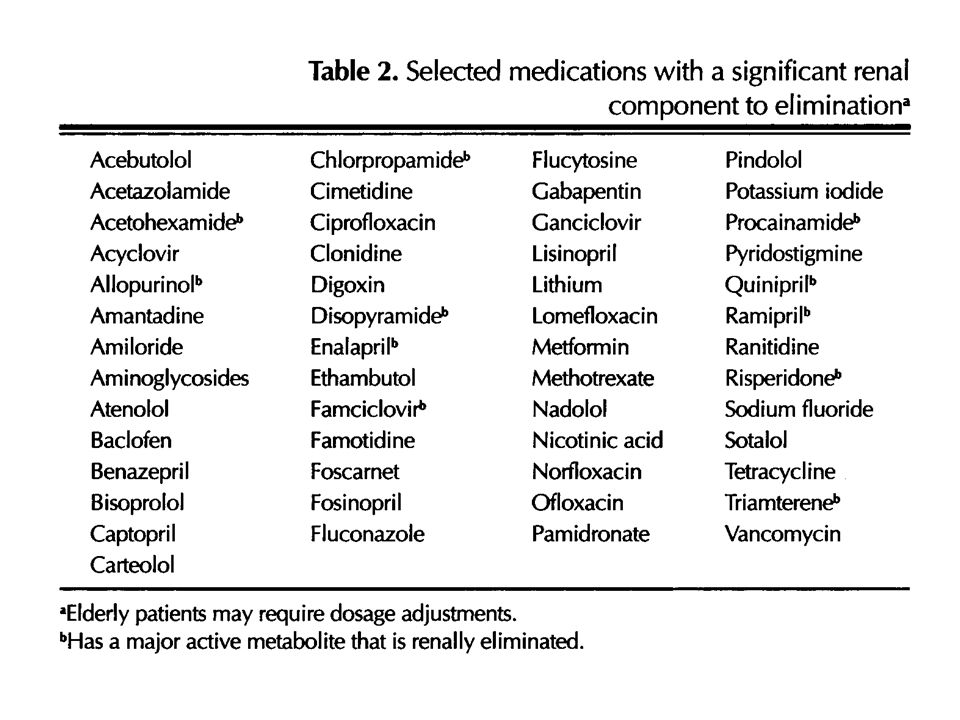
RISKS FOR DRUG TOXICITY IN THE ELDERLY Ageing decreased lean mass increased fat stores decreased renal function decreased hepatic function (Beers and Ouslander, Drugs 37: 105-112, 1989)
")
10
RISKS FOR DRUG TOXICITY IN THE ELDERLY Disease and illness renal failure hepatic diseases congestive heart failure dementia dehydration prostatic hypertrophy ortostatic hypertension pain

11
RISKS FOR DRUG TOXICITY IN THE ELDERLY Psychosocial demanding personality care-givers poverty complex medication regimens (Beers and Ouslander, Drugs 37: 105-112, 1989)
")
12
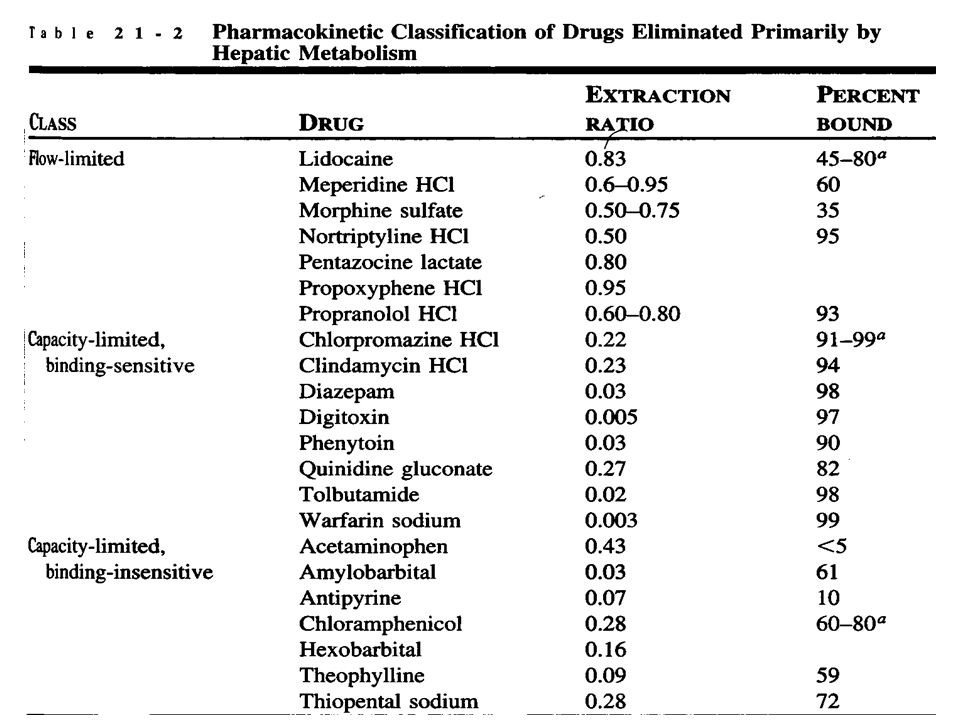
DRUG METABOLISM Drug Oxygenated Metabolite Excretion Conjugated Metabolite Phase I Phase II

13
Ketoconazole Gestodene Midazolam Nifedipine Erythromycin Cyclosporine Tolbutamide Warfarin Phenytoin Mephenytoin Omeprazole Caffeine Theophylline Tacrine Dextrometorpha n Sparteine Debrisoquine Coumarin Chlorzoxazone SUBSTRATES INHIBITORS MethoxsalenFluconazoleSulphaphenazoleFurafylline Fluvoxamine Quinidine Tetrahydro- furane DEDTC INDUCERS Phenobarb. Rifampicin Phenobarb. Rifampicin Phenobarb. Rifampicin Dexamethasone Carbamazepine Omeprazole Tobacco smoke Ethanol Isoniazid CYP2C8/9/18 ~20% CYP1A2 ~15% CYP2C19 <5% CYP2A6 <5% CYP2D6 <5% CYP2E1 ~10% CYP2B6 CYP1A1 CYP3A4/5/7 ~30% No known

14
DETERMINANTS OF DRUG METABOLISM Environmental factors drugs, tobacco,alcohol, occupational exposures, pollution, diet Genetic factors developmental programs multigene factors polymorphisms inborn errors Host factors therapeutic interventions work load, lliver disease other diseases hormonal milieu INDIVIDUAL PHENOTYPE

15
DRUG METABOLISM IN THE ELDERLY How important is age/ageing as a factor causing variability in drug therapy among all the other factors affecting variability? How could age/ageing be taken into consideration in drug therapy?

16
CYP3A4 most abundant in liver (~30%) and gut metabolises >50% of all drugs substrates midazolam, simvastatin, nifedipine, cyclosporine, quinidine, numerous interactions (antimycotics) inducible by antiepileptics, rifampicin, steroids declines considerably during ageing
 and gut metabolises >50% of all drugs substrates midazolam, simvastatin, nifedipine, cyclosporine, quinidine, numerous interactions (antimycotics) inducible by antiepileptics, rifampicin, steroids declines considerably during ageing")
17
MIDAZOLAM Elimination completely dependent on metabolism (oxidation) by CYP3A4 Relatively rapid clearance (half-life ~2-3 hr) Gut wall CYP3A4 participates in oral clearance Clearance retarded ~2-fold in the elderly (only in males?)
 by CYP3A4 Relatively rapid clearance (half-life ~2-3 hr) Gut wall CYP3A4 participates in oral clearance Clearance retarded ~2-fold in the elderly (only in males )")
18
Effect of inhibitors and inducers on midazolam metabolism in vitro and in vivo Substance Effect AUC change (%) Erythromycininhibitor 442 Azithromycininhibitor 87 Fluconazoleinhibitor 373 Itraconazoleinhibitor 1080 Ketoconazoleinhibitor 1590 Rifampicininducer 4 Neuvonen et al 1993-1998
 Erythromycininhibitor 442 Azithromycininhibitor 87 Fluconazoleinhibitor 373 Itraconazoleinhibitor 1080 Ketoconazoleinhibitor 1590 Rifampicininducer 4 Neuvonen et al")
19
CYP2D6 relatively minor in liver (~4%) metabolises >50 drugs substrates midazolam, simvastatin, genetic polymorphisms (>50 variant alleles known): poor metabolizer phenotype numerous interactions (quinidine) very little decline during ageing
 metabolises >50 drugs substrates midazolam, simvastatin, genetic polymorphisms (>50 variant alleles known): poor metabolizer phenotype numerous interactions (quinidine) very little decline during ageing")
20
Examples of Drugs Metabolized by CYP2D6 Captopril Debrisoquine Desipramine Dextrometorphan Fluoxetine Haloperidol Lidocaine Metoprolol Paroxetine Phenformin Propranolol Sparteine Thioridazine Timolol

21
Drug treatment in elderly: beta-blockers Metoprolol metabolically cleared (CYP2D6, others) large interindividual variation age not an important factor Sotalol renally cleared small interindividual variation decrease in renal function
 large interindividual variation age not an important factor Sotalol renally cleared small interindividual variation decrease in renal function")
22
DRUG TREATMENT IN THE ELDERLY Is it possible to predict dose and regimen in an individual geriatric patient? - from clinical information? - from “general knowledge” of age-related pharmacokinetics and -dynamics - from specific “probes”

34
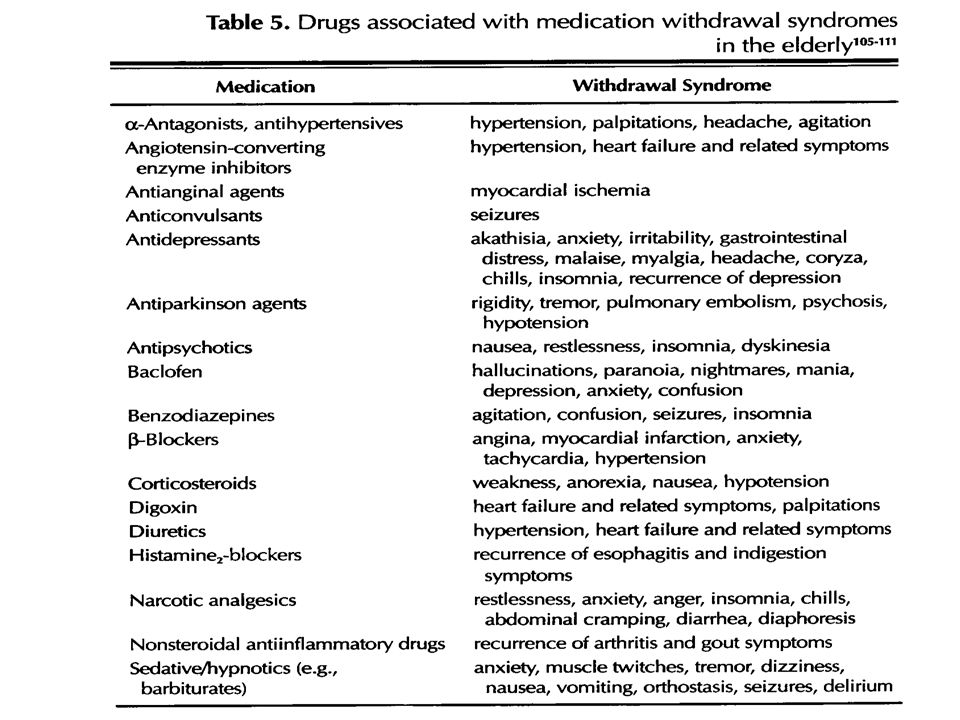
CONCLUSIONS Aging is a factor in pharmacokinetics and pharmacodynamics Other factors (genetic, environmental, host) may be more important than aging as such Age-related changes are dependent on specific drugs, individuals and situations; thus generalisations are difficult and uncertain A scheme for risk management is proposed
 may be more important than aging as such Age-related changes are dependent on specific drugs, individuals and situations; thus generalisations are difficult and uncertain A scheme for risk management is proposed")
Similar presentations










? Pain Inflammation Infection Fluid retention Heart problems High.>")


















