Download presentation
Presentation is loading. Please wait.

1
Pancreatic diseases WU JIAN Department of hepatobiliary Surgery First Affiliated Hospital Zhejiang University School of Medicine

2
Pancreas: Anatomy and Physiology Retroperitoneal organ Retroperitoneal organ 15-20cm in length 15-20cm in length Head, neck, body and tail Head, neck, body and tail Uncinate process: curves behind the superior mesenteric vessels Uncinate process: curves behind the superior mesenteric vessels

3
Posterior Posterior L1-2 vertebral column L1-2 vertebral column Anterior Anterior stomach, omentum stomach, omentum Right Right Duodenum Duodenum Left Left Splenic hilum Splenic hilum Neighborhood of the pancreas

4
Main duct : Wirsung ( 1642) Main duct : Wirsung ( 1642) Ampula: Vater (1720) Ampula: Vater (1720) Accessory duct : Santorini( 1734) Accessory duct : Santorini( 1734)
 Main duct : Wirsung ( 1642) Ampula: Vater (1720) Ampula: Vater (1720) Accessory duct : Santorini( 1734) Accessory duct : Santorini( 1734)")
5
Pancreas: blood supply HEAD : HEAD : Superior pancreatoduodenal A. (from gastroduodenal A.) Superior pancreatoduodenal A. (from gastroduodenal A.) Inferior pancreatoduodenal A. (from SMA) Inferior pancreatoduodenal A. (from SMA) BODY AND TAIL : BODY AND TAIL : superior pancreatic A. superior pancreatic A. pancreatic magna A. pancreatic magna A. transverse pancreatic A. transverse pancreatic A. VEIN : VEIN : to splenic vein,SMV and portal vein to splenic vein,SMV and portal vein
 Superior pancreatoduodenal A. (from gastroduodenal A.) Inferior pancreatoduodenal A. (from SMA) Inferior pancreatoduodenal A. (from SMA) BODY AND TAIL : BODY AND TAIL : superior pancreatic A. superior pancreatic A. pancreatic magna A. pancreatic magna A. transverse pancreatic A. transverse pancreatic A. VEIN : VEIN : to splenic vein,SMV and portal vein to splenic vein,SMV and portal vein.")
6
Lymphatic drainage of pancreas

7
Common Common pathway pathway

8
Physiology Exocrine : pancreatic juice 。 Exocrine : pancreatic juice 。 HCO 3 - and digestive enzyme HCO 3 - and digestive enzyme Endocrine : Endocrine : A cell : glycagon A cell : glycagon B cell : insulin B cell : insulin D cell : somatostatin D cell : somatostatin G cell : gastrin G cell : gastrin

9
Acute Pancreatitis Chronic Pancreatitis Chronic Pancreatitis Pancreatic cancer Periampullary cancer Periampullary cancer Endocrinal tumor Endocrinal tumor

10
Acute Pancreatitis Common acute abdomen Common acute abdomen Local inflammatory change in pancreas Local inflammatory change in pancreas Systemic change Systemic change Life-threatening inflammatory disorder of the pancreas Life-threatening inflammatory disorder of the pancreas Abrupt onset and unpredictable course Abrupt onset and unpredictable course Variable severity and duration Variable severity and duration Self-limited but remarkable morbidity and mortality Self-limited but remarkable morbidity and mortality

11
Etiology Biliary tract disease Biliary tract disease Abuse of ethanol Abuse of ethanol Endoscopic retrograde cholangiopancreatography Endoscopic retrograde cholangiopancreatography Trauma and operation Trauma and operation Ischemia of pancreas Ischemia of pancreas Drugs Drugs Idiopathic pancreatitis Idiopathic pancreatitis Hypercalcemia Hypercalcemia Hyperlipidemia Hyperlipidemia Infections and Parasites Infections and Parasites Scorpion sting Scorpion sting

12
PATHOGENESIS “ Self digestion ” “ Self digestion ” Reflux of bile or duodenal juice Reflux of bile or duodenal juice Trypsinogen was activated Trypsinogen was activated Trypsin can activate the other zymogens Trypsin can activate the other zymogens Intraparenchymal enzyme activation, tissue destruction, and ischaemic necrosis. Intraparenchymal enzyme activation, tissue destruction, and ischaemic necrosis.

13
Pathological and clinical type Pathological type Pathological type Acute edematic pancreatitis Acute edematic pancreatitis Acute hemorrhgic and necrotic pancreatitis (AHNP) Acute hemorrhgic and necrotic pancreatitis (AHNP) Clinical type Clinical type Mild Acute pancreatitis (MAP) Mild Acute pancreatitis (MAP) Severe Acute pancreatitis (SAP) Severe Acute pancreatitis (SAP) Fulminant Acute pancreatitis (FAP) Fulminant Acute pancreatitis (FAP)
 Acute hemorrhgic and necrotic pancreatitis (AHNP) Clinical type Clinical type Mild Acute pancreatitis (MAP) Mild Acute pancreatitis (MAP) Severe Acute pancreatitis (SAP) Severe Acute pancreatitis (SAP) Fulminant Acute pancreatitis (FAP) Fulminant Acute pancreatitis (FAP)")
14
Clinical manifestations Abdominal pain Abdominal pain Nausea, vomiting Nausea, vomiting Distension Tenderness, rebound tenderness, muscular regard Tenderness, rebound tenderness, muscular regard Fever , jaundice , Fever , jaundice , Gray-Turner sign: flank ecchymoses Gray-Turner sign: flank ecchymoses Cullen sign: periumbilical ecchymoses Cullen sign: periumbilical ecchymoses MODS MODS

15
laboratory test Amylase level in serum and in urine Amylase level in serum and in urine Lipase assays Lipase assays Blood Rt, liver function, FBS, PaCO2,serum calcium, DIC Blood Rt, liver function, FBS, PaCO2,serum calcium, DIC Diagnostic paracentesis Diagnostic paracentesis

16
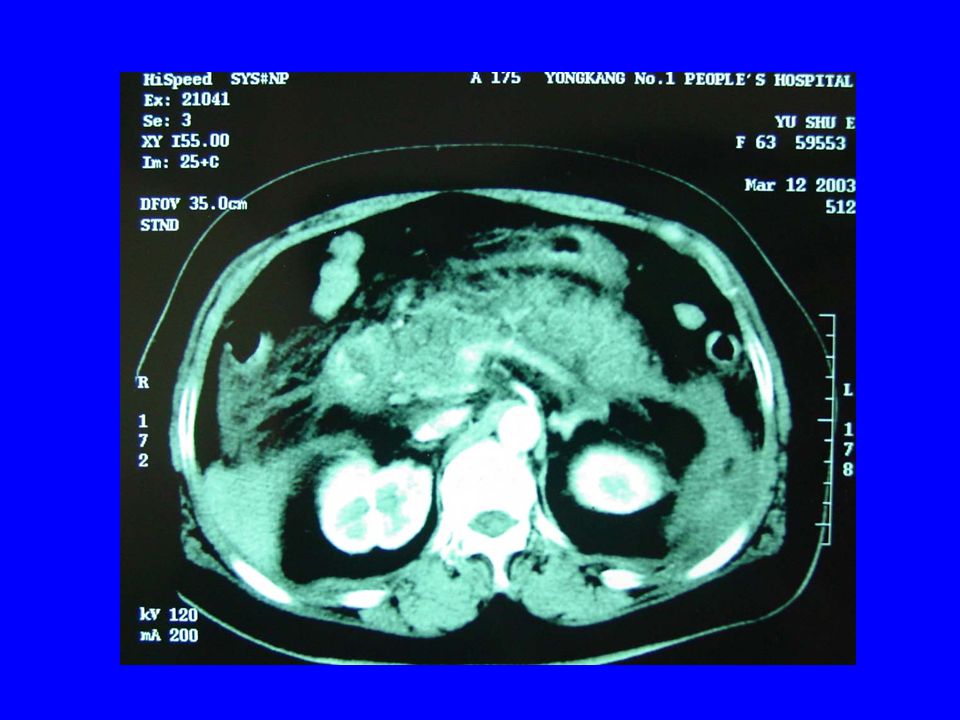
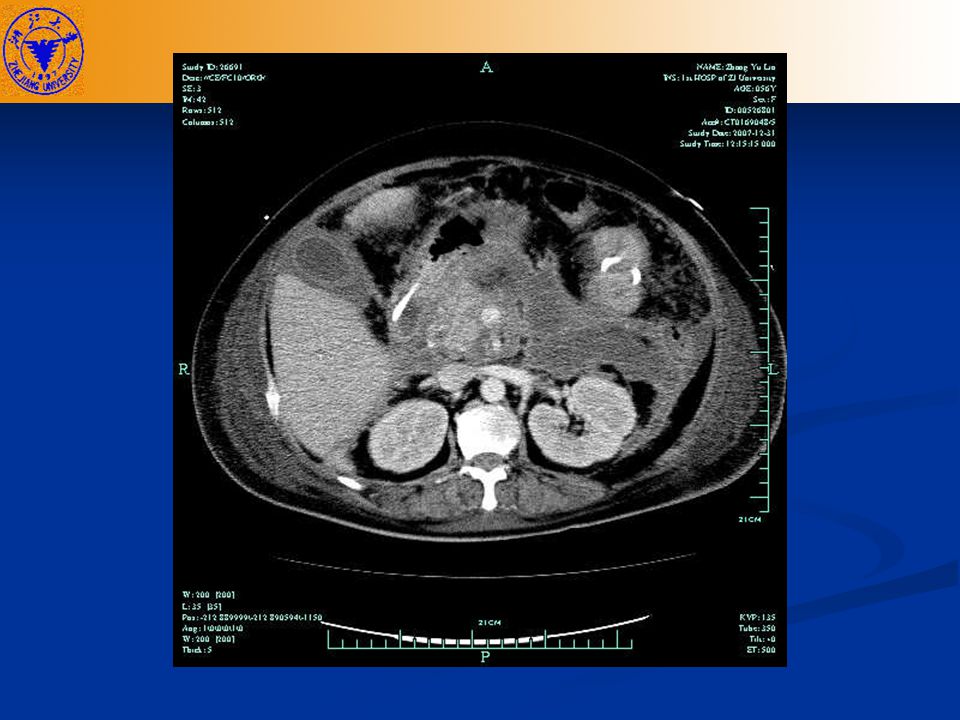
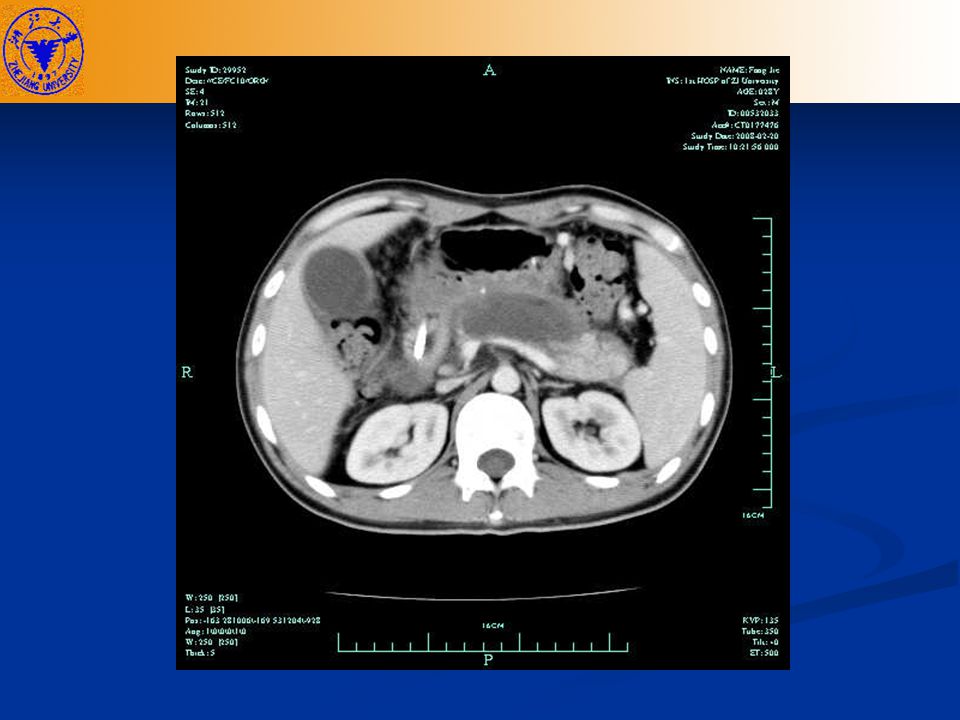
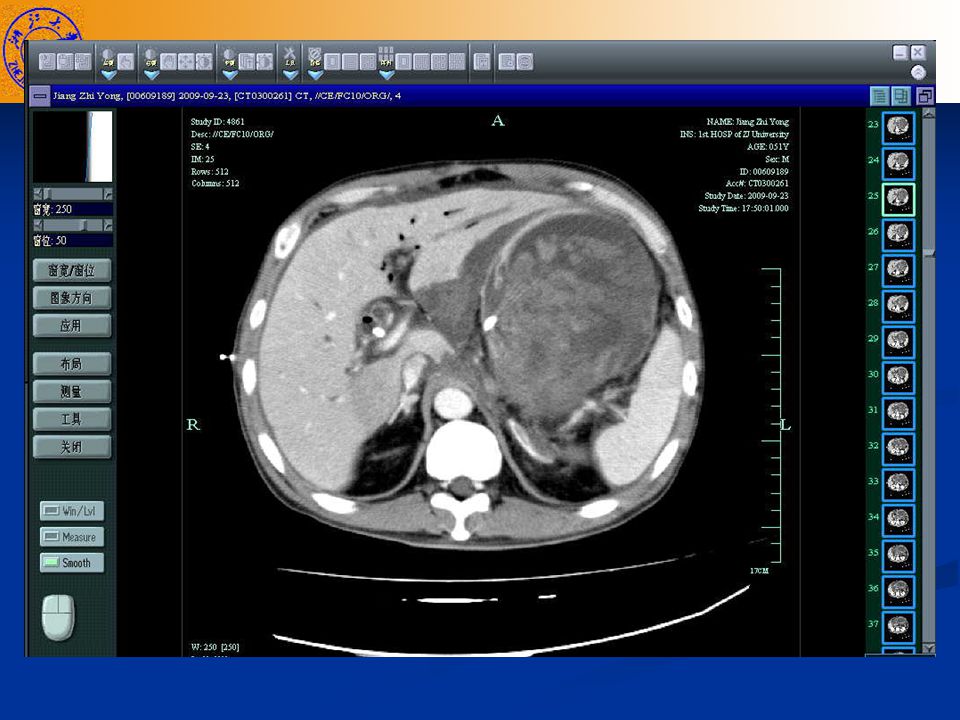
Image findings BUS BUS CT CT ERCP ERCP MRCP MRCP Abdomen plain film Abdomen plain film

24
Pancreatic necrosis Pancreatic necrosis Infective pancreatic necrosis Infective pancreatic necrosis Sterile pancreatic necrosis Sterile pancreatic necrosis Pancreatic abscess Pancreatic abscess Pancreatic pseudocyst Pancreatic pseudocyst Local complication

25
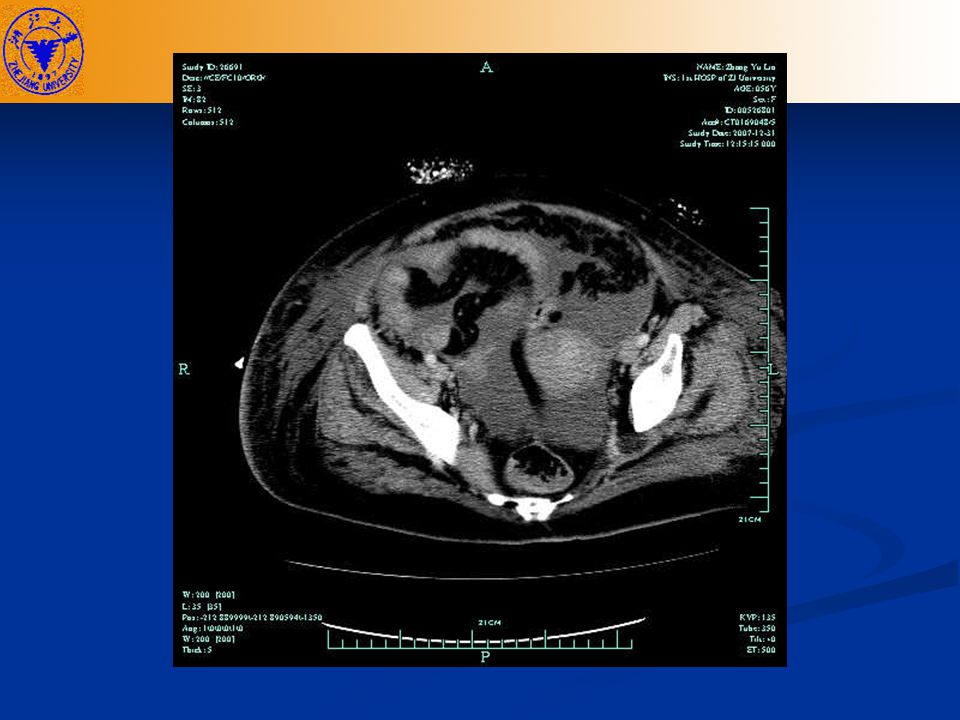
Acute pancreatic pseudocyst Peripancreatic fluid collections occur in 10-20 % of patients Peripancreatic fluid collections occur in 10-20 % of patients Those persisting beyond the phase of acute inflammation become pancreatic pseudocysts Those persisting beyond the phase of acute inflammation become pancreatic pseudocysts Collection surrounded by fibrous tissue or granula tissue Collection surrounded by fibrous tissue or granula tissue Diagnosed by PE or image test Diagnosed by PE or image test Round or ellipse Round or ellipse Clear cyst wall Clear cyst wall

29
Severe Acute Pancreatitis Severe Acute Pancreatitis Severe Acute pancreatitis (SAP) Severe Acute pancreatitis (SAP) Complicated with MODS Complicated with MODS Necrosis, abscess, pseudocyst Necrosis, abscess, pseudocyst Or both Or both
 Severe Acute pancreatitis (SAP) Complicated with MODS Complicated with MODS Necrosis, abscess, pseudocyst Necrosis, abscess, pseudocyst Or both Or both")
30
Classification system General evaluation General evaluation John Ranson score (1974):5 (on admission) +6 (48hr) John Ranson score (1974):5 (on admission) +6 (48hr) Imrie score:8 (WBC,Ca,sugar,PO2,LF) Imrie score:8 (WBC,Ca,sugar,PO2,LF) APACHE II score (1985):12+age + Chronic health+coma APACHE II score (1985):12+age + Chronic health+coma Atlanta classification system(1992) Atlanta classification system(1992) Local evaluation Local evaluation Beger ’ criteria (1985) Beger ’ criteria (1985) Balthazar CT classification system (1990):I, II, III GRADE Balthazar CT classification system (1990):I, II, III GRADE MODS evaluation MODS evaluation Marshall MODS score system(1995):6 systems/organs involved Marshall MODS score system(1995):6 systems/organs involved
:5 (on admission) +6 (48hr) John Ranson score (1974):5 (on admission) +6 (48hr) Imrie score:8 (WBC,Ca,sugar,PO2,LF) Imrie score:8 (WBC,Ca,sugar,PO2,LF) APACHE II score (1985):12+age + Chronic health+coma APACHE II score (1985):12+age + Chronic health+coma Atlanta classification system(1992) Atlanta classification system(1992) Local evaluation Local evaluation Beger ’ criteria (1985) Beger ’ criteria (1985) Balthazar CT classification system (1990):I, II, III GRADE Balthazar CT classification system (1990):I, II, III GRADE MODS evaluation MODS evaluation Marshall MODS score system(1995):6 systems/organs involved Marshall MODS score system(1995):6 systems/organs involved")
31
Clinical manifestation of SAP Abdominal sign: obvious tenderness, rebound tenderness, muscular regard, distension, lose of bowl sound Abdominal sign: obvious tenderness, rebound tenderness, muscular regard, distension, lose of bowl sound Mass in abdomen, Grey - Turner, Cullen Mass in abdomen, Grey - Turner, Cullen MODS MODS Irreversible shock Irreversible shock CT: swelling , uneven density, invade to outside of pancreas(Balthazar CT>II) CT: swelling , uneven density, invade to outside of pancreas(Balthazar CT>II) APACHE value>8 APACHE value>8
 CT: swelling , uneven density, invade to outside of pancreas(Balthazar CT>II) APACHE value>8 APACHE value>8")
32
MODS Cardiac function : quick pulse 、 shock Cardiac function : quick pulse 、 shock Pulmonary function : PaO2<60mmHg , ARDS Pulmonary function : PaO2<60mmHg , ARDS Liver function : jaundice , elevated ALT Liver function : jaundice , elevated ALT Renal function : elevated BUN and Creatinine Renal function : elevated BUN and Creatinine Digestive function : GI bleeding Digestive function : GI bleeding Endocrinal function : glucose>11.1mmol/L Endocrinal function : glucose>11.1mmol/L Coagulation system : DIC Coagulation system : DIC Nerve system : unclear consciousness 、 pancreatic brain disease Nerve system : unclear consciousness 、 pancreatic brain disease

33
Stage of SAP Acute response stage : within 2 weeks complicated with shock,ARDS,renal failure Systemic infection stage : 2 weeks to 2 months Bacteria or fungus infection Post-infection stage : after 2 3 months Abscess, fistula,

34
TREATMENT

35
I.Non-operative therapy

36
Acute Response Stage ICU : to prevent MODS ICU : to prevent MODS fasting the patient, nasogastric suction fasting the patient, nasogastric suction Minimizing pancreatic secretion Minimizing pancreatic secretion antacids antacids 5-FU 5-FU somatostatin analogues somatostatin analogues antiprotease antiprotease Fluid replacement and Nutritional support Fluid replacement and Nutritional support maintenance of adequate hydration maintenance of adequate hydration TPN , glucose,lipid, amino acid, protein TPN , glucose,lipid, amino acid, protein Analgesia Analgesia Antibiotics Antibiotics Traditional Chinese Medicine Traditional Chinese Medicine Abdominal lavage Abdominal lavage

37
II. Operation

38
Indication of Operation Biliary obstruction Biliary obstruction Secondary pancreatic infection Secondary pancreatic infection Shock cannot be reversed, Shock cannot be reversed, multiple ogan deteriorate multiple ogan deteriorate Undetermined diagnosis, need to laparotomy Undetermined diagnosis, need to laparotomy

39
Principle for treatment of pancreatitis MAP SAP Biliary Non-biliary ObstuctiveNon-obstructiveInfection Noinfection Conservativetherapy Urgent operation Or ERCP Conservativetherapy Elective operation Conservativetherapy

40
Chronic pancreatitis Recurrent upper abdominal pain Recurrent upper abdominal pain With dysfunction of endocrine and exocrine of pancreas With dysfunction of endocrine and exocrine of pancreas

41
Clinical manifestition Four main symptoms Four main symptoms Abdominal pain Abdominal pain Body weight loss Body weight loss Diabetes Diabetes Lipid diarrhea Lipid diarrhea

43
Therapy of chronic pancreatitis Relieve pain Drainage of the pancreatic juice Prevent acute attack Ameliorate the nutrition Improve pancreatic function Non-operation or operation

45
Pancreatic Cyst Pancreatic pseudocyst Pancreatic pseudocyst Congenital pancreatic cyst Congenital pancreatic cyst Retention pancreatic cyst Retention pancreatic cyst Neoplastic pancreatic cyst Neoplastic pancreatic cyst Pancreatic cystadenoma Pancreatic cystadenoma Pancreatic cystadenocarcinoma Pancreatic cystadenocarcinoma

46
Pancreatic pseudocyst Indication for operation Indication for operation Associated with ongoing pain Associated with ongoing pain More than 6 cm in diameter which persist for 6 weeks More than 6 cm in diameter which persist for 6 weeks Cyst with haemorrhage and sepsis Cyst with haemorrhage and sepsis Methods Methods Percutaneous drainage Percutaneous drainage Operative drainage Operative drainage Cystgastrostomy, cystjejunostomy Cystgastrostomy, cystjejunostomy Resection of pancreatic body and tail Resection of pancreatic body and tail

48
Thanks !

Similar presentations












 EXOCRINE PANCREASE Lecture Dr. Gamal Hamra Wednesday 01/12/1430 (18/11/2009)>")














