Download presentation
Presentation is loading. Please wait.

1
REGIONAL ANESTHESIA Anesthesia Care Teams and Block Areas NAPAN Conference Sue Belo MD PhD FRCPC May 23rd, 2009

2
HOLLAND CENTRE

3
The Holland Centre AMALGAMATION 1998 Orthopedic and Arthritic Hospital Sunnybrook Hospital Orthopedic and Arthritic Institute SWCHCS Holland Centre 2005

4
Resources 4 Operating Rooms 5 bay Post Anesthesia Care Unit 10 bay Same Day Admission Area 5 Anesthetists (OR and Pre-assessment) 50 Acute Care Beds 20 Short term Rehab Beds
 50 Acute Care Beds 20 Short term Rehab Beds")
5
2004 3200 cases per year 1500 total joint arthroplasties 100% under General Anesthesia Limited use of femoral nerve blocks Post-op nurse-managed morphine PCA

6
2004 Average length of stay 7 days In-patient rehab 10 days 20% to long term rehab 16 days

7
2004 Average 16/20 lists per month ran overtime Average overtime 30 hours/month Average 18 cancellations/month

8
How can patient care be improved at the Holland Centre? Wait Time strategy 2004 Holland Centre of Excellence Aug 2005 Anesthesia and Nursing shortages

9
Regional Anesthesia 4-fold reduction in mortality with regional compared to GA (Shamrock et al 1995) decreased DVT/PE; decreased blood loss and transfusion rate (Mauermann et al 2006) better pain control and decreased opioid use (Salinas et al 2006) improved surgical outcomes (Peters et al 2006)
 decreased DVT/PE; decreased blood loss and transfusion rate (Mauermann et al 2006) better pain control and decreased opioid use (Salinas et al 2006) improved surgical outcomes (Peters et al 2006)")
10
VISION Convert the Holland Centre to Regional Anesthesia

11
Regional Anesthesia at the Holland Centre better patient care decrease overtime and cancellations through increased efficiency ability to increase volume of cases increase nursing satisfaction increase recruitment and retention

12
prolonged operating room time decreased efficiency unpredictable success rate inferior surgical conditions unacceptable to patients CHANGE!!

13
Anesthesia Concerns Regional Anesthesia requires time Regional Anesthesia requires expertise Regional Anesthesia requires co-operation Regional Anesthesia requires a team effort Investment for Improvement

14
Administration Concerns $$$$$$

15
Anesthesia Care Team Model Create a separate but adjacent “Block Area” (4 bays) “ Block RNs” to staff area (2) – check patients, prepare equipment, monitor patients Anesthesia Assistants (2) – monitor stable patients under regional anesthesia in OR while anesthetist performs regional/blocks for next patient Anesthesiologists (4) – each anesthesiologist does own blocks in the Block Area
 Block RNs to staff area (2) – check patients, prepare equipment, monitor patients Anesthesia Assistants (2) – monitor stable patients under regional anesthesia in OR while anesthetist performs regional/blocks for next patient Anesthesiologists (4) – each anesthesiologist does own blocks in the Block Area")
16
Patient Flow OR Same Day Admission Block Area PACU

17
2007

19
Surgeon Education Approached surgeons individually and as a group Provided relevant literature (including surgical literature) Presented rounds
 Presented rounds")
20
Nursing Education Involved Pre-Assessment Clinic nursing staff, ward nurses, OR nurses Provided with literature, in-services Invited to Block Area and PACU

21
Allied Health Professionals educational sessions for Physiotherapy feedback from Physiotherapy on issues in regards to rehab revision of practice and protocols to address concerns with hypotension, prolonged motor block, etc. consultation with Pharmacy re pre-op medications, pre-printed orders

22
Patient education by anesthetist at pre-op visit patient information pamphlets DVD video sent home with patient Web-site

23
Post-operatively established an Acute Pain Service under the direction of Nurse Practitioner and a dedicated anesthesiologist (Nov 2005) developed best practices for post-op pain management (epidural analgesia, PCEA, oral analgesia protocols for THR, multi-modal analgesia regimens)
 developed best practices for post-op pain management (epidural analgesia, PCEA, oral analgesia protocols for THR, multi-modal analgesia regimens)")
24
Developed protocols and standardization for selected procedures initially and introduced new procedures slowly – Spinal Anesthesia for THR and TKR – Femoral Nerve Blocks for TKR – Sciatic Nerve Blocks for TKR – Combined spinal epidural anesthesia for bilateral TKR – Peripheral nerve block catheters

25
2007 2100 total joint arthroplasties Neuraxial anesthesia in 90% Peripheral nerve blocks used in 90% of TKA Peripheral nerve block catheters for continuous infusions

26
OR Time 17% decrease in time for patient-in to patient-out from 2004 to 2007 in total knee arthroplasties 18.6% decrease in time required from patient-in to patient-out for total hip arthroplasties

27
OR Overtime (* cancellations)
")
28
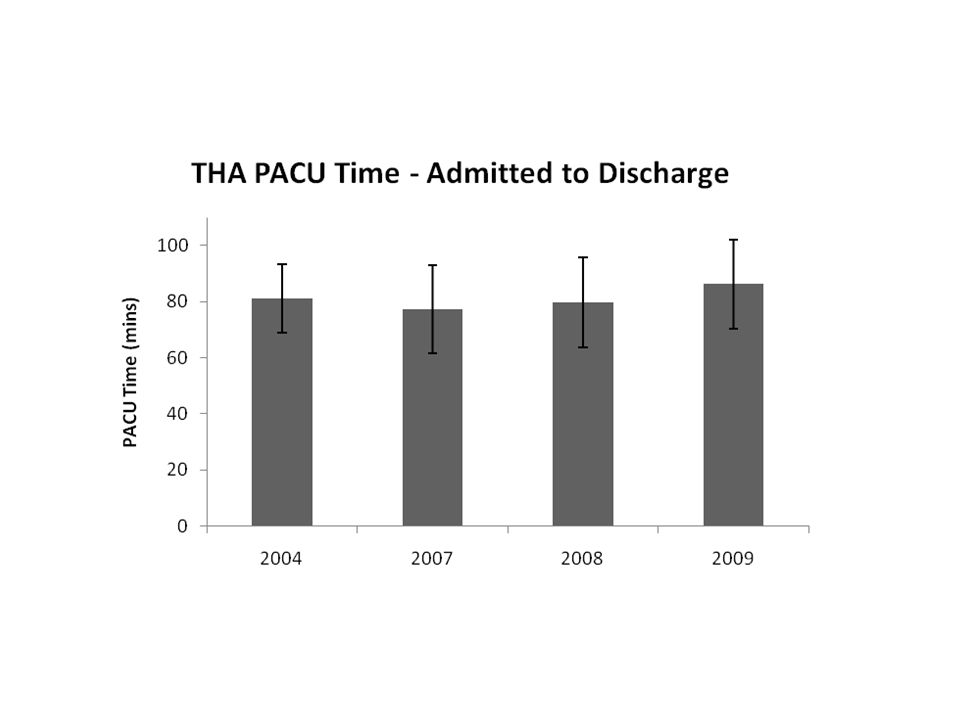
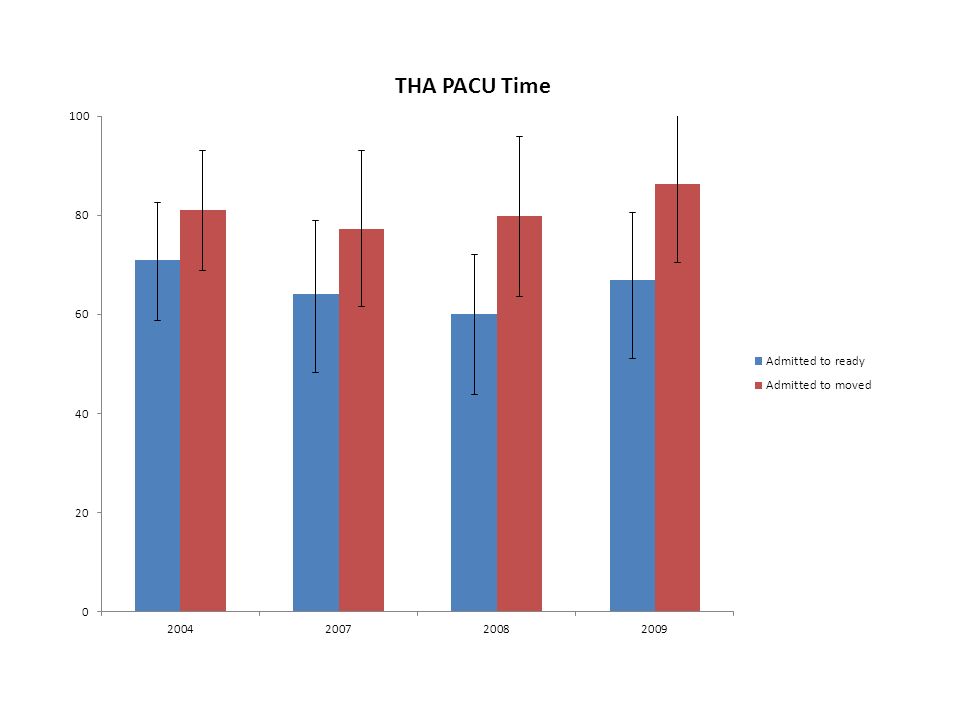
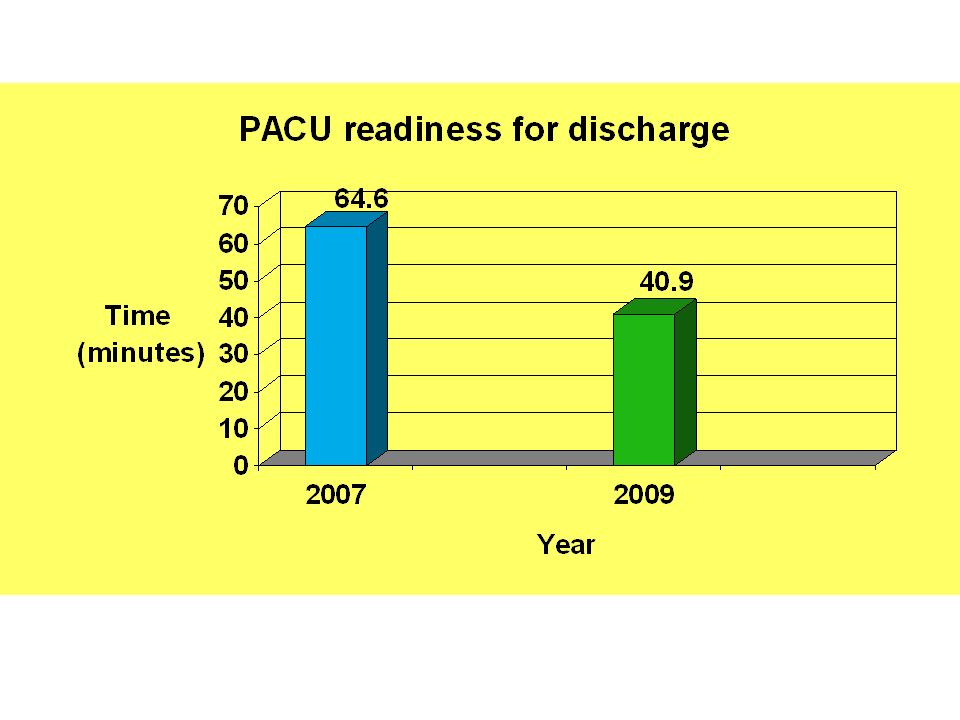
PACU Length of Stay

29
Average LOS 4.8 days 67% discharged home (day 5) 24% short term in-pt rehab- 5 days (day 3) 9% longer in-pt rehab
 24% short term in-pt rehab- 5 days (day 3) 9% longer in-pt rehab")
30
Anesthesiologist’s Perspective Changes in anesthetic practice facilitated improved efficiency and “fast-tracking” Improvement in global peri-operative care No incremental risk for patients Improved outcomes Benefits for patients, physicians, nurses, allied health care practitioners No additional Anesthesia resources required

35
PACU Discharge Criteria Modifications for Spinal Anesthesia sensory block level at a minimum of T8 recession of sensory block by at least one dermatome level any patient admitted to PACU with a sensory block at T10 or below and some movement of the lower extremities may be discharged from PACU

37
The Future Improved patient care Continuous catheters Patient controlled oral analgesia Expanded ultrasound applications Optimization of drugs and dosages Best Practice guidelines Expansion of Anesthesia Care Team model

38
Retainment and Recruitment (Anesthesiologists, Block RNs, Anesthesia Assistants) Documenting improved outcomes Continuous improvement Expansion of program to Sunnybrook site Maintaining expertise at 2 sites
 Documenting improved outcomes Continuous improvement Expansion of program to Sunnybrook site Maintaining expertise at 2 sites")
39
THANK YOU

Similar presentations





















.>")
