Download presentation
Presentation is loading. Please wait.

1
Holger Schünemann Professor of Clinical Epidemiology, Biostatistics and Medicine McMaster University, Hamilton, Canada Italian NCI „Regina Elena“, Rome, Italy

2
Content Describe the grade of recommendation and what each category means: strong/weak and optional language How the quality of evidence can be upgraded/down-graded What happens when you’re recommending something not be done? Maybe provide some ID-type examples if possible - I’m attaching our clinical questions that may be used as examples? Provide a quick tutorial of GRADEPro Questions

3
The GRADE approach Clear separation of 2 issues: 1) 4 categories of quality of evidence: very low, low, moderate, or high quality? methodological considerations likelihood of systematic deviation from truth by outcome 2) Recommendation: 2 grades – weak/conditional or strong (for or against)? Quality of evidence only one factor Influenced by magnitude of effect(s) – balance of benefits and harms, values and preferences, cost *www.GradeWorkingGroup.org
 Recommendation: 2 grades – weak/conditional or strong (for or against). Quality of evidence only one factor Influenced by magnitude of effect(s) – balance of benefits and harms, values and preferences, cost *")
4
Content Describe the grade of recommendation and what each category means: strong/weak and optional language How the quality of evidence can be upgraded/down-graded What happens when you’re recommending something not be done? Maybe provide some ID-type examples if possible - I’m attaching our clinical questions that may be used as examples? Provide a quick tutorial of GRADEPro Questions

5
Implications of a strong recommendation Patients: Most people in this situation would want the recommended course of action and only a small proportion would not Clinicians: Most patients should receive the recommended course of action Policy makers: The recommendation can be adapted as a policy in most situations

6
Implications of a weak recommendation Patients: The majority of people in this situation would want the recommended course of action, but many would not Clinicians: Be prepared to help patients to make a decision that is consistent with their own values/decision aids and shared decision making Policy makers: There is a need for substantial debate and involvement of stakeholders

7
Content Describe the grade of recommendation and what each category means: strong/weak and optional language How the quality of evidence can be upgraded/down-graded What happens when you’re recommending something not be done? Maybe provide some ID-type examples if possible - I’m attaching our clinical questions that may be used as examples? Provide a quick tutorial of GRADEPro Questions

8
Answer Same type of interpretation

9
Content Describe the grade of recommendation and what each category means: strong/weak and optional language How the quality of evidence can be upgraded/down-graded What happens when you’re recommending something not be done? Maybe provide some ID-type examples if possible - I’m attaching our clinical questions that may be used as examples? Provide a quick tutorial of GRADEPro Questions

10
Determinants of quality - For body of evidence - RCTs start high observational studies start low 5 factors that can lower quality 1. limitations of detailed design and execution 2. inconsistency 3. Indirectness/applicability 4. publication bias 5. Imprecision 3 factors can increase quality 1. large magnitude of effect 2. all plausible confounding may be working to reduce the demonstrated effect or increase the effect if no effect was observed 3. dose-response gradient

11
Assessing the quality of evidence 11

12
1. Design and Execution limitations lack of concealment intention to treat principle violated inadequate blinding loss to follow-up early stopping for benefit selective outcome reporting Example: RCT suggests that danaparoid sodium is of benefit in treating HIT complicated by thrombosis Key outcome: clinicians’ assessment of when the thromboembolism had resolved Not blinded – subjective judgement

13
2. Inconsistency of results (Heterogeneity) if inconsistency, look for explanation patients, intervention, outcome, methods unexplained inconsistency downgrade quality Bleeding in thrombosis-prophylaxed hospitalized patients seven RCTs 4 lower, 3 higher risk
 if inconsistency, look for explanation patients, intervention, outcome, methods unexplained inconsistency downgrade quality Bleeding in thrombosis-prophylaxed hospitalized patients seven RCTs 4 lower, 3 higher risk.")
14
Example: Bleeding in the hospital Dentali et al. Ann Int Med, 2007

15
Judgment variation in size of effect overlap in confidence intervals statistical significance of heterogeneity I2I2

16
Akl E, Barba M, Rohilla S, Terrenato I, Sperati F, Schünemann HJ. “Anticoagulation for the long term treatment of venous thromboembolism in patients with cancer”. Cochrane Database Syst Rev. 2008 Apr 16;(2):CD006650. Heparin or vitamin K antagonists for survival in patients with cancer
:CD Heparin or vitamin K antagonists for survival in patients with cancer.")
17
Non-steroidal drug use and risk of pancreatic cancer Capurso G, Schünemann HJ, Terrenato I, Moretti A, Koch M, Muti P, Capurso L, Delle Fave G. Meta-analysis: the use of non-steroidal anti-inflammatory drugs and pancreatic cancer risk for different exposure categories. Aliment Pharmacol Ther. 2007 Oct 15;26(8):1089-99.
:")
18
3. Directness of Evidence differences in populations/patients (mild versus severe COPD, older, sicker or more co-morbidity) interventions (all inhaled steroids, new vs. old) outcomes (important vs. surrogate; long-term health- related quality of life, short –term functional capacity, laboratory exercise, spirometry) indirect comparisons interested in A versus B have A versus C and B versus C formoterol versus salmeterol versus tiotropium
 interventions (all inhaled steroids, new vs. old) outcomes (important vs. surrogate; long-term health- related quality of life, short –term functional capacity, laboratory exercise, spirometry) indirect comparisons interested in A versus B have A versus C and B versus C formoterol versus salmeterol versus tiotropium.")
19
Alendronate Risedronate Placebo Directness interested in A versus B available data A vs C, B vs C

20
4. Publication Bias & Imprecision Publication bias number of small studies

21
Egger M, Smith DS. BMJ 1995;310:752-54 21 I.V. Mg in acute myocardial infarction Publication bias Meta-analysis Yusuf S.Circulation 1993 ISIS-4 Lancet 1995

22
Egger M, Cochrane Colloquium Lyon 2001 22 Funnel plot Standard Error Odds ratio 0.10.313 3 2 1 0 100.6 Symmetrical: No publication bias

23
Egger M, Cochrane Colloquium Lyon 2001 23 Funnel plot Standard Error Odds ratio 0.10.313 3 2 1 0 100.6 Asymmetrical: Publication bias?

24
Egger M, Smith DS. BMJ 1995;310:752-54 24 I.V. Mg in acute myocardial infarction Publication bias Meta-analysis Yusuf S.Circulation 1993 ISIS-4 Lancet 1995

25
Egger M, Smith DS. BMJ 1995;310:752-54 25 Meta- analysis confirme d by mega- trials

26
26 Publication bias (File Drawer Problem) Faster and multiple publication of “positive” trials Fewer and slower publication of “negative” trials
 Faster and multiple publication of positive trials Fewer and slower publication of negative trials")
27
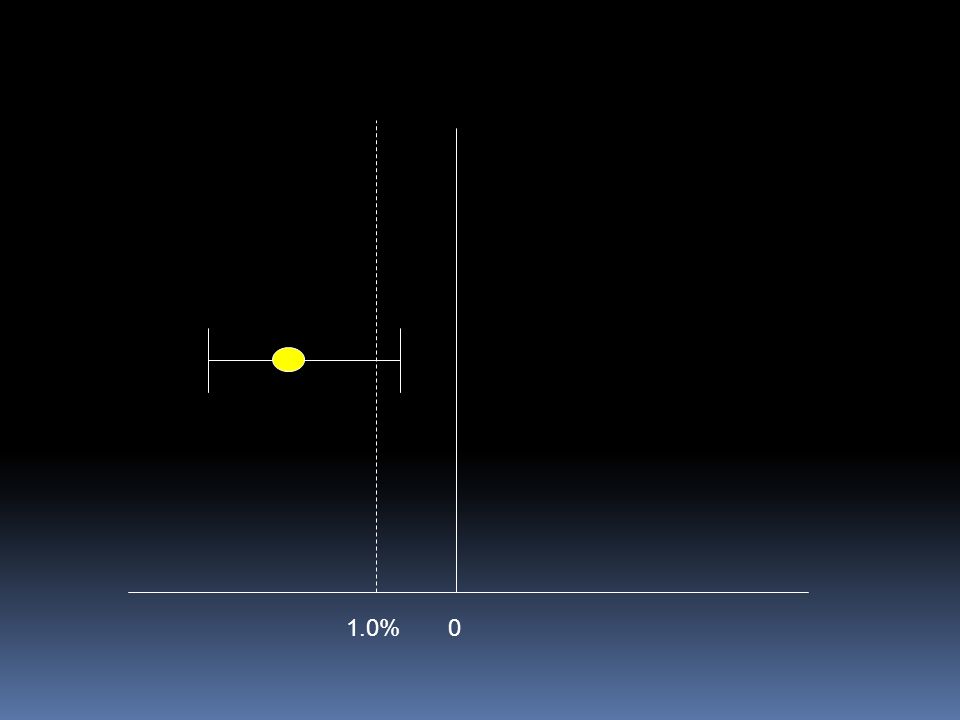
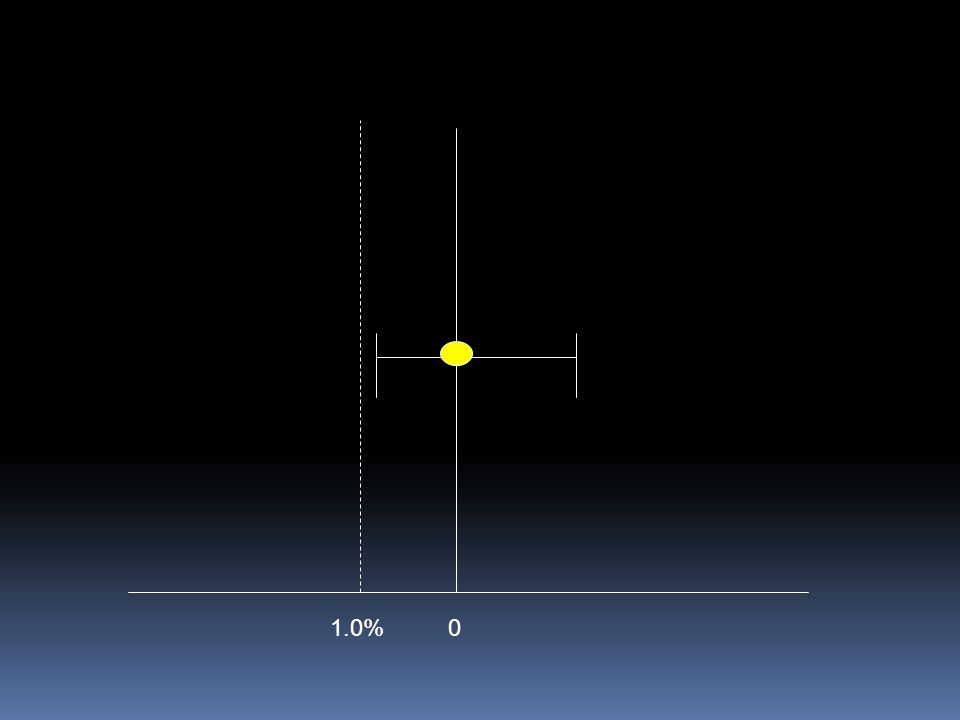
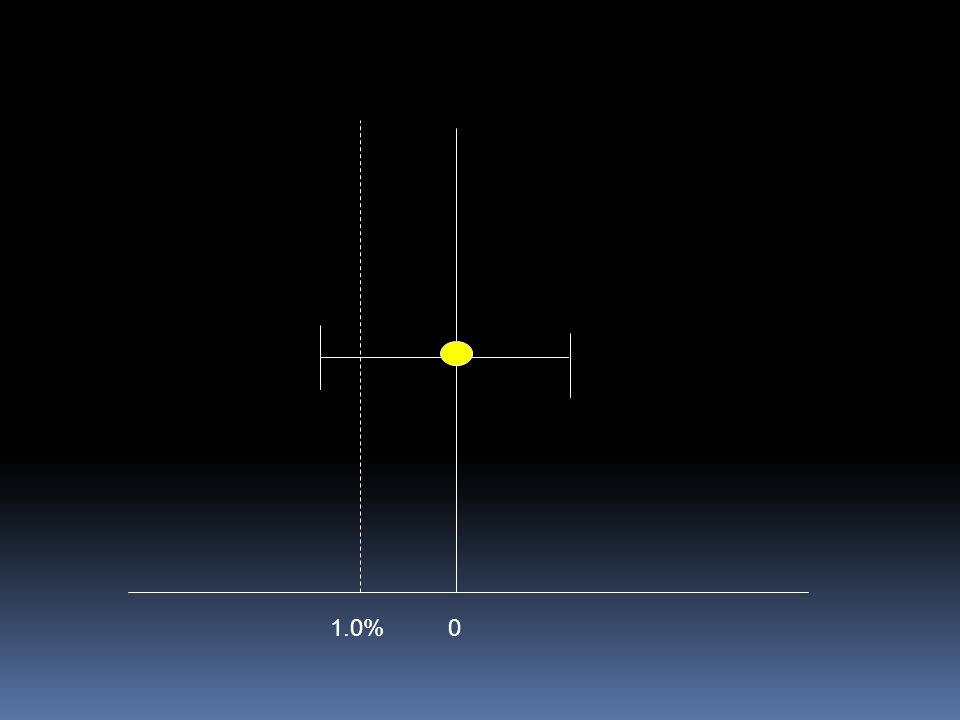
5. Imprecision small sample size small number of events wide confidence intervals uncertainty about magnitude of effect how to decide if CI too wide? grade down one level? grade down two levels? extent to which confidence in estimate of effect adequate to support decision

28
Example: Bleeding in the hospital Dentali et al. Ann Int Med, 2007

29
Offer all effective treatments? atrial fib at risk of stroke warfarin increases serious gi bleeding 3% per year 1,000 patients 1 less stroke 30 more bleeds for each stroke prevented 1,000 patients 100 less strokes 3 strokes prevented for each bleed where is your threshold? how many strokes in 100 with 3% bleeding?

30
01.0%

31
0
32
0
33
0
34
What can raise quality? 1. large magnitude can upgrade (RRR 50%) very large two levels (RRR 80%) common criteria everyone used to do badly almost everyone does well oral anticoagulation for mechanical heart valves insulin for diabetic ketoacidosis hip replacement for severe osteoarthritis 2. dose response relation (higher INR – increased bleeding) 3. all plausible confounding may be working to reduce the demonstrated effect or increase the effect if no effect was observed
 very large two levels (RRR 80%) common criteria everyone used to do badly almost everyone does well oral anticoagulation for mechanical heart valves insulin for diabetic ketoacidosis hip replacement for severe osteoarthritis 2. dose response relation (higher INR – increased bleeding) 3. all plausible confounding may be working to reduce the demonstrated effect or increase the effect if no effect was observed.")
35
All plausible confounding would result in an underestimate of the treatment effect Higher death rates in private for-profit versus private not-for-profit hospitals patients in the not-for-profit hospitals likely sicker than those in the for-profit hospitals for-profit hospitals are likely to admit a larger proportion of well-insured patients than not-for- profit hospitals (and thus have more resources with a spill over effect)
")
36
All plausible biases would result in an overestimate of effect Hypoglycaemic drug phenformin causes lactic acidosis The related agent metformin is under suspicion for the same toxicity. Large observational studies have failed to demonstrate an association Clinicians would be more alert to lactic acidosis in the presence of the agent

37
Content Describe the grade of recommendation and what each category means: strong/weak and optional language How the quality of evidence can be upgraded/down-graded What happens when you’re recommending something not be done? Maybe provide some ID-type examples if possible - I’m attaching our clinical questions that may be used as examples? Provide a quick tutorial of GRADEPro Questions

38
Relevant clinical question? Example from a not so common disease Clinical question: Population: Avian Flu/influenza A (H5N1) patients Intervention: Oseltamivir (or Zanamivir) Comparison: No pharmacological intervention Outcomes: Mortality, hospitalizations, resource use, adverse outcomes, antimicrobial resistance Schunemann et al. The Lancet ID, 2007
 patients Intervention: Oseltamivir (or Zanamivir) Comparison: No pharmacological intervention Outcomes: Mortality, hospitalizations, resource use, adverse outcomes, antimicrobial resistance Schunemann et al. The Lancet ID,")
39
Methods – WHO Rapid Advice Guidelines for management of Avian Flu Applied findings of a recent systematic evaluation of guideline development for WHO/ACHR Group composition (including panel of 13 voting members): clinicians who treated influenza A(H5N1) patients infectious disease experts basic scientists public health officers methodologists Independent scientific reviewers: Identified systematic reviews, recent RCTs, case series, animal studies related to H5N1 infection
: clinicians who treated influenza A(H5N1) patients infectious disease experts basic scientists public health officers methodologists Independent scientific reviewers: Identified systematic reviews, recent RCTs, case series, animal studies related to H5N1 infection")
40
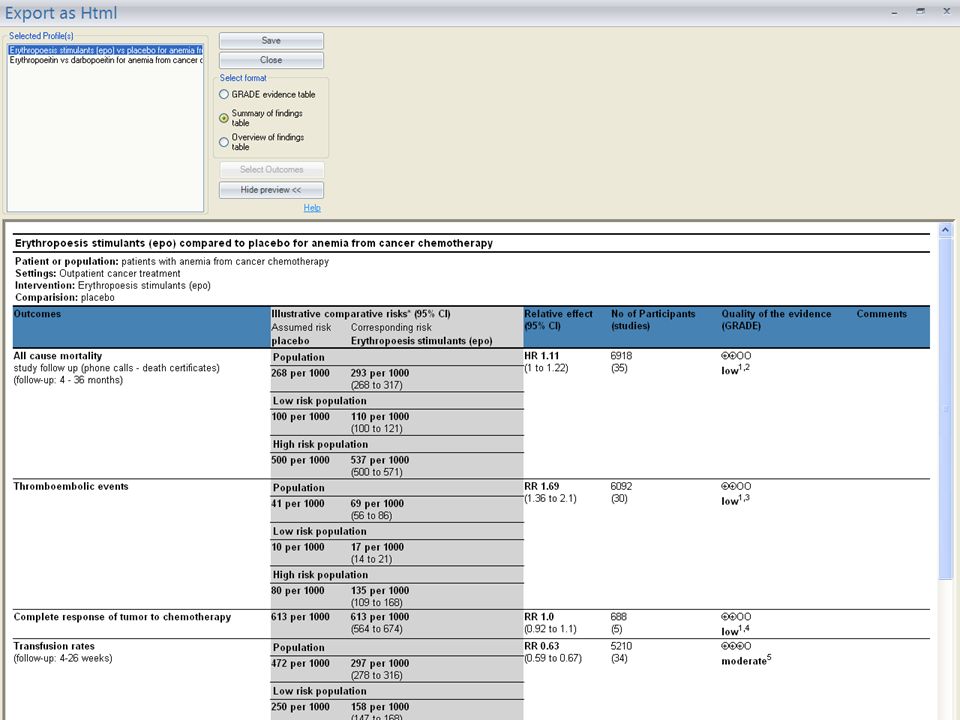
Evidence Profile Oseltamivir for treatment of H5N1 infection: - -

41
Oseltamivir for Avian Flu Summary of findings: No clinical trial of oseltamivir for treatment of H5N1 patients. 4 systematic reviews and health technology assessments (HTA) reporting on 5 studies of oseltamivir in seasonal influenza. Hospitalization: OR 0.22 (0.02 – 2.16) Pneumonia: OR 0.15 (0.03 - 0.69) 3 published case series. Many in vitro and animal studies. No alternative that is more promising at present. Cost: ~ 40$ per treatment course Schunemann et al. Lancet ID, 2007 & PLOS Medicine 2007
 reporting on 5 studies of oseltamivir in seasonal influenza. Hospitalization: OR 0.22 (0.02 – 2.16) Pneumonia: OR 0.15 ( ) 3 published case series. Many in vitro and animal studies. No alternative that is more promising at present. Cost: ~ 40$ per treatment course Schunemann et al. Lancet ID, 2007 & PLOS Medicine")
42
Determinants of the strength of recommendation

43
Example: Oseltamivir for Avian Flu Recommendation: In patients with confirmed or strongly suspected infection with avian influenza A (H5N1) virus, clinicians should administer oseltamivir treatment as soon as possible (????? recommendation, very low quality evidence). Schunemann et al. The Lancet ID, 2007
. Schunemann et al. The Lancet ID,")
44
Example: Oseltamivir for Avian Flu Recommendation: In patients with confirmed or strongly suspected infection with avian influenza A (H5N1) virus, clinicians should administer oseltamivir treatment as soon as possible (strong recommendation, very low quality evidence). Values and Preferences Remarks: This recommendation places a high value on the prevention of death in an illness with a high case fatality. It places relatively low values on adverse reactions, the development of resistance and costs of treatment. Schunemann et al. The Lancet ID, 2007

45
Other explanations Remarks: Despite the lack of controlled treatment data for H5N1, this is a strong recommendation, in part, because there is a lack of known effective alternative pharmacological interventions at this time. The panel voted on whether this recommendation should be strong or weak and there was one abstention and one dissenting vote.

46
Strength of recommendation “The strength of a recommendation reflects the extent to which we can, across the range of patients for whom the recommendations are intended, be confident that desirable effects of a management strategy outweigh undesirable effects.” Strong or weak/conditional

47
Quality of evidence & strength of recommendation Linked but no automatism Other factors beyond the quality of evidence influence our confidence that adherence to a recommendation causes more benefit than harm Systems/approaches failed to make this explicit GRADE separates quality of evidence from strength of recommendation

48
Content Describe the grade of recommendation and what each category means: strong/weak and optional language How the quality of evidence can be upgraded/down-graded What happens when you’re recommending something not be done? Maybe provide some ID-type examples if possible - I’m attaching our clinical questions that may be used as examples? Provide a quick tutorial of GRADEPro Questions

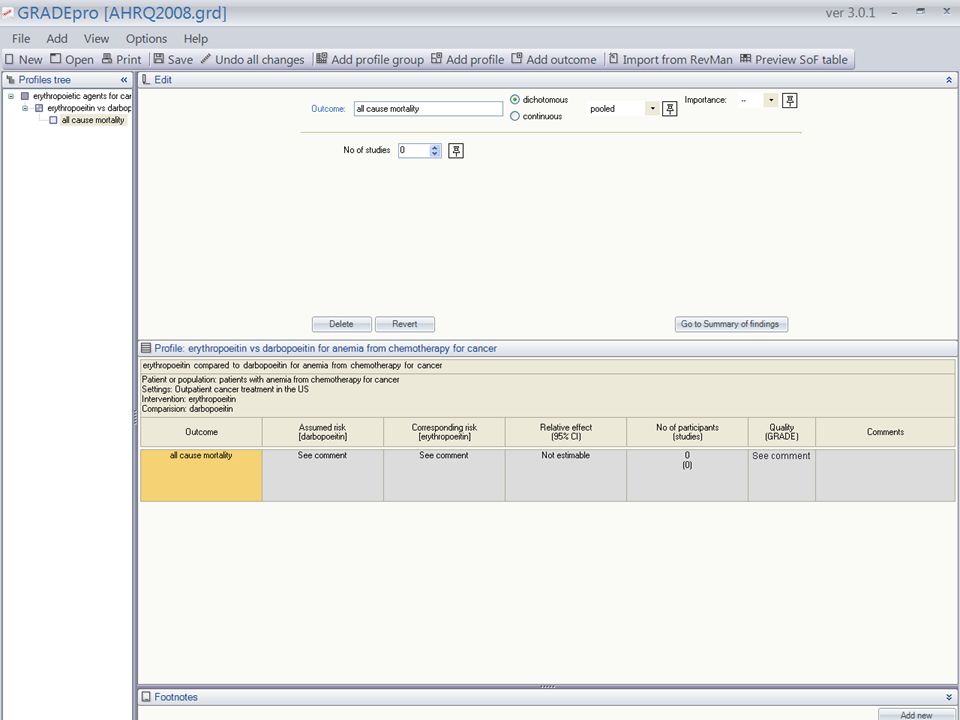
49
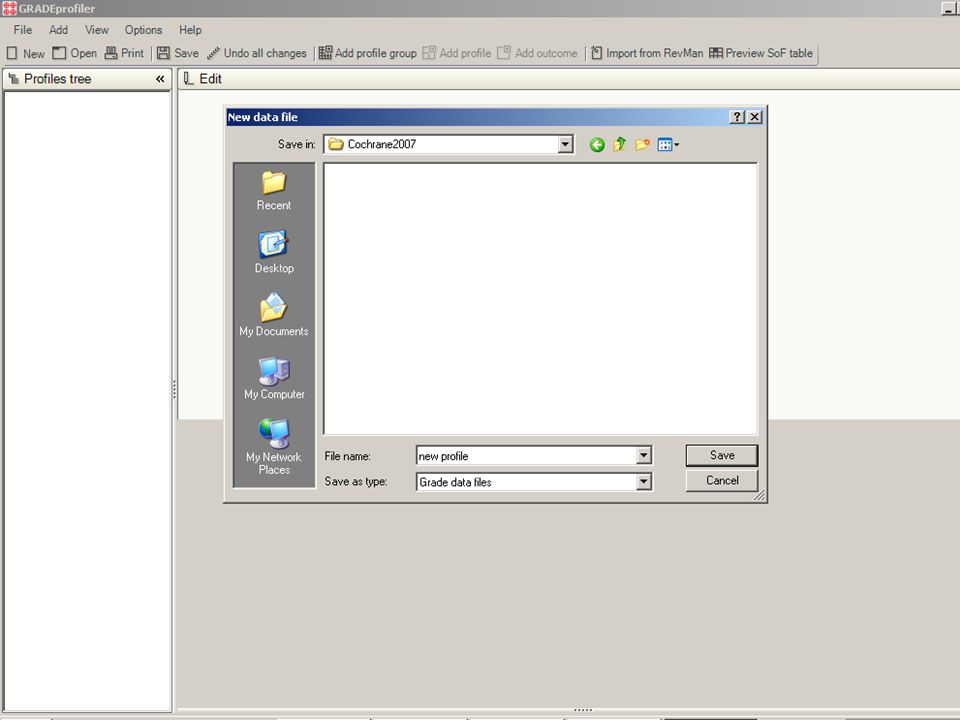
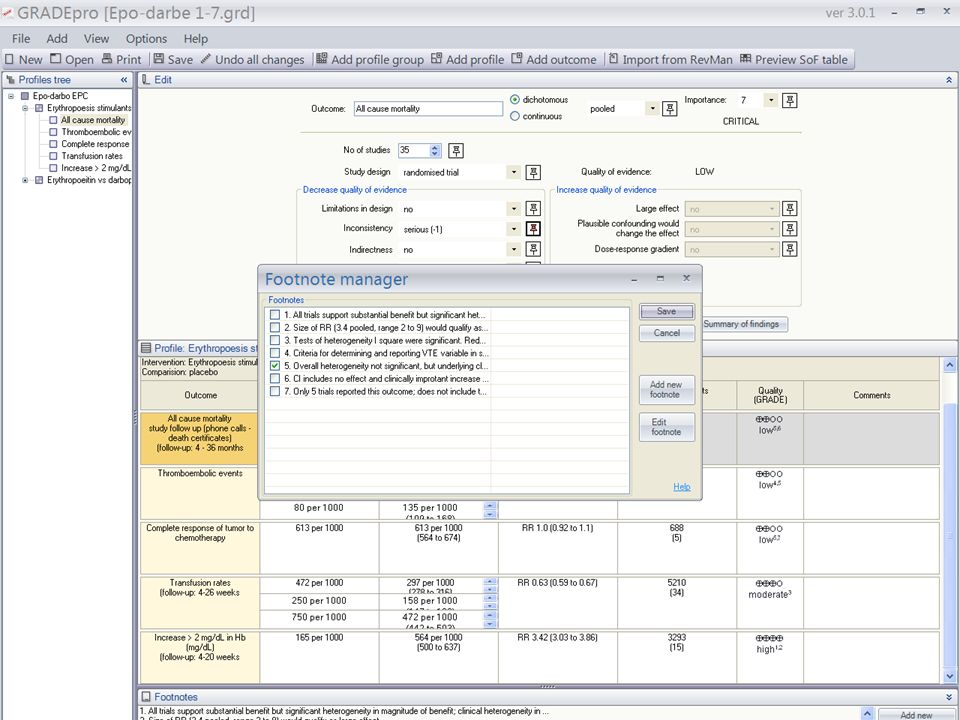
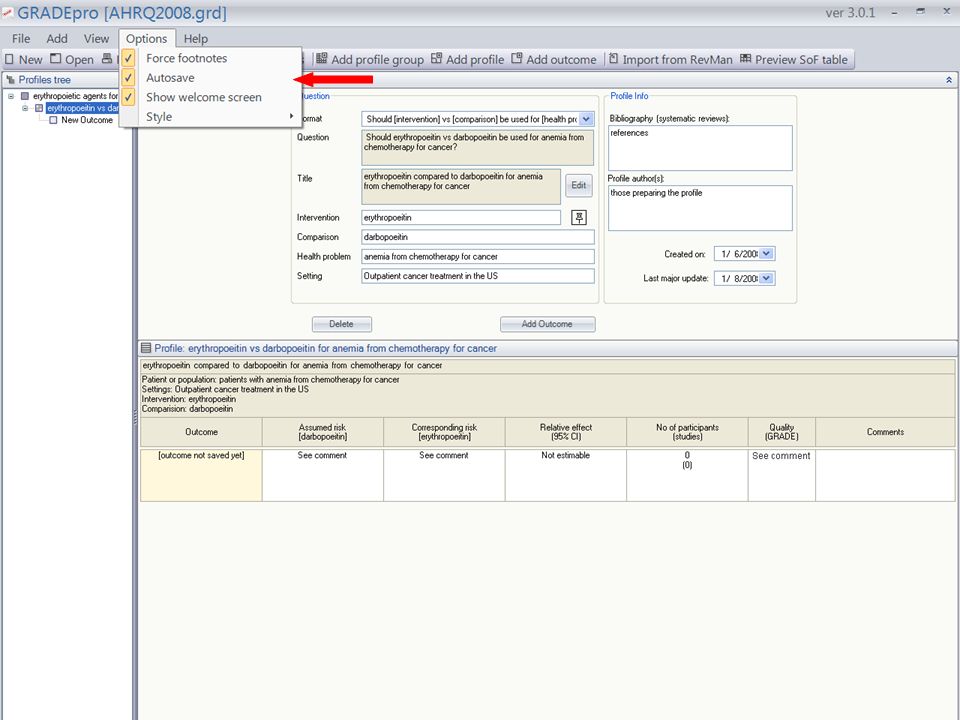
Creating a new GRADEpro file

52
Profile groups Profiles

53
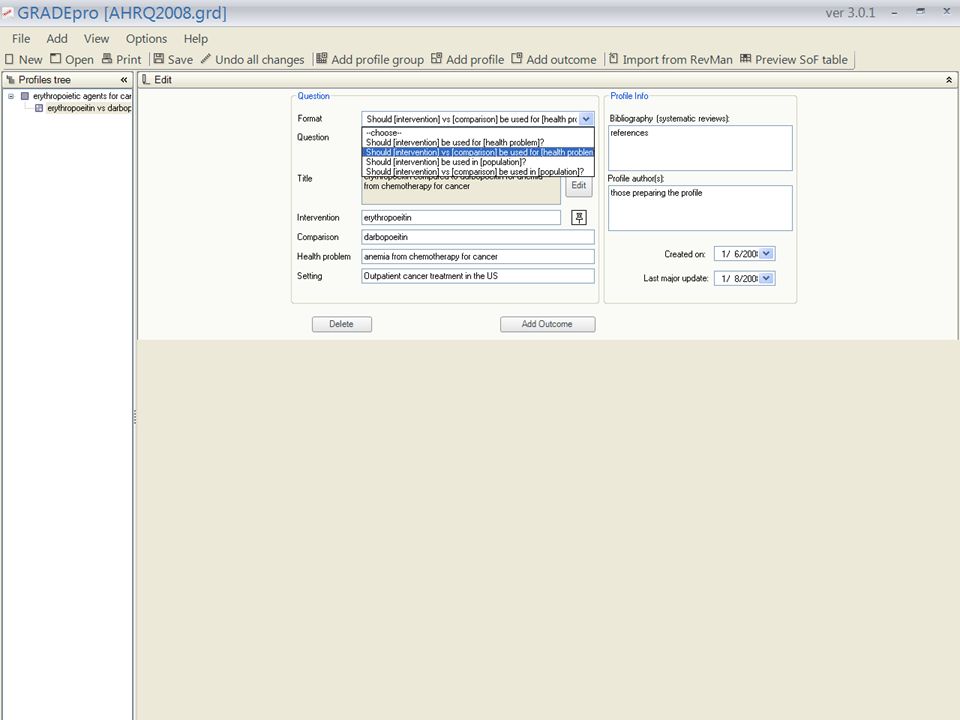
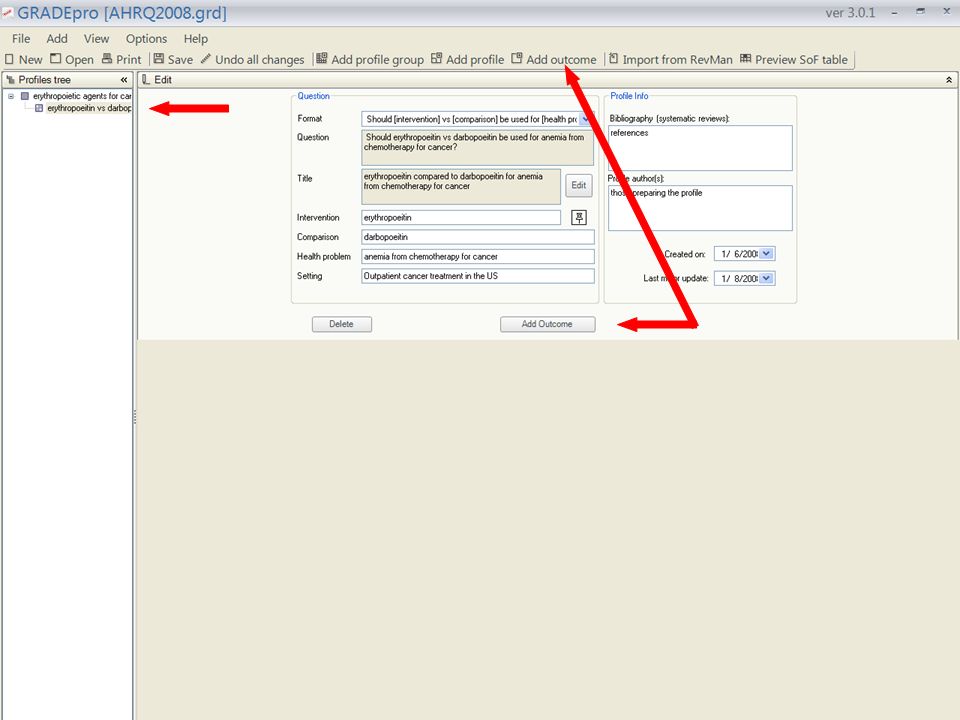
Profiles: Questions

59
Importing a RevMan 5 file of a systematic review Imported data from RevMan 5 file: outcomes meta-analyses results bibliographic information

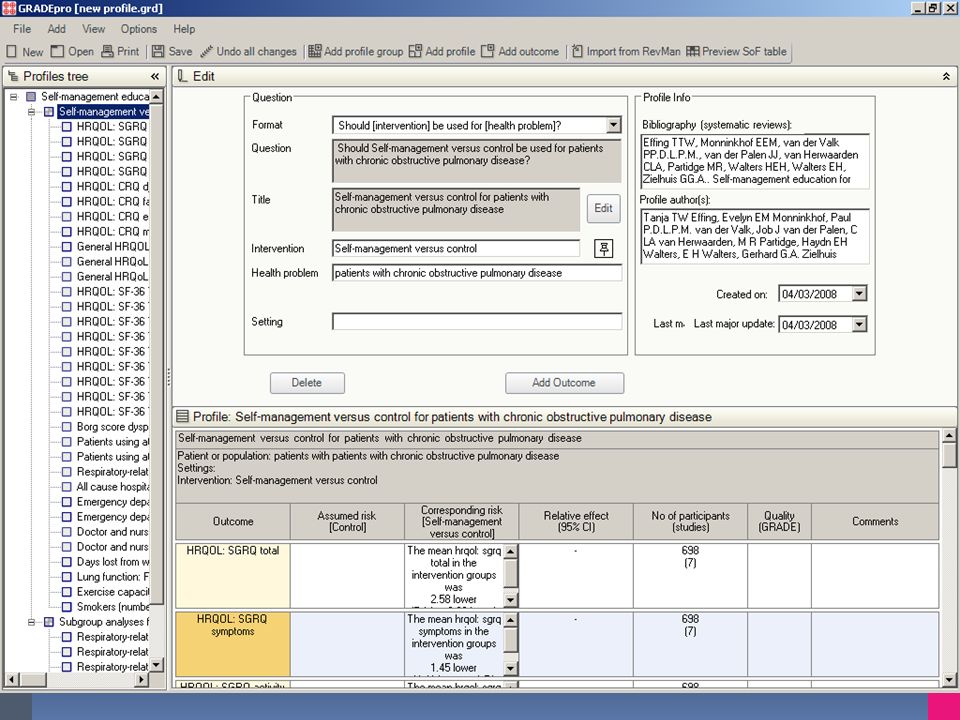
61
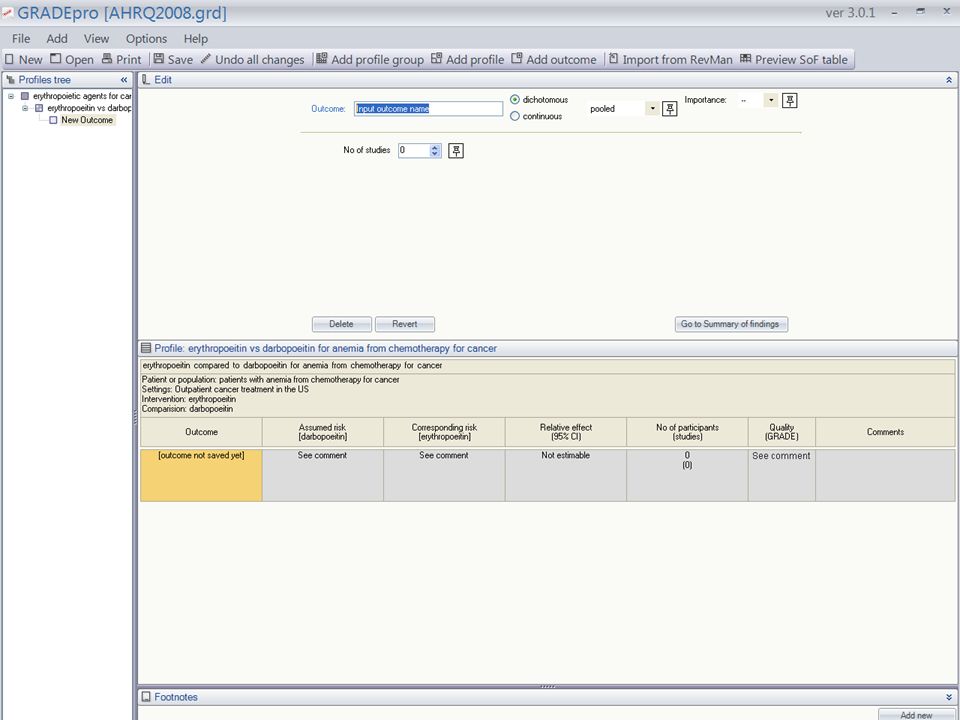
Managing outcomes to include a maximum of 7

62
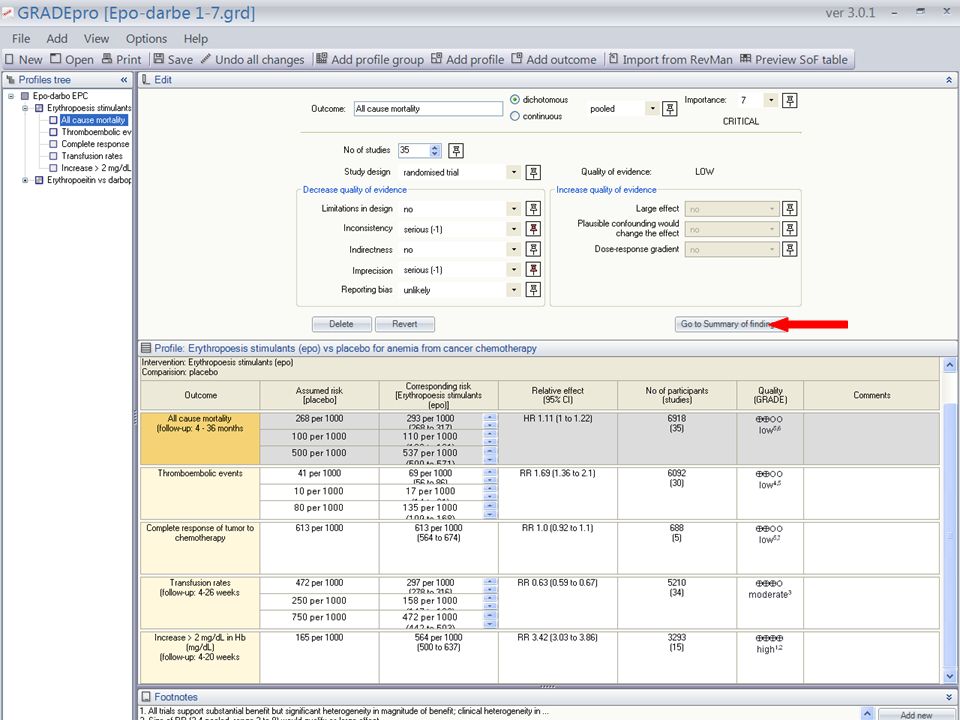
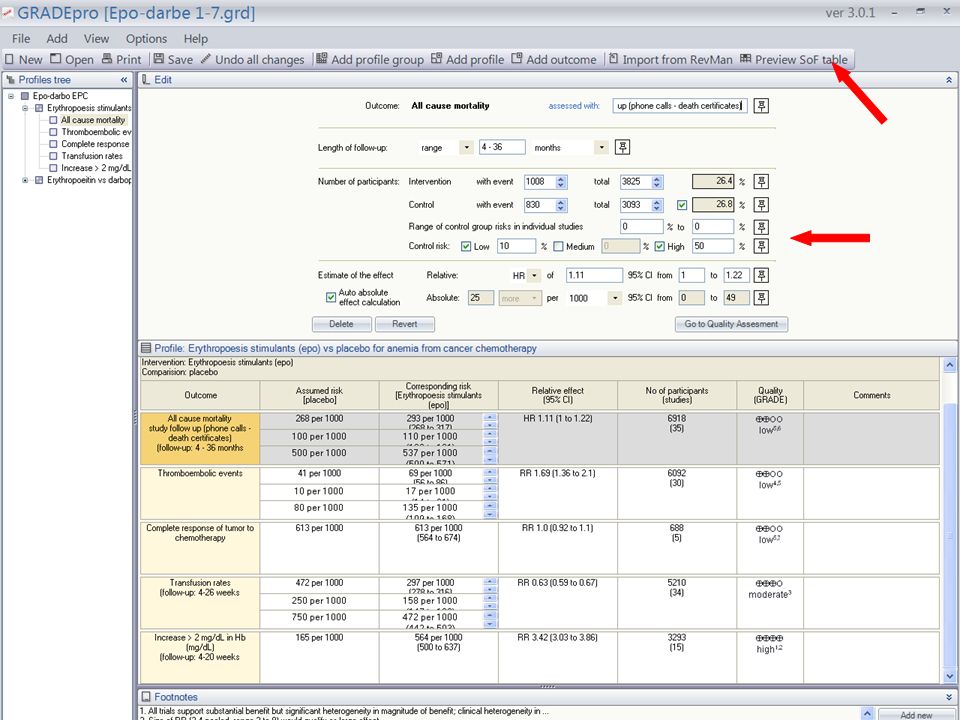
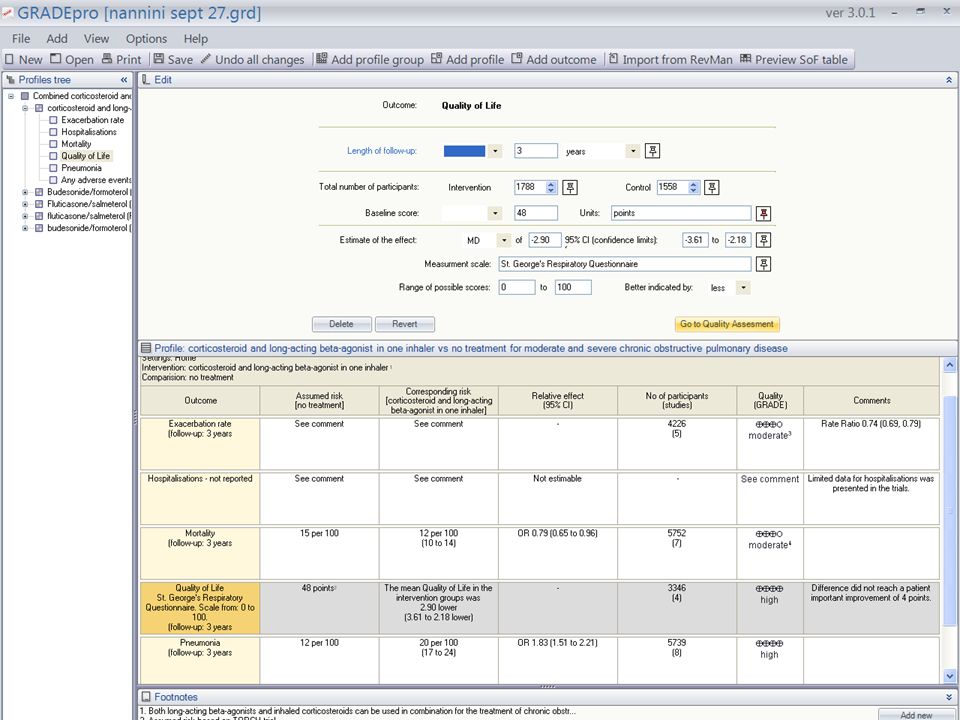
Entering/editing information for dichotomous outcomes

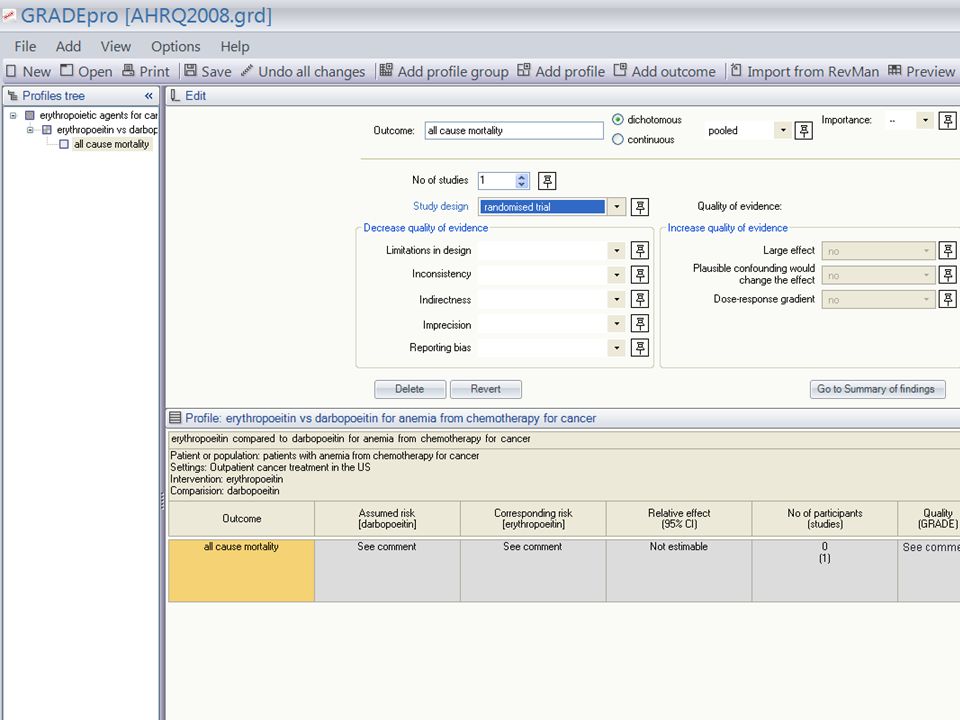
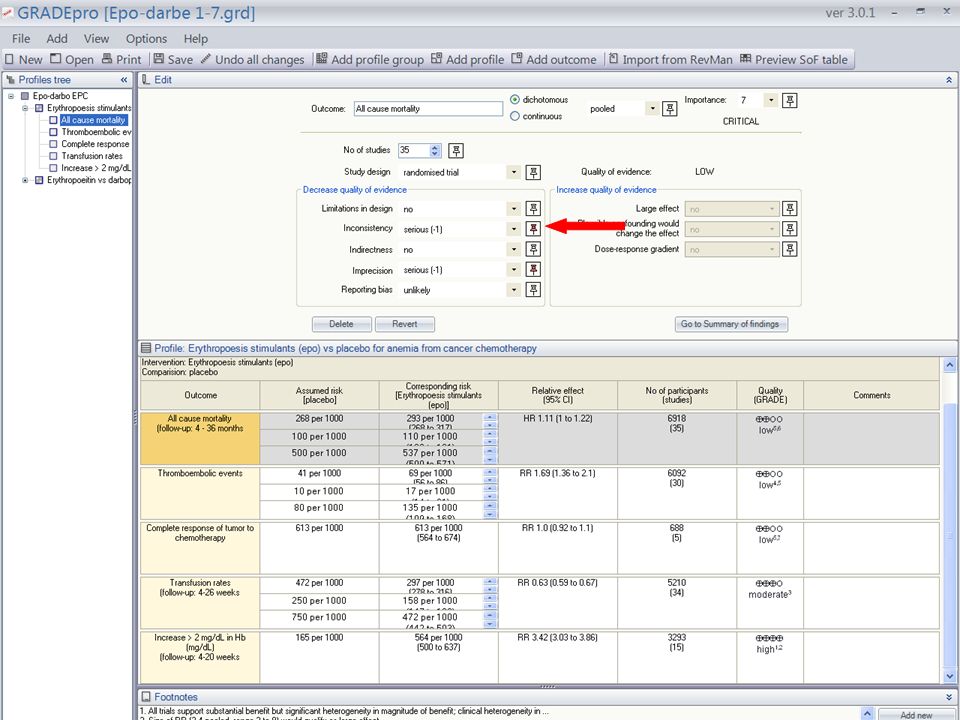
63
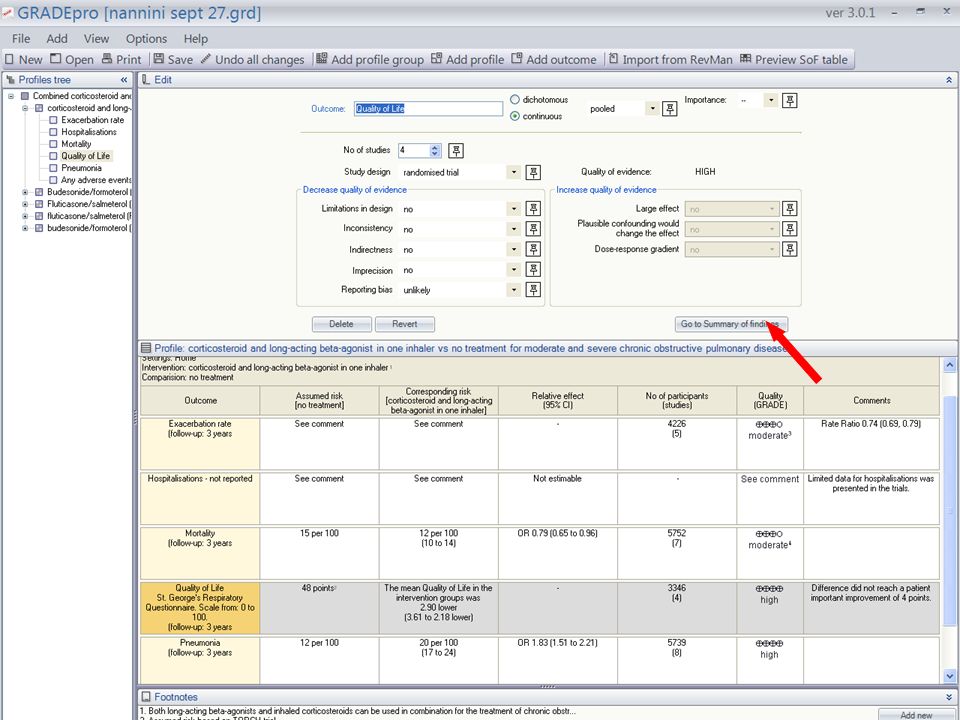
Entering/editing information to grade the quality of the evidence

73
Content Describe the grade of recommendation and what each category means: strong/weak and optional language How the quality of evidence can be upgraded/down-graded What happens when you’re recommending something not be done? Maybe provide some ID-type examples if possible - I’m attaching our clinical questions that may be used as examples? Provide a quick tutorial of GRADEPro Questions

75
Example: Oseltamivir for Avian Flu Recommendation: In patients with confirmed or strongly suspected infection with avian influenza A (H5N1) virus, clinicians should administer oseltamivir treatment as soon as possible (strong recommendation, very low quality evidence). Values and Preferences This recommendation places a high value on the prevention of death in an illness with a high case fatality. It places relatively low values on adverse reactions, the development of resistance and costs of treatment. Remarks Despite the lack of controlled treatment data for H5N1, this is a strong recommendation, in part, because there is a lack of known effective alternative pharmacological interventions at this time. Schunemann et al. The Lancet ID, 2007

76
Confidence in evidence There always is evidence “When there is a question there is evidence” Research evidence alone is never sufficient to make a clinical decision Better research greater confidence in the evidence and decisions

77
77 Sequence gen. Allocation concealment Blinding/Masking Intention-to-treat analysis Blinding/Masking Baseline Allocation A B InterventionNo interv. Follow up Outcome Method Random? Selection bias? Performance bias? Attrition bias? Detection bias? Question Factors leading to bias? Can you explain them? P-values and confidence intervals important? CONSENSUS ALWAYS REQUIRED

78
Limitations of existing systems confuse quality of evidence with strength of recommendations lack well-articulated conceptual framework criteria not comprehensive or transparent GRADE unique breadth, intensity of development process wide endorsement and use conceptual framework comprehensive, transparent criteria

79
G rades of R ecommendation A ssessment, D evelopment and E valuation *Grade Working Group. CMAJ 2003, BMJ 2004, BMC 2004, BMC 2005, AJRCCM 2006, BMJ 2008

80
GRADE Working Group David Atkins, chief medical officer a Dana Best, assistant professor b Martin Eccles, professor d Francoise Cluzeau, lecturer x Yngve Falck-Ytter, associate director e Signe Flottorp, researcher f Gordon H Guyatt, professor g Robin T Harbour, quality and information director h Margaret C Haugh, methodologist i David Henry, professor j Suzanne Hill, senior lecturer j Roman Jaeschke, clinical professor k Regina Kunx, Associate Professor Gillian Leng, guidelines programme director l Alessandro Liberati, professor m Nicola Magrini, director n James Mason, professor d Philippa Middleton, honorary research fellow o Jacek Mrukowicz, executive director p Dianne O ’ Connell, senior epidemiologist q Andrew D Oxman, director f Bob Phillips, associate fellow r Holger J Sch ü nemann, professor g,s Tessa Tan-Torres Edejer, medical officer t David Tovey, Editor y Jane Thomas, Lecturer, UK Helena Varonen, associate editor u Gunn E Vist, researcher f John W Williams Jr, professor v Stephanie Zaza, project director w a) Agency for Healthcare Research and Quality, USA b) Children's National Medical Center, USA c) Centers for Disease Control and Prevention, USA d) University of Newcastle upon Tyne, UK e) German Cochrane Centre, Germany f) Norwegian Centre for Health Services, Norway g) McMaster University, Canada h) Scottish Intercollegiate Guidelines Network, UK i) F é d é ration Nationale des Centres de Lutte Contre le Cancer, France j) University of Newcastle, Australia k) McMaster University, Canada l) National Institute for Clinical Excellence, UK m) Universit à di Modena e Reggio Emilia, Italy n) Centro per la Valutazione della Efficacia della Assistenza Sanitaria, Italy o) Australasian Cochrane Centre, Australia p) Polish Institute for Evidence Based Medicine, Poland q) The Cancer Council, Australia r) Centre for Evidence-based Medicine, UK s) National Cancer Institute, Italy t) World Health Organisation, Switzerland u) Finnish Medical Society Duodecim, Finland v) Duke University Medical Center, USA w) Centers for Disease Control and Prevention, USA x) University of London, UK Y) BMJ Clinical Evidence, UK
 Agency for Healthcare Research and Quality, USA b) Children s National Medical Center, USA c) Centers for Disease Control and Prevention, USA d) University of Newcastle upon Tyne, UK e) German Cochrane Centre, Germany f) Norwegian Centre for Health Services, Norway g) McMaster University, Canada h) Scottish Intercollegiate Guidelines Network, UK i) F é d é ration Nationale des Centres de Lutte Contre le Cancer, France j) University of Newcastle, Australia k) McMaster University, Canada l) National Institute for Clinical Excellence, UK m) Universit à di Modena e Reggio Emilia, Italy n) Centro per la Valutazione della Efficacia della Assistenza Sanitaria, Italy o) Australasian Cochrane Centre, Australia p) Polish Institute for Evidence Based Medicine, Poland q) The Cancer Council, Australia r) Centre for Evidence-based Medicine, UK s) National Cancer Institute, Italy t) World Health Organisation, Switzerland u) Finnish Medical Society Duodecim, Finland v) Duke University Medical Center, USA w) Centers for Disease Control and Prevention, USA x) University of London, UK Y) BMJ Clinical Evidence, UK")
81
GRADE Uptake World Health Organization National Institute Clinical Excellence (NICE) Allergic Rhinitis in Asthma Guidelines (ARIA) American Thoracic Society British Medical Journal Infectious Disease Society of America American College of Chest Physicians UpToDate American College of Physicians Cochrane Collaboration Infectious Disease Society of America European Society of Thoracic Surgeons Clinical Evidence Agency for Health Care Research and Quality (AHRQ) Over 20 major organizations
 Allergic Rhinitis in Asthma Guidelines (ARIA) American Thoracic Society British Medical Journal Infectious Disease Society of America American College of Chest Physicians UpToDate American College of Physicians Cochrane Collaboration Infectious Disease Society of America European Society of Thoracic Surgeons Clinical Evidence Agency for Health Care Research and Quality (AHRQ) Over 20 major organizations")
82
The GRADE approach Clear separation of 2 issues: 1) 4 categories of quality of evidence: very low, low, moderate, or high quality? methodological quality of evidence likelihood of systematic deviation from truth by outcome 2) Recommendation: 2 grades – weak/conditional or strong (for or against)? Quality of evidence only one factor Influenced by magnitude of effect(s) – balance of benefits and harms, values and preferences, cost *www.GradeWorkingGroup.org
 Recommendation: 2 grades – weak/conditional or strong (for or against). Quality of evidence only one factor Influenced by magnitude of effect(s) – balance of benefits and harms, values and preferences, cost *")
83
GRADE Quality of Evidence “Extend of confidence on how adequate the estimate of effect is to support decision” high: considerable confidence in estimate of effect. moderate: further research likely to have impact on confidence in estimate, may change estimate. low: further research is very likely to impact on confidence, likely to change the estimate. very low: any estimate of effect is very uncertain

84
Developing recommendations

85
Conclusion clinicians, policy makers need summaries that separate: quality of evidence strength of recommendations explicit rules transparent, informative GRADE four categories of quality of evidence two grades for strength of recommendations transparent, systematic by and across outcomes applicable to diagnosis wide adoption

87
Consistency of results consistency of results if inconsistency, look for explanation patients, intervention, outcome, methods unexplained inconsistency downgrade quality oxygen for day-to-day dyspnea in COPD with exercise hypoxemia five cross-over RCTs oxygen versus placebo 4 no benefit, 1 substantial benefit

88
Evidence profiles

89
Directness of Evidence indirect comparisons interested in A versus B have A versus C and B versus C formoterol versus salmeterol versus tiotropium Acetylcysteine alone for Pulmonary Fibrosis (all that is available is Acetylcysteine + Prednisone + Azathioprine vs. Prednisone + Azathioprine)
.")
90
Directness of Evidence differences in patients (inhalers for mild versus moderate to severe COPD) interventions (all inhaled steroids versus those used in clinical trials – drug class effect) outcomes (long-term health-related quality of life, short – term functional capacity, laboratory exercise, spirometry)
 interventions (all inhaled steroids versus those used in clinical trials – drug class effect) outcomes (long-term health-related quality of life, short – term functional capacity, laboratory exercise, spirometry)")
91
Reporting Bias & Imprecision reporting bias reporting of studies publication bias number of small studies reporting of outcomes small sample size small number of events wide confidence intervals uncertainty about magnitude of effect

92
Differences in exercise capacity in short-term randomized trials of oxygen in COPD patients.

93
What can raise quality? large magnitude can upgrade (RRR 50%) very large two levels (RRR 80%) common criteria everyone used to do badly almost everyone does well Insulin in diabetic ketoacidosis dose response relation (smoking - cancer)
 very large two levels (RRR 80%) common criteria everyone used to do badly almost everyone does well Insulin in diabetic ketoacidosis dose response relation (smoking - cancer).")
94
The clinical scenario A 68 year old male long-term patient of yours. He suffers from COPD but is unable to stop smoking after over 30 years of tobacco use. He has been taking beta-carotene supplements for several months because someone in the “healthy food” store recommended it to prevent cancer. He wants to know whether this will prevent him from getting cancer and whether he should use beta-carotene.

95
The clinical question Population: In patients with COPD Intervention: does beta-carotene suppl Comparison: compared to no suppl. Outcomes: reduce the risk of lung cancer?

96
Where do you look for an answer?

97
Clinical Practice Guidelines Systematically developed statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances Institute of Medicine, 1992

99
Determinants of quality RCTs start high observational studies start low 5 Factors that lower quality (bias) 3 Factors that increase quality (bias is unlikely to explain observed effect) Final quality by outcome: High Moderate Low Very low
 3 Factors that increase quality (bias is unlikely to explain observed effect) Final quality by outcome: High Moderate Low Very low")
100
Design and Execution limitations lack of concealment intention to treat principle violated inadequate blinding loss to follow-up early stopping for benefit 13 RCTs bacterial extract (immunomodulation) for preventing exacerbation unclear concealment of randomization questionable intention to treat inadequate attention to loss to follow-up
 for preventing exacerbation unclear concealment of randomization questionable intention to treat inadequate attention to loss to follow-up")
101
Consistency of results consistency of results if inconsistency, look for explanation patients, intervention, outcome, methods unexplained inconsistency downgrade quality oxygen for day-to-day dyspnea in COPD with exercise hypoxemia five cross-over RCTs oxygen versus placebo 4 no benefit, 1 substantial benefit

102
Directness of Evidence indirect comparisons interested in A versus B have A versus C and B versus C formoterol versus salmeterol versus tiotropium differences in patients (mild versus severe COPD) interventions (all inhaled steroids) outcomes (long-term health-related quality of life, short – term functional capacity, laboratory exercise, spirometry)
 interventions (all inhaled steroids) outcomes (long-term health-related quality of life, short – term functional capacity, laboratory exercise, spirometry)")
103
How should recommendations be formulated and presented? Few written standards exist For strong recommendations, the GRADE working group has suggested adopting terminology such as, “We recommend…” or “Clinicians should…”. For weak recommendation, they should use less definitive wording, “We suggest…” or “Clinicians might…”.

104
Clinicians and patients want to know! 1) UpToDate ® Users 2) Mini Medical School attendees*: Participants preferred to know about the uncertainty relating to outcomes of a treatment or a test more interested in knowing about uncertainty relating to benefits than harms (96% vs. 90%; P<0.001). strong preference to be informed about the quality of evidence that supports a recommendation. *Akl et al. J Clin Epi, 2007, in press
 UpToDate ® Users 2) Mini Medical School attendees*: Participants preferred to know about the uncertainty relating to outcomes of a treatment or a test more interested in knowing about uncertainty relating to benefits than harms (96% vs. 90%; P<0.001). strong preference to be informed about the quality of evidence that supports a recommendation. *Akl et al. J Clin Epi, 2007, in press.")
105
GRADE Quality of Evidence Extent to which confidence in estimate of effect adequate to support decision high: considerable confidence in estimate of effect. moderate: further research likely to have impact on confidence in estimate, may change estimate. low: further research is very likely to impact on confidence, likely to change the estimate. very low: any estimate of effect is very uncertain

106
There always is evidence The better the research and the evidence, the more confident the decision Evidence alone is never sufficient to make a clinical decision

107
Do evidence based guidelines make a difference? Non-rigorous guidelines: Create noise & bias Make more aggressive recommendations Can harm patients and impair research efforts Can reduce credibility of professional societies Evidence-based clinical practice guidelines can: reduce delivery of inappropriate care support introduction of new knowledge into clinical practice Grimshaw et al (1992); Woolf et al (1999); Fretheim et al (2002)
; Woolf et al (1999); Fretheim et al (2002).")
Similar presentations









 Director of Evidence-Based Practice, Quality Management Assistant.>")


 Methodology.>")





 Working Group www.gradeworkinggroup.org.>")




