Download presentation
Presentation is loading. Please wait.

1
The Little Brother of Hepatitis B Min Li Andie Lee

2
Case Study – Mr SG 35 year-old male Chronic HBV infection HIV Diagnosed 2006, probably acquired 2001 Homosexual male, partner HIV positive On antiretroviral treatment since diagnosis HIV viral load undetectable, CD4 count 620 Major depression

3
Case Study – Mr SG Presented in September 2008 with 3 weeks of: Malaise, fatigue Nausea, vomiting and diarrhoea Jaundice Dark urine and pale stool No fever or abdominal swelling

4
Case Study – Mr SG Medications Atripla (tenofovir/ emtricitabine/ efavirenz) 1 tablet po daily Sildenafil 50mg po prn Previously worked as a graphic designer, now on disability pension Smoker Crystal methamphetamine
 1 tablet po daily Sildenafil 50mg po prn Previously worked as a graphic designer, now on disability pension Smoker Crystal methamphetamine")
5
Case Study – Mr SG Physical examination Afebrile Jaundiced Spider naevi and palmar erythema No abdominal tenderness, hepatosplenomegaly or ascites

6
Case Study – Mr SG Test21.08.200824.09.200830.09.2008 Bilirubin (<18) μmol/L662334 ALP (30-130) U/L71123135 GGT (<60) U/L29742596 ALT (5-55) U/L2512453781 AST (5-55) U/L244703158 Albumin (38-48) g/L4639 INR (0.9-1.2)-1.01.6 Platelet count (150-400)178170116
 μmol/L ALP (30-130) U/L GGT (<60) U/L ALT (5-55) U/L AST (5-55) U/L Albumin (38-48) g/L4639 INR ( ) Platelet count ( )")
7
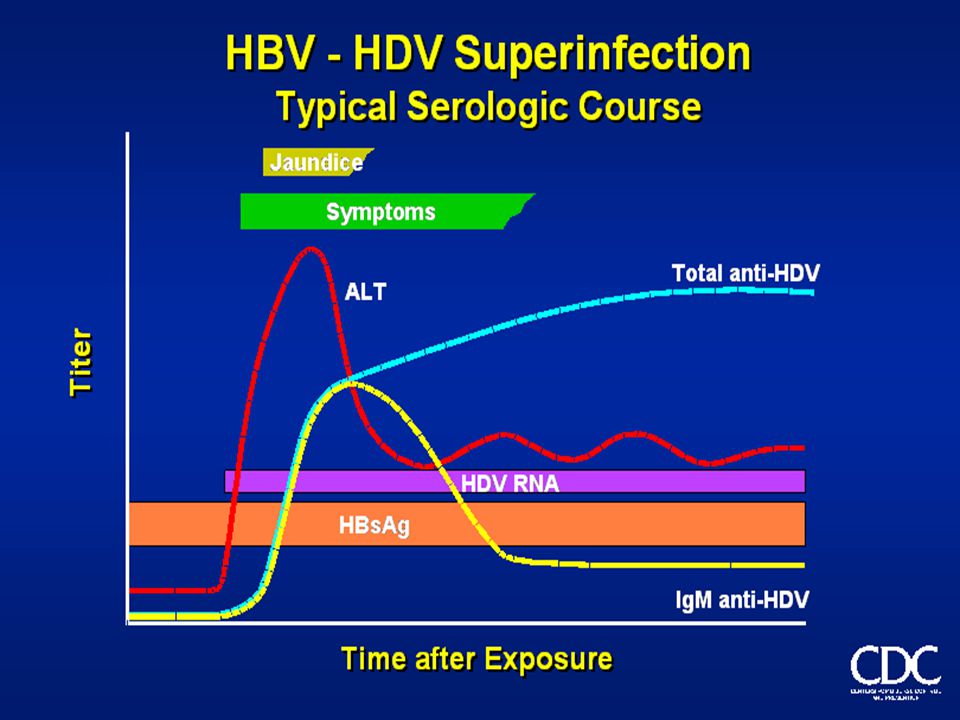
Case Study – Mr SG Hepatitis serology: Hepatitis A IgM –ve, IgG +ve Hepatitis B cAb +ve, B sAg +ve, B eAg –ve HBV concentration 8954 copies/mL (1210 IU/mL) Hepatitis C Ab –ve, HCV PCR –ve Hepatitis D total Ab +ve Hepatitis E IgM –ve, IgG –ve HDV superinfection Superinfection can lead to fulminant hepatitis Mortality rate for HDV infection is 2-20%
 Hepatitis C Ab –ve, HCV PCR –ve Hepatitis D total Ab +ve Hepatitis E IgM –ve, IgG –ve HDV superinfection Superinfection can lead to fulminant hepatitis Mortality rate for HDV infection is 2-20%")
8
Case Study – Mr SG Symptoms and liver function tests improved but ongoing fatigue June 2010 - Liver function tests remained elevated probably due to chronic Hepatitis D (HBV DNA negative)
")
9
Case Study – Mr SG Test result21.08.200824.09.200830.09.200816.06.2010 Bilirubin (<18) μmol/L66233410 ALP (30-130) U/L71123135109 GGT (<60) U/L29742596185 ALT (5-55) U/L2512453781372 AST (5-55) U/L244703158218 Albumin (38-48) g/L4639 46 INR (0.9-1.2)-1.01.61.0 Platelet count (150-400)178170116121
 μmol/L ALP (30-130) U/L GGT (<60) U/L ALT (5-55) U/L AST (5-55) U/L Albumin (38-48) g/L INR ( ) Platelet count ( )")
10
Case Study – Mr SG Consideration for liver biopsy and treatment with interferon therapy Treatment deferred

11
Min Li

12
Introduction Hepatitis is serious inflammation of the liver caused by hepatitis viruses Most common – Hepatitis A, B, C Less common – Hepatitis D, E Liver – Inflammation - cirrhosis - cancer

13
Hepatitis Delta Hepatitis D or Hepatitis Delta: Discovered by Dr Rizzetto in 1977 Is a defective single stranded RNA virus It requires Hepatitis B virus for its own replication It is the least common but most severe form of viral hepatitis

14
What is HepD virus? 36-43 nanometres in diameter The genome of the virus is very small and consists of single- stranded RNA and HD Ag HDV does not synthesize its own coat, it is enveloped by Hepatitis B surface antigen Its replication requires helper functions provided by HBsAg

15
HDV viral replication inserts its genetic material into liver cells uses liver cell resources to replicate itself genetic material is assembled in the host liver cell outer coating synthesizes its own outer protein coat release from host cell as Hep D virus HBsAg

16
Geographic distribution of HDV Infection Generally corresponds to prevalence of chronic HBV infection world wide. However, distinct features have been documented For those countries in which the prevalence of chronic HBV is low, distribution of HDV is low among chronic HBV carriers In these countries (like Australia) HDV infection commonly occurs among intravenous drug users
 HDV infection commonly occurs among intravenous drug users.")
17
Route of transmission Similar to those for HBV (except vertical transmission is rare) Percutaneous Contaminated drug use equipment Transfusion of infected blood and blood products Permucosal Sexually transmitted, although less efficient than HBV
 Percutaneous Contaminated drug use equipment Transfusion of infected blood and blood products Permucosal Sexually transmitted, although less efficient than HBV")
18
Who is at Risk of HDV infection? Chronic HepB carrier Anyone at risk for HBV Injecting drug users Haemophiliacs/haemodialysis patients Homosexuals and heterosexuals with multiple sex partners It has been estimated that 15 million people with Hepatitis B are infected with Hepatitis D In Australia, over the last 6 years, 20-30 cases reported each year

19
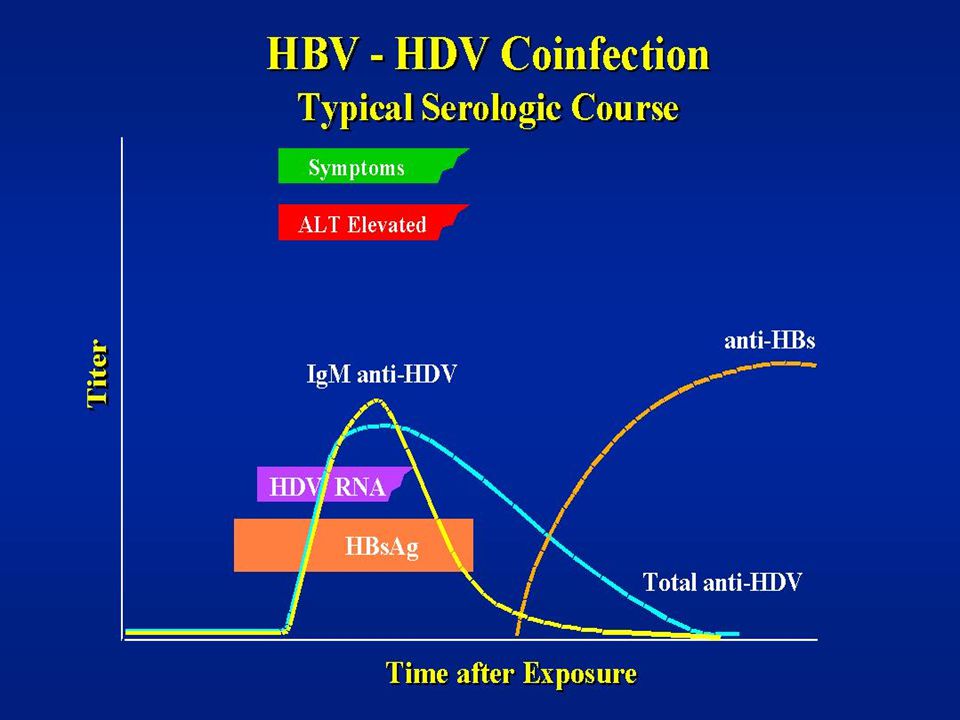
HDV infection clinical features Coinfection Superinfection Coinfection Superinfection HDV HBV HDV HDV HBV HDV Healthy individual HBV Carrier Healthy individual HBV Carrier 3-4% 90% Rare 7-10% 10-15% 80% 3-4% 90% Rare 7-10% 10-15% 80% Fulminant Recovery Chronic Fulminant Acute, severe Chronic Fulminant Recovery Chronic Fulminant Acute, severe Chronic Hepatitis with immunity HBV/HDV Hepatitis disease HBV/HDV Hepatitis with immunity HBV/HDV Hepatitis disease HBV/HDV Death Cirrhosis Death Recovery Death Death Cirrhosis Death Recovery Death

20
Symptoms of HDV infection Similar to Hepatitis B loss of appetite nausea and vomiting tiredness pain in the liver (upper, right side of abdomen) muscle and joint pain jaundice (yellowish eyes and skin, dark urine and pale-coloured faeces)
 muscle and joint pain jaundice (yellowish eyes and skin, dark urine and pale-coloured faeces)")
23
Diagnosis of Hepatitis D Detection of HDV RNA by PCR : sensitive method can detect 10-100 copies of HDV genome in infected serum HD Ag detection by EIA The finding of HD Ag in the serum indicating acute HDV infection and early stage of infection Anti –HD IgM, IgG detection by EIA The serological response to HDV infection. Provides supplemental evidence for HDV infection.

24
RPAH Serology Section Testing algorithm Normally would not test for HDV unless HBV surface antigen present Sometimes patient history is not provided when a request for HDV is received Testing requests for HDV are almost exclusively by specialists HDV RNA requests uncommon, though requests received are from experienced specialists Crucial window between RNA presence and HDV-Ab presence These requests are forwarded to VIDRL

25
RPAH Serology Section Qualitative HDV detection conducted by detecting total antibodies to HDV antigen (anti-HD) Dia Sorin ETI-AB-DELTAK-2 (P2808) 1. Well coated with recombinant HD Ag. 2. Anti-HD from sample or control. 3. Enzyme tracer: anti-HD antibodies (human) conjugated to horseradish peroxidase (H R P).
 conjugated to horseradish peroxidase (H R P)..")
26
RPAH Serology Section Dia Sorin EIA Performed fortnightly Manual test Samples tested in duplicate One blank, positive and negative controls / run External controls periodically tested and monitored Results are calculated manually Interpreted via cut-off values derived from positive and negative controls All initial positives are repeated before reporting

27
Anti-HDV total anti-bodies (RPA)
")
28
Treating Hepatitis D There is no antiviral therapy specifically for chronic hepatitis D Individuals with chronic HDV and HBV infection should follow HBV therapy Research indicates using Pegylated interferon demonstrates some benefit in people with hepatitis D Liver transplantation may be considered for end-stage chronic hepatitis D

29
Prevention of Hepatitis D No vaccine specific for HDV Since HDV is dependent on HBV for replication, preventing HDV through HBV vaccination can be effective In HDV superinfection, education to reduce risk behaviours and reduce exposure to infectious blood

30
Australian Society for Microbiology NSW-ACT Branch Proudly sponsored in 2011 by: Platinum Sponsor Gold Sponsor Silver Sponsor Bronze Sponsors

Similar presentations





,FICM,FCCS CONSULTANT INTERNAL MEDICINE & CRITICAL CARE IVY HOSPITAL MOHALI Hepatitis D.>")

>")









 Hepatitis type B virus (Hepadnaviridae)>")

