Download presentation
Presentation is loading. Please wait.

1
POSTERIOR PITUITARY

2
Hypothalamic Control of Posterior Pituitary
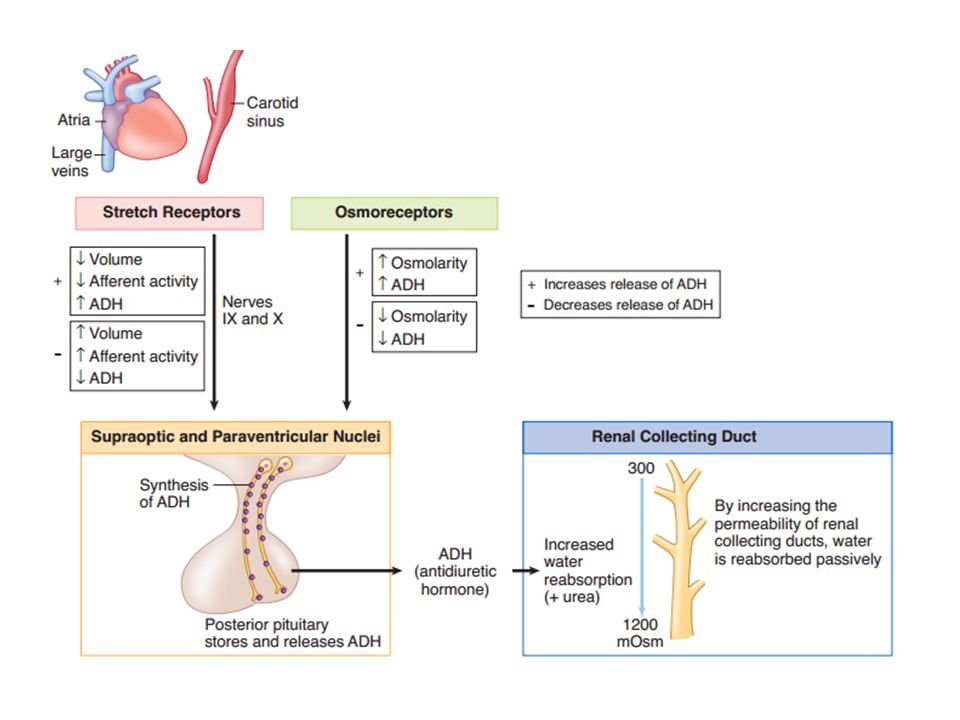
Hypothalamic neuron cell bodies produce: ADH: supraoptic nuclei. Oxytocin: para ventricular nuclei. Transported along hypothalamo-hypophyseal tract. Stored in posterior pituitary. Release controlled by neuroendocrine reflexes. ADH and oxytocin are released from the pars nervosa in response to stimuli that are primarily detected at the cell body and its dendrites in the SON and PVN of the hypothalamus. The stimuli are mainly in the form of neurotransmitters released from hypothalamic interneurons. With sufficient stimulus, the neurons will depolarize and propagate an action potential down the axon. At the axonal termini, the action potential increases intracellular [Ca++] and results in a stimulus-secretion response, with the exocytosis of ADH or oxytocin, along with neurophysins, into the extracellular fluid of the pars nervosa Hormones and neurophysins enter the peripheral circulation, and both can be measured in blood.

4
The osmoreceptor neurons in the hypothalamus are extremely sensitive and are able to maintain ECF osmolarity within a very narrow range. There is a reseting of the osmostat downward in pregnancy, the men-strual cycle, and with volume depletion. In the latter case osmoregula-tion is secondary to volume regulation; a return of circulating volume will occur even as osmolarity decreases. Volume receptors are less sensitive than osmoreceptors and a change of 10–15% in volume is required to produce a measureable change in ADH. Cortisol and thyroid hormone restrain the release of ADH.

5
At the kidney (collecting duct)
ADH cAMP V2 Vesicles containing AQP2 ’s AQP2 production Nephron lumen Interstitial Space

6
ACTIONS OF ADH 1.ACTION ON KIDNEY Maintenance of ECF volume & Osmolarity Acts on DCT and CD of kidney Reabsorbs water Maintenance of volume more important that maintenance of osmolarity 2.VASOCONSTRICTOR EFFECT 3.ACTION ON ANTERIOR PITUITARY-cause increased ACTH secretion from the corticotroph The main target tissue is the renal collecting duct (V2 receptors). l ADH increases the permeability of the duct to water by placing water channels in the luminal membrane. l Water is reabsorbed passively, drawn across the membranes by the higher osmolarity of the interstitium. l Urea can pass with the water, but electrolytes cannot. l In severe hemorrhage, high levels of ADH via V1 receptors on vascular smooth muscle cause a vasoconstriction
. l ADH increases the permeability of the duct to water by placing water. channels in the luminal membrane. l Water is reabsorbed passively, drawn across the membranes by the higher. osmolarity of the interstitium. l Urea can pass with the water, but electrolytes cannot. l In severe hemorrhage, high levels of ADH via V1 receptors on vascular. smooth muscle cause a vasoconstriction.")
7
Effect of Alcohol and Weightlessness on ADH Secretion
Ingesting ethyl alcohol or being in a weightless environment suppresses ADH se-cretion. In weightlessness, there is a net shift of blood from the limbs to the abdo-men and chest. This results in greater stretch of the volume receptors in the large veins and atria, thus suppressing ADH secretion

8
pATHOpHYSIOLOgIC CHANgES IN ADH SECRETION

9
Central diabetes insipidus
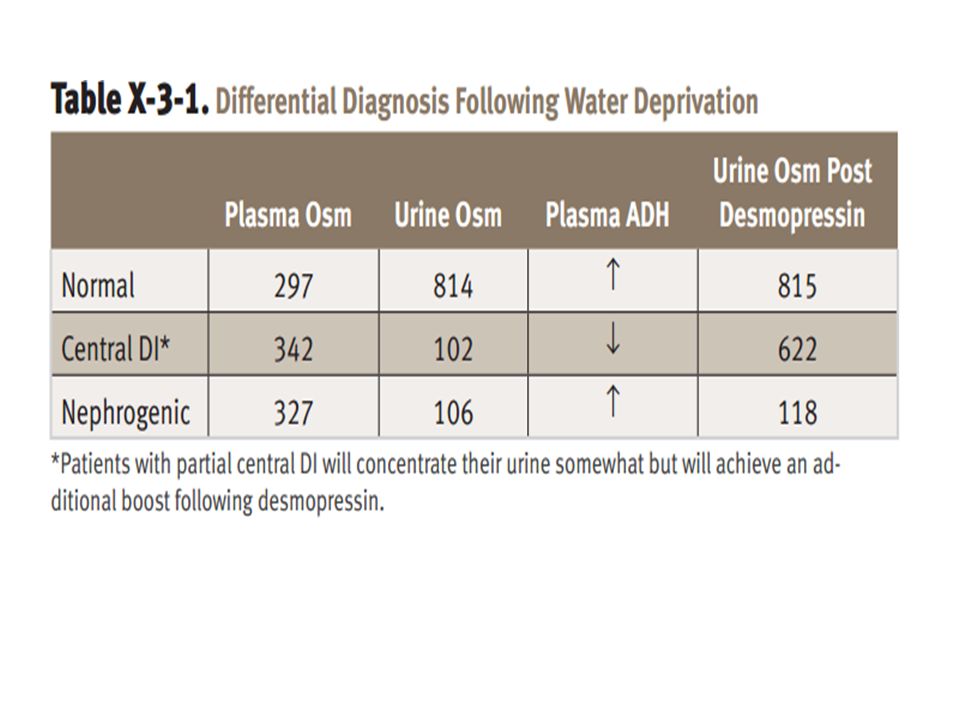
Sufficient ADH is not available to affect the renal collecting ducts. Causes include familial, tumors (craniopharyngioma), autoimmune, trauma Pituitary trauma – transient diabetes insipidus Sectioning of pituitary stalk – triphasic response: diabetes insipidus, followed by SIADH, followed by a return of diabetes insipidus
, autoimmune, trauma. Pituitary trauma – transient diabetes insipidus. Sectioning of pituitary stalk – triphasic response: diabetes insipidus, followed by SIADH, followed by a return of diabetes insipidus.")
10
Nephrogenic diabetes insipidus
Due to inability of the kidneys to respond to ADH Causes include familial, acquired, drugs (lithium)
")
12
Syndrome of Inappropriate ADH Secretion (SIADH)
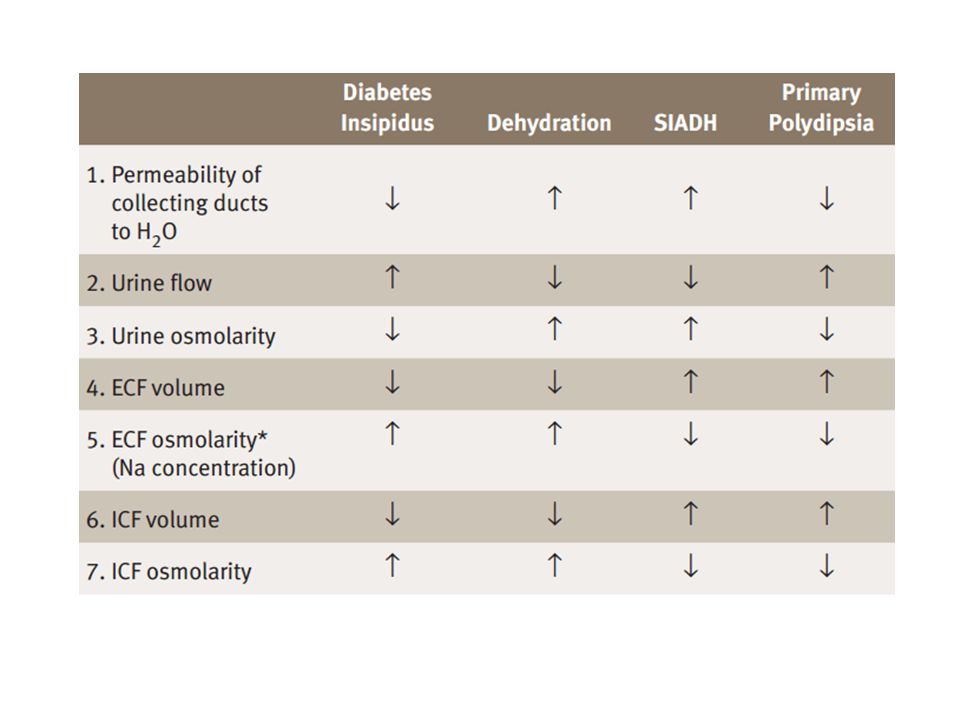
Excessive secretion of ADH causes an inappropriate increased reabsorption of water in the renal collecting duct. Causes Ectopic production of ADH (small cell carcinoma of the lung) Drug induced Lesions in the pathway of the baroreceptor system Pathophysiology Increased water retention, hyponatremia, but clinically euvolumic Volume expansion increases ANP, decreases renin creating a natriuresis, which contributes to the hyponatremia Inappropriate concentration of urine, can be greater than plasma osmo-larity A small, constant secretion of ADH by a tumor may have a minimal effect on the ability to form dilute urine but has a major effect on the ability to excrete a large water load. Treatment Fluid restriction but not salt restriction
 Drug induced. Lesions in the pathway of the baroreceptor system. Pathophysiology. Increased water retention, hyponatremia, but clinically euvolumic. Volume expansion increases ANP, decreases renin creating a natriuresis, which contributes to the hyponatremia. Inappropriate concentration of urine, can be greater than plasma osmo-larity. A small, constant secretion of ADH by a tumor may have a minimal effect. on the ability to form dilute urine but has a major effect on the ability to. excrete a large water load. Treatment. Fluid restriction but not salt restriction.")
14
Oxytocin 9 AA peptide Stored in Herring bodies
Nerve stimulation release Half life ~ 4 minutes

15
Pressure against cervix
Hypothalamus Nursing Pressure against cervix Posterior Pituitary Oxytocin

16
At the target cell Oxytocin Contraction IP3 & DAG Ca2+
Smooth muscle cell

17
Actions of oxytocin In females: Milk ejection
Contraction of uterus during labor In females: during coitus causes uterine contraction and transport of sperms In Males: Increases at time of ejaculation May cause increase contraction of smooth muscle of vas deferens - propelling sperm through urethra

18
milk-ejection reflex

20
IN THE CLINIC-- hypophysectomy (pituitary removal)
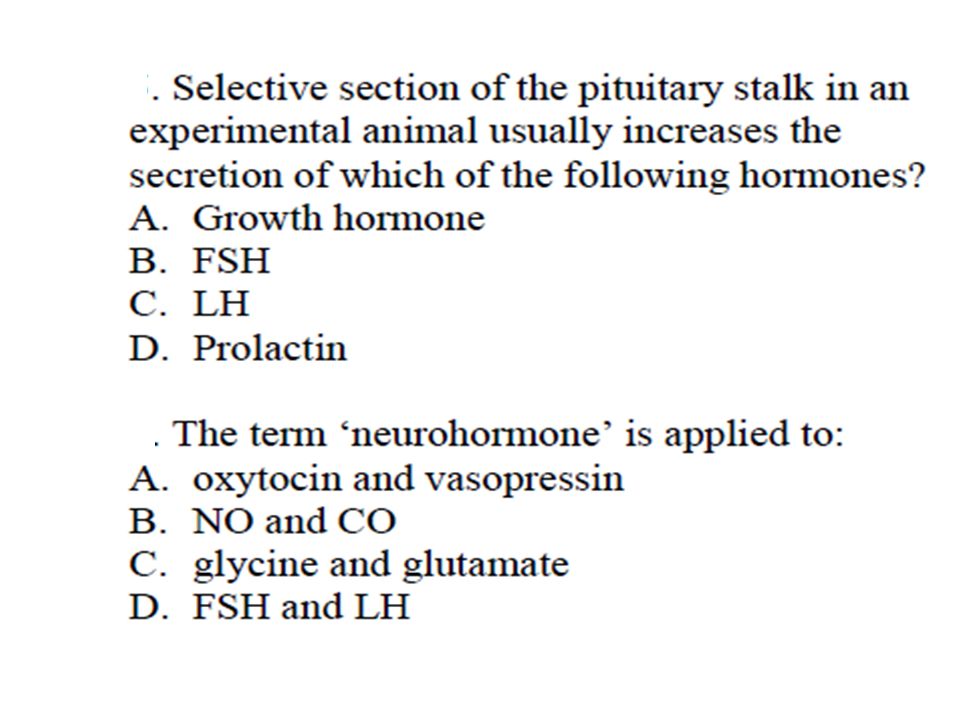
Because posterior pituitary hormones are synthesized in the hypothalamus rather than the pituitary, hypophysectomy (pituitary removal) does not necessarily permanently disrupt synthesis and secretion of these hormones. Immediately after hypophysectomy, secretion of the hormones decreases. However, over a period of weeks, the severed proximal end of the tract will show histological modification and pituicytes will form around the neuron terminals. Secretory vacuoles are seen, and secretion of hormone resumes from this proximal end. Secretion of hormone can even potentially return to normal levels. In contrast, a lesion higher up on the pituitary stalk can lead to loss of neuronal cell bodies in the PVN and SON.
 does not necessarily permanently disrupt synthesis and secretion of these hormones. Immediately after hypophysectomy, secretion of the hormones decreases. However, over a period of weeks, the severed proximal end of the tract will show histological modification and pituicytes will form around the neuron terminals. Secretory vacuoles are seen, and secretion of hormone resumes from this proximal end. Secretion of hormone can even potentially return to normal levels. In contrast, a lesion higher up on the pituitary stalk can lead to loss of neuronal cell bodies in the PVN and SON.")
Similar presentations











 is an uncommon condition that occurs when the kidneys are unable to conserve.>")

 response How the anterior and posterior pituitary.>")






