Download presentation
Presentation is loading. Please wait.

1
INTRALIPIDS AS RESCUE 2:30-3:30

2
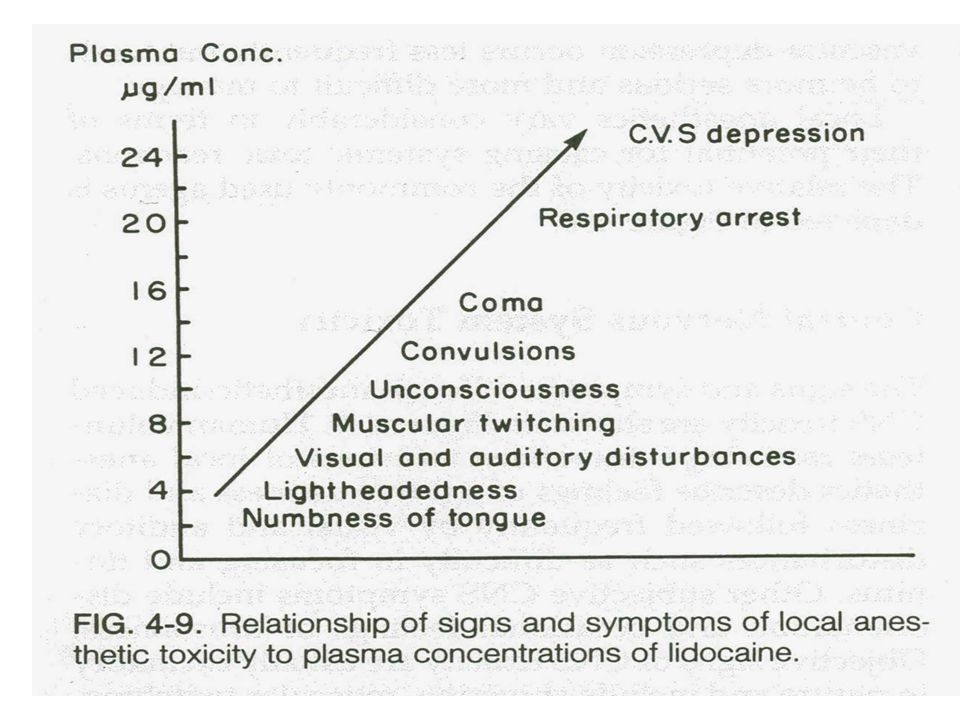
Objectives Describe signs and symptoms of local anesthetic (LA) toxicity. Identify treatment modalities including use of lipids for patients with LA toxicity. Identify factors influencing LA toxicity.

3
Mechanism of action Loss of sensation by – inhibiting excitation at nerve endings – blocking conduction in peripheral nerves Progression of anesthesia related to affected nerve fiber: – diameter – myelination – conduction velocity Prevent the development of action potential in nerve

4
Regional Anesthesia Involves the use of a local anesthetic strategically placed along the neural access to produce: – Surgical anesthesia – Postoperative analgesia – Analgesia for acute & chronic pain management Goal: Block conduction of nociceptive (pain) impulses
 impulses")
5
LOCAL AGENTS Levels dependent on: – Dose – Rate of injection – Specific gravity of fluid – Position of patient

6
LOCAL AGENTS ESTERS – Hydrolyzed in Plasma – Unstable in solution – Poor Penetrance – Fair to Poor Stability EXAMPLES Cocaine – (1884) Procaine - (Novacain) – 1984 Chloroprocaine - (Nesacaine) Tetracaine- (Pontocaine) - 1931
 Procaine - (Novacain) – 1984 Chloroprocaine - (Nesacaine) Tetracaine- (Pontocaine)")
7
LOCAL AGENTS AMIDES – Metabolized by Liver – Stable Good Penetrance Lidocaine - (Xylocaine) Mepivacaine - (Carbocaine) Prilocaine - (Citanest) Bupivacaine - (Marcaine, Sensorcaine) Etidocaine Ropivacaine
 Mepivacaine - (Carbocaine) Prilocaine - (Citanest) Bupivacaine - (Marcaine, Sensorcaine) Etidocaine Ropivacaine")
8
LOCAL AGENTS Epinepherine Added to Local – Vasoconstriction – Slows Vascular Absorption – Prolongs Effect

9
Local Anesthesia Toxicity Agents used in excessive doses or administered improperly. Repetitive (small) doses to achieve an adequate level of anesthesia may lead to eventual administration of toxic dose. Anesthesia injected into confined space Doses may inadvertently be delivered as intravascular injection rather than epidurally
 doses to achieve an adequate level of anesthesia may lead to eventual administration of toxic dose. Anesthesia injected into confined space Doses may inadvertently be delivered as intravascular injection rather than epidurally.")
10
Local Anesthesia Toxicity Administration of toxic doses of LA – Increase disruptions of cellular metabolism – Interfere with inotropic function pathways that regulate NA+, K+ and Cl- ion flow – Modulation of autonomic system and enzymatic processes for ATP formation

11
Toxicity Early: agitation, lightheadedness, altered mental state, visual changes, slurred speech, hypertension and tachycardia Middle: CNS excitation, cardiac dysrhythmias, contractile depression & conduction blockade. Seizure ( 20-30 minutes) Severe: Hypotension, bradycardia, Ventricular dysrhythmia and cardiovascular collapse
 Severe: Hypotension, bradycardia, Ventricular dysrhythmia and cardiovascular collapse.")
13
CNS Toxicity Sedation CNS excitation at low drug concentration Dizziness, ringing in the ear, Metallic taste Paresthesia (circumoral tingling) Anxiety Fear of death Uncontrolled muscle activity Tonic –clonic seizures CNS depression Bupivacaine ( CNS & Cardiac toxicity simultaneously
 Anxiety Fear of death Uncontrolled muscle activity Tonic –clonic seizures CNS depression Bupivacaine ( CNS & Cardiac toxicity simultaneously")
14
Cardiovascular Toxicity Block of sodium, calcium and potassium channels Difficult to resuscitate on patient with asystole with Bupivacaine toxicity due to long term Bupivacaine is cardiotoxic, strong attraction to myocardial sodium channel, slow dissociation from the sodium channels due to its lipophilic properties.

15
Management of Local Anesthesia Toxicity ACLS protocol – Airway – Vital Signs – Resuscitative Medications

16
Chance Observation Noted that patient with carnitine deficiency exhibited sensitivity to bupivacaine induced cardiac dysrhythnias, therefore postulated that bupivacaine might interfere with carnitine metabolism. Carnitine = essential component of biochemical pathways that transport fatty acids into mitochondria where they provide the majority of cardiac energy needs. Interestingly enough, the opposite was discovered – infusing lipids made them more resistant to bupivacaine-induced asystole. Lipid infusion improves the success of resuscitation from bupivacaine toxicity.

17
2006 Case 17 year old developed seizure activity and CV collapse after intentional ingestion. Ingested: Bupropion (Antidepressant) and Lamotrigine (Anticonvulsant) Unsuccessful resuscitation attempts for 70 minutes 100 ml IV bolus of 20% lipid emulsion given After 1 minute, an effective sustained pulse was observed. Patient recovered with no major neurologic deficit.
 and Lamotrigine (Anticonvulsant) Unsuccessful resuscitation attempts for 70 minutes 100 ml IV bolus of 20% lipid emulsion given After 1 minute, an effective sustained pulse was observed. Patient recovered with no major neurologic deficit..")
18
91 year old History: COPD, HTN, CAD, Reflux Infraclavicular brachial plexus block for olecranon bursa excision. Given 1% mepivicaine 30 ml 20 min after injection was then injected with 10 ml 1% Prilocaine. 5 minutes after injection of prilocaine, (20 min after patient received the Mepivicaine) patient developed dizziness, nausea, agitation & then lost consciousness Given 1ml/kg bolus of 20% intralipid followed by infusion and patient recovered within minutes and surgery proceeded.
 patient developed dizziness, nausea, agitation & then lost consciousness Given 1ml/kg bolus of 20% intralipid followed by infusion and patient recovered within minutes and surgery proceeded..")
19
60 year old male with CAD, diabetes and end-stage renal disease For Supraclavicular Brachial plexus block he received: – 30 ml 1.5% mepivacaine with bicarbonate and epi – 10 ml 0.5% bupivacaine Developed labored respiration followed by obtundation 5 min after injection CPR without re-establishment of effective cardiac rhythm Given 20% lipid (250 ml over 30 min) patient recovered
 patient recovered")
20
Local Anesthetic Systemic Toxicity (LAST) requiring treatment 20 out of 10,000 peripheral nerve blocks 4 out of 10,000 epidural blocks Initial symptoms of LA Overdose – Mild hypertension – Tachycardia – Mild agitation – Confusion
 requiring treatment 20 out of 10,000 peripheral nerve blocks 4 out of 10,000 epidural blocks Initial symptoms of LA Overdose – Mild hypertension – Tachycardia – Mild agitation – Confusion")
21
Cardiac Toxicity Hypotension Atrioventricular conduction delay Idioventricular rhythms Respiratory depression Cardiovascular collapse

22
Local Anesthetic Toxicity Can occur after ingestion IV administration Topical Administration

23
Checklist for Treatment of LAST (ASRA & Pain Medicine) Get Help Initial focus – Airway management – Seizure suppression ( Benzodiazepines NOT Propofol) – Alert nearest facility having Cardiopulmonary bypass capability Manage cardiac dysrhymias – BLS & ACLS – Avoid Vasopressin, Calcium channel blockers, beta blockers and local anesthetics – Reduce epinepherine doses to <1mcg/kg
 Get Help Initial focus – Airway management – Seizure suppression ( Benzodiazepines NOT Propofol) – Alert nearest facility having Cardiopulmonary bypass capability Manage cardiac dysrhymias – BLS & ACLS – Avoid Vasopressin, Calcium channel blockers, beta blockers and local anesthetics – Reduce epinepherine doses to <1mcg/kg")
24
Checklist for Treatment of LAST (ASRA & Pain Medicine) Lipid emulsion therapy (20%) – Bolus 1.5 ml/kg IV over 1 minute – Continuous infusion 0.25 ml/kg/min – Repeat bolus once or twice for persistent CV collapse – Double the infusion rate to 0.5 ml/kg/min if BP low – Continue infusion for at least 10 min after attaining circulatory stability – Recommend upper limit: 10ml/kg/lipid emulsion over 30 min. Post LAST events at www.lipidrescue.org or www.lipidregistry.orgwww.lipidrescue.org www.lipidregistry.org

25
Lipid Sink Expanded plasma lipid compartment that traps lipophilic drugs Infused intravascular lipid mass binds the offending toxin in sufficient quantity to pull drug from the target tissue, thereby reversing the toxicity. Successful resuscitation suggest the efficacy of lipid emulsion infusion for treating non-local anesthetic overdoses across a wide spectrum of drugs: beta blockers, calcium channel blockers, parasiticides, herbicides and several varieties of psychotropic agents.

26
2 Proposed methods of How Intralipids Work 1. Lipid infusion creates a lipid phase in the plasma to which local anesthetics partition into. 2. Reversal of mitochondrial fatty acid transport inhibition – Believed LA inhibit carnitine acylcarnitine translocase (CACT) – an enzyme used in mitochrondrial fatty acid metabolism and transport – Because fatty acids are involved in 80-90% of cardiac adenosine 5-triphosphate (ATP) synthesis, inhibition of CACT may contribute to cardiac toxicity. – Lipid infusion may increase the intracellular fatty acid content enough to overcome the inhibition of the CACT enzyme by the anesthetic.
 – an enzyme used in mitochrondrial fatty acid metabolism and transport – Because fatty acids are involved in 80-90% of cardiac adenosine 5-triphosphate (ATP) synthesis, inhibition of CACT may contribute to cardiac toxicity. – Lipid infusion may increase the intracellular fatty acid content enough to overcome the inhibition of the CACT enzyme by the anesthetic..")
27
Death of woman at a Laser Treatment Center Patient received cream containing 10% Lidocaine and 10% Tetracaine. Patient applied cream over Large areas of skin then wrapped her legs in cellophane which increased the absorption of the drug. Found seizing in her car. Unable to resuscitate

28
Lipid Therapy Side Effect Allergic reaction, headache, somnolence, dizziness, dyspnea, diaphoresis, N&V, hyperthermia and hypercoagulability Thrombocytopenia, jaundice, overloading syndrome, Increased liver function, leucopenia, hepatomegaly, splenomegaly Pulmonary hypertension with long term therapy Yeast infection

29
Conclusions Lipid infusion appears to reverse cardiotoxicity rapidly and is easier than cardiopulmonary bypass. Lipid emulsion is readily available at a much lower cost. Lipid rescue therapy is to be reserved until ACLS procedures have been unsuccessful in cases of local anesthetic toxicity

30
Summary Nurses plan an important role towards a successful outcome for patients with local anesthesia toxicity Know your high risk patients Recognize signs and symptoms of toxicity Have adequate emergency equipment available when resuscitation needs arise Know your facility policy for Local Anesthesia Toxicity

Similar presentations




 rapid onset; shorter acting.>")














