Download presentation
Presentation is loading. Please wait.

1
Epilepsy and convulsion syndromes

2
Epilepsy is a chronic disorder, which is characterized by the presence of: Epileptic focus Recurrent attacks with various clinical signs Personality disorders between attacks Some specific paraclinical signs

5
Epilepsy as a disease should be differentiated from: Epileptic reaction Epileptic syndrome

6
Epileptic reaction – is the response of the brain to the strong external and internal damaging factors (such as electro – shock, insulin shock, brain hypoxia, severe alcohol intoxication and so on). The main clinical features of epileptic reaction are abortive seizures or general tonic – clonic seizures.

7
Epileptic syndrome – is characterized by recurrent epileptic attacks on the background of pathologic focus in brain. The attacks are variable and depend on the localization of focus. Focal symptoms are obligatory in this case.

8
Risk factors Inheritance Organic brain diseases Prenatal (infections – cytomegalovirus, rubella, toxoplasmosis, toxicosis of pregnancy, diet disturbances) Perinatal (physical trauma, child birth anoxia, metabolic disorders, neonatal infection) Postnatal (infections, trauma, dehydration, toxins) Disorders of brain function. Sleep disorders. Paroxysmal states in childhood Newborns seizures Febrile seizures Affective – respiratory seizures

9
Pathology The results of organic diseases The results of epileptic process Each epileptic attack causes hypoxic changes in brain and leads to the development of encephalopathy

10
Pathologic physiology There is a group of neurons with pathologic activity, which is called epileptic focus There is the ability to enforce and spread the activity Weakness of anti - epileptic protection. (It is provided by caudal parts of the brain)
.")
11
Pathophysiology Presence of neurons’ group with pathological activity (epifocus) Ability to spread activity Weakness of system of antiepileptic defense
 Ability to spread activity Weakness of system of antiepileptic defense")
12
Neurochemistry of epilepsy Disorders of balance between glutamate (exciting neurotransmitter), GABA (inhibitory neurotransmitter) that leads to desynchronization. Disorders of K / Na pump

13
Immunology of epilepsy There is increasing content of anti– brain antibodies. The primary attack causes disturbances of HEB. The result is production of antibodies and CIC that are fixed in brain tissue and encourage its lesion in new zones.

14
Classification of epileptic attacks Partial epileptic Simple Simple motor Focal motor without march Focal motor with march Adversive Postural Phonatory simple Simple sensory Somatosensory (with and without march) Visual, acoustical, gustatory, smell) Simple autonomic – visceral Simple with psychiatric disorders Aphatic Dysmnestic With thinking disturbances (ideatory) Emotional – affective Hallucinatory
 Visual, acoustical, gustatory, smell) Simple autonomic – visceral Simple with psychiatric disorders Aphatic Dysmnestic With thinking disturbances (ideatory) Emotional – affective Hallucinatory")
15
Classification of epileptic attacks Complex Temporal pseudoabsance Automatisms Simple with generalization (secondary general) General attacks Absance Typical Atypical Myoclonic Tonic – clonic Tonic Clonic General atonic Non classified Epileptic status
 General attacks Absance Typical Atypical Myoclonic Tonic – clonic Tonic Clonic General atonic Non classified Epileptic status")
19
Clinical features A. General seizures. Epileptic general tonic – clonic attack (grandmal) usually begins with short initial stage that lasts several seconds. The last can manifest as: Bilateral general muscle jerks Loss of consciousness Autonomic changes Enlargement of pupils
 usually begins with short initial stage that lasts several seconds. The last can manifest as: Bilateral general muscle jerks Loss of consciousness Autonomic changes Enlargement of pupils.")
20
Types of epileptic tonic attacks Axial – body and facial muscles are involved in attack. There is spasm of respiratory muscles and breathing stop at expiration. The same signs plus less involvement of extremities muscles. Global means involvement of body and extremities muscles in the same way.

21
Clonic epileptic attacks general typical clonic attacks are often observed in newborn babies. loss of consciousness autonomic disorders rhythmic clonic seizures between the attacks of clonic muscles jerking movements there is muscle hypotonia If the attacks last 1–2 min the consciousness recovers quickly. But these attacks can last 4–5 min and even more. Then after the attack coma can develop.

22
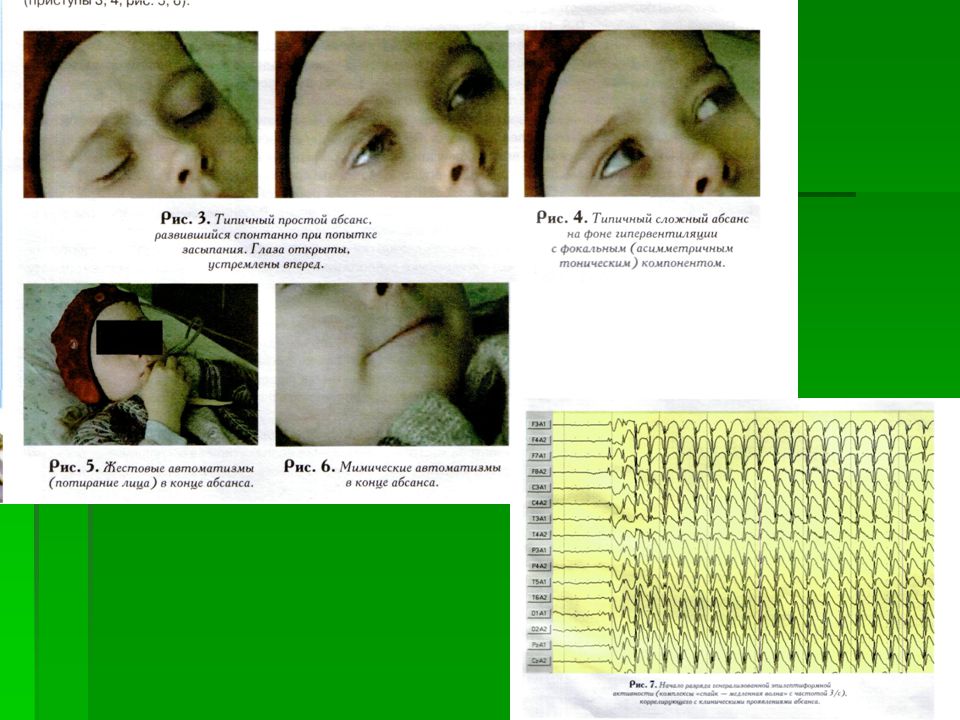
Without seizure attacks Complex absance can be divided into myoclonic, atonic, tonic and with automatisms. Myoclonic absance - loss of consciousness, rhythmic bilateral myoclonus in muscles of face and upper extremities. There are jerking movements in eyelids, periorbital muscles, mouth edges, eye bulbs. The patient can loose some objects which he is holding in his arms Atonic absance - decreasing of postural tonus, hanging head and sudden drops Tonic absance is associated with looking of eyes upwards. There is domination of either extensor or flexor component, symmetric or asymmetric

23
Without seizure attacks Absance with automatism can be the sign of focal attack and absance. The main condition for automatism is incomplete loss of consciousness. Typical absance are associated with bilateral symmetric complexes “top – waves” with frequency 3 per sec in frontal–central lobe. Atypical absance

24
Focal attacks Groups of focal attacks: Simple focal Complex focal Focal attacks with secondary generalization. Differential feature of complex focal attacks from simple - loss of consciousness.

25
Symptoms: Motor Sensory (somatosensory, visual, acoustical, olphactory, taste attacks and epileptic attacks of dizziness) Autonomic Psychiatric that depends on focus localization Epileptic discharges in motor speech center speech disorders or involuntary vocalization – involuntary repetition of words are observed. As for visual, acoustical, olphactory, taste attacks and epileptic attacks of dizziness they can manifest as simple disorders or complex illusion or hallucinations.

26
Intensive Video-EEG-Monitoring

27
Treatment The main principals : emergency accordance to stages following On the way to hospital: To release breathing air ways Digitalis drugs Sibazonum 0.01g

28
Treatment In ambulance: Tracheobronchial tree drain Sibazonum 30 ml in 150 ml of physiological solution, in 10 min we add the medication up to 100 – 120 mg Magnesiii sulfas 25% 10.0 in glucose 40 % Anesthesia with nitrous oxide Dosed anesthesia Aminazinum 25% 1-2 ml Atropinum 0.1% 1.0 s/c Cardiac, antihistamine, diuretics Natrii tiopentali 1g in 10 ml of physiological solution

29
Treatment Epileptic status To provide permeability of respiratory airways To evaluate the function of heart – vascular and respiratory systems To provide free way to veins Lorazepam 4mg i/v or Diazepam 10 mg In the hospital To take blood for analysis % of urea, electrolytes liver function % of glucose % of blood gas etiology of attack – hypoglycemia – 50% solution of glucose 50 mg at alcohol abuse – Tiaminum

30
Treatment Next half an hour: to introduce the medication through the naso–gastral tube Fentoin 18 mg per kg or Phenobarbitalum 15 mg per kg i/v by drop 100 mg per kg In 30 minutes: General anesthesia EEG

31
Surgical methods of treatment: Resections Anterior temporal lobectomy Selective amygdalohypocampoectomia Calosotomia Hemisphereectomia Stereotaxic Destruction of deep temporal structures. This procedure on lateral part normally decreases seizures, on medial ones – aggression.

32
Radio – surgical with γ – knife. γ – waves from 201 sources are focused on certain distance. The effectiveness of this procedure is 70 – 80 %. Electrostimulative – stimulation of certain structures: Nucleus dentatus, the caput of nucleus caudatus Stimulation of n. vagus – this method is one of the newest one. It is indicated at partial seizures with secondary generalization.

34
Treatment of patients with epileptic status

35
Measures Time, min Treatment 0-5 Definition of state of living functions. Oxigenotherapy. 6-10 Intravenous infusion of physiological solution. Checking of tempeature, BP, biochemical blood analysis. Intravenous injection of Tiaminum 100 mg, then 50 ml 40 % glucose.

36
Time, min Treatment 11-15 Intravenous injection of Diazepam 0,2 mg per kg (speed 5 mg per min). Injection is repeated every 5 min. General dose is not more then 20 mg 16-45 Intravenous injection by drops of Fenitoin in dose 20 mg per kg (speed 50 mg per min). While injection ECG is made, BP is checked. At changes on ECG or BP injection is stopped. If attacks continue we can add 5 – 10 mg per kg of Fenitoin.
. While injection ECG is made, BP is checked. At changes on ECG or BP injection is stopped. If attacks continue we can add 5 – 10 mg per kg of Fenitoin..")
37
Time, min Treatment 46-59 If attacks continue we make endotracheal intubation, then use Fenobarbitalum in dose 20 mg per kg (speed 100 mg per min) 60-90 If attacks continue we introduce patient in barbiturate coma. It is recommended to start usage of Fenobarbital in dose 5 mg per kg up to stopping of epileptic activity on EEG.Then continue usage of 0,5-3,0 mg per kg per hour to stop recurring attacks. From time to time we decrease speed to prove ourselves that the attacks are absent. While infusion we check EEG, ECG, BP and breathing functions.

Similar presentations

 The only diagnostic test for absence seizures Ambulatory EEG monitoring over 24 hours may be useful to.>")



. An extremely.>")













