Download presentation
Presentation is loading. Please wait.

1
Epilepsy In children with Cerebral Palsy Epilepsy In children with Cerebral Palsy By Dr. Asia Mulhi

6
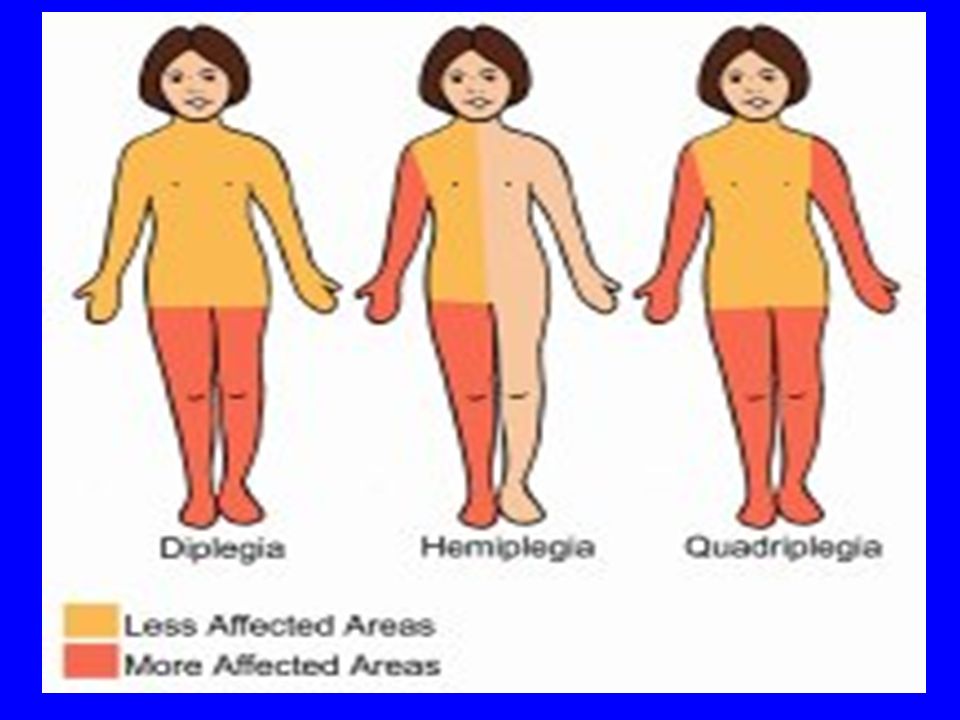
Introduction Cerebral palsy is a term that define a group of non progressive but often changing syndromes of motor impairment secondary to a lesions of motor impairment secondary to a lesions or anomalies of the brain often arising in the or anomalies of the brain often arising in the early stages of its development. early stages of its development. The incidence of CP range from 1.5- 2.5 per 1000 live births 1000 live births

7
A range of 15-60 % of CP having epilepsy. Their epilepsies tend to be persistent. Cerebral palsy who have mental retardation tend to have higher incidence of epilepsy. tend to have higher incidence of epilepsy. Higher risk of seizure relapse have been observed in children with cerebral palsy.

8
Objectives General : To evaluate the epilepsy in children with Cerebral Palsy Specific ; Specific ; To determine the frequency of epilepsy in relation to types of CP. To identify : - -factors associated with epilepsy in children with cp - children with cp in relation to age at seizure onset. - types of seizures in children with cp. - Seizure outcome in children with cp.

9
Methods Prospective and analytic study reviewed epilepsy in children with cerebral palsy Setting : study was conducted in Alwahda teaching hospital / ADEN Period of study : January 2000 to Dec. 2003 Study population : 100 children with CP were seen in neurology out-patient 50 of CP with seizures were studied ( group 1)
.")
10
A control group of 50 epileptic children with normal neurodevelopment studied during the same period (group 2). Period of follow up was at least two years. Data were obtained from parents, patients as: type of CP, type of epilepsy, age of epilepsy onset, family history of seizure, history of neonatal seizures, history of status epilepticus, presence of mental retardation, brain C T scan findings, interictal EEG data, use of anti epileptic drugs and seizure outcome.

11
Evaluation of mental subnormality based on clinical assessment,neurological exam. Speech, or need for special education Seizure outcome was defined as good if patient was seizure free for 2 years or more and poor for seizure recurrence daily,weekly and poor for seizure recurrence daily,weekly or monthly. or monthly. Intractable epilepsy was defined as 2 seizures per month in spite of appropriate therapy with per month in spite of appropriate therapy with maximal tolerable dose maximal tolerable dose

12
Statistical analysis Data was processed by computer facilities, using percentage as summary measure, X 2 test was applied to relate variables among groups and Odd Ratio was calculated with a significant level of 0.05. Data was processed by computer facilities, using percentage as summary measure, X 2 test was applied to relate variables among groups and Odd Ratio was calculated with a significant level of 0.05.

13
Results

14
Table ( 1) frequency of epilepsy by cerebral palsy types Table ( 1) frequency of epilepsy by cerebral palsy types Type of Cp Total CP with epilepsy NO.% Sp tetreplegia 462860 Sp hemiplegia 13646 Sp Diplegia 9444 Dyskinetic17741 Mixed15533 Total10050
 frequency of epilepsy by cerebral palsy types Table ( 1) frequency of epilepsy by cerebral palsy types Type of Cp Total CP with epilepsy NO.% Sp tetreplegia Sp hemiplegia Sp Diplegia 9444 Dyskinetic17741 Mixed15533 Total10050")
15
Table ( 2) Children by groups and associated factors. FactorsEpilepsy With cp Group 1 Epilepsy without CP Group 2 Odd ratio N=50%N=50% X2X2X2X2P Neonatal seizures 16322413.280.000211.3(2.3-76.3) Positive F/H of seizures 112236 5. 32 0.02 4. 4 (1. 03-21.6) Seizures onset during the first year of life 2856612 21. 57 0.000 9.33(3.08- 2.97) Mental subnormality 45903670.70.000 14.1(27.3- 887.1) Status epilpticus 17342414.620.0001 12.4(2.5- 83.3) Need two or more AED 3468153014.450.0001 4.96(1.96- 12.7) EEG abnormalities 459040801.25 0.2626 (Ns) 2.25 Abnormalities on brain imaging 428483229.00.0000 29.8(6.1- 169.1)
 Positive F/H of seizures ( ) Seizures onset during the first year of life ( ) Mental subnormality ( ) Status epilpticus ( ) Need two or more AED ( ) EEG abnormalities (Ns) 2.25 Abnormalities on brain imaging ( ).")
16
Table(3 ) Children with epilepsy and cerebral palsy by age at seizure onset at seizure onset Types of CP Epilepsy With cp Group 1 Group 1N=50 Epilepsy without CP Group 2 N=50 Age(years)SpasticTetraplegiaSpasticHemiplegiSpasticDiplegiaDysk.Mix <12175%116%0228%480%2856%612% 1-6621%233%375%457%120%1632%1938% >61 3.5% 3.5%350%125%114%0612%2550% X 2 :26.14 P :0.000
 Children with epilepsy and cerebral palsy by age at seizure onset at seizure onset Types of CP Epilepsy With cp Group 1 Group 1N=50 Epilepsy without CP Group 2 N=50 Age(years)SpasticTetraplegiaSpasticHemiplegiSpasticDiplegiaDysk.Mix <12175%116%0228%480%2856%612% %233%375%457%120%1632%1938% >61 3.5% 3.5%350%125%114%0612%2550% X 2 :26.14 P :0.000")
17
Seizures Types Epilepsy With cp Group 1 Group 1 Epilepsy without CP Group 2 No.%No.% Generalized T+C 19381530 Partial /complex, sec general. 11221836 Myoclonic816612 Infantile spasms 4824 Atonic0036 Absence (TYPICAL) 0048 Polymorphic91824 Table (4) Children of epilepsy by types of seizure
 0048 Polymorphic91824 Table (4) Children of epilepsy by types of seizure.")
18
Graph(2) children with cerebral palsy by seizure types
 children with cerebral palsy by seizure types")
19
Table No. ( 5) Children with CP and Epilepsy and Epilepsy without CP by Seizure outcome. Seizure outcome Epilepsy With cp Group 1 Epilepsy without CP Group 2 No.%No.% Good19383876 Poor31621224 Total5010050100

20
Seizure outcome Epilepsy With cp Group 1 Epilepsy without CP Group 2 X 2 p-value Intractable 31( 62%) 12 ( 24 % ) 14.7 0.001 Controlled 19 (38%) 38 ( 76%) 22.2 0.000 Discontinuation of AEDs 11 (22%) 35 (70%) 14.9 0.0001 Monotherapy 16 (32%) 35 (70%) 14.50 0.0001 polytherapy 34 (68%) 15 (30%) 14.5 0.0001 Table (6) Children with epilepsy by seizure outcome
 12 ( 24 % ) Controlled 19 (38%) 38 ( 76%) Discontinuation of AEDs 11 (22%) 35 (70%) Monotherapy 16 (32%) 35 (70%) polytherapy 34 (68%) 15 (30%) Table (6) Children with epilepsy by seizure outcome")
21
Table (7) seizure outcome in children with cerebral palsy by types of CP Seizure outcome. Types of CP Types of CP Epilepsy With CP Group 1 Epilepsy EpilepsywithoutCP Group 2 Spastic Tetraplegia. DyskineticMixed.spasticHemiplegiaSpastic Diplegi a Good635%342%240%466.7%4100%19 38 % 38 3876% poor2278.6%457.1%360%233.3%03162% 12 1224% X 2 14.7 P :0.0001

22
Table (8 ) Intractable epilepsy in children with cerebral palsy and Antiepileptic drugs (AED). Type of CP TotalIntractableepilepsy Controlled epilepsy Discontinua -tion of AEDs Mono- therapy Poly- therapy SpasticTetraplegia 28 22 (78%) 6 (35%) 4 (14% ) 7(25%) 21(75%) Dyskinetic 7 4 (57%) 4 (57%) 3 (42 %) 0 (0.0 %) 1(14 %) 6(85% ) Mixed 5 3 (60%) 2 (40%) 0 (0.0 %) 0 5(100% ) SpasticHemiplegia 6 2 ( 33%) 4(66%) 4 (66% ) 5(83% ) 1( 16%) Spastic Diplegia 40 4 (100%) 3 (75%) 1(25%) Total 50 31 (62%) 19 (38%) 11 (22%) 16 (32%) 34 (70%)
 6 (35%) 4 (14% ) 7(25%) 21(75%) Dyskinetic 7 4 (57%) 4 (57%) 3 (42 %) 0 (0.0 %) 1(14 %) 6(85% ) Mixed 5 3 (60%) 2 (40%) 0 (0.0 %) 0 5(100% ) SpasticHemiplegia 6 2 ( 33%) 4(66%) 4 (66% ) 5(83% ) 1( 16%) Spastic Diplegia 40 4 (100%) 3 (75%) 1(25%) Total (62%) 19 (38%) 11 (22%) 16 (32%) 34 (70%).")
23
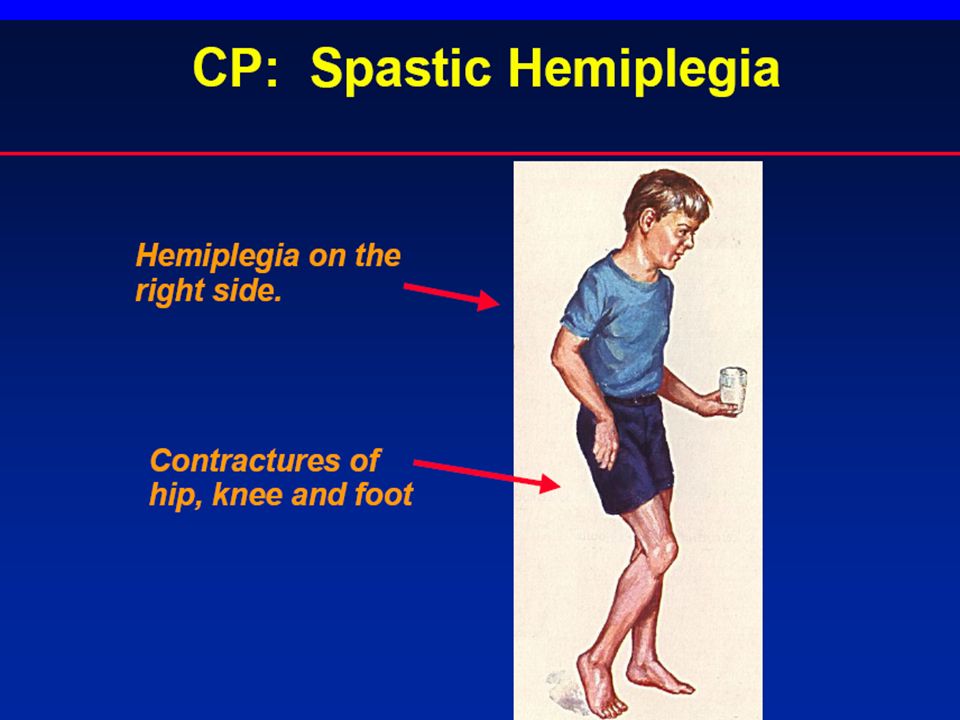
Conclusion The incidence of epilepsy was higher in tetraplegic cerebral palsy. Intellectual impairment, history of neonatal seizures, earlier age of seizure onset, status epilepticus,abnormal brain imaging finding and need for polytherapy were associated factors in cerebral palsy. Epilepsy in CP was associated with earlier age of seizure onset than that in control group.

24
Generalized seizure was predominant form of seizures in children with CP, and all infantile spasms were observed among tetraplegic patients. of seizures in children with CP, and all infantile spasms were observed among tetraplegic patients. Better seizure outcome was associated with normal intelligence, single seizure type,monotherapy, spastic diplegia. Fewer children with CP were able to discontinue Anti-epileptic drugs, and non of children with infantile spasms or polymorphic seizure achieved a seizure free period of more than one year.

25
Recommendations Further studies concerning risks of epilepsy development and its relations with the EEG and brain imaging are needed. Trial of AEDs discontinuation after at least two years free of seizures should be practiced in CP patient when possible. Early treatment for epilepsy in patients with cerebral palsy recommended to avoid further brain damage and more cognitive dysfunction.

28
Thank you

Similar presentations






 The only diagnostic test for absence seizures Ambulatory EEG monitoring over 24 hours may be useful to.>")







 Report of the Quality Standards Subcommittee of the American Academy of.>")


 epilepsie.>")


 The name “Down Syndrome” comes from the facial appearance of afflicted.>")


