Download presentation
Presentation is loading. Please wait.

1
Mr. J is a 70 year old man with an ischemic cardiomyopathy who presents with class III CHF and significant dissatisfaction with his functional capacity (can only walk 100-200 yards on the level). Past history is significant for an anterior MI, intermittent atrial fibrillation, and a dual chamber ICD implant in 2002 for syncope, a positive TWA stress test, and inducible VT at EPS. His medicines include digoxin 0.125 mg QD, amiodarone 200 mg QD, Lasix 40 mg QD, Coreg 12.5 mg BID, and lisinopril 5 mg QD. Aldactone was stopped due to hyperkalemia and azotemia. A BP of 88/56 has prevented more aggressive drug Rx.
. Past history is significant for an anterior MI, intermittent atrial fibrillation, and a dual chamber ICD implant in 2002 for syncope, a positive TWA stress test, and inducible VT at EPS. His medicines include digoxin mg QD, amiodarone 200 mg QD, Lasix 40 mg QD, Coreg 12.5 mg BID, and lisinopril 5 mg QD. Aldactone was stopped due to hyperkalemia and azotemia. A BP of 88/56 has prevented more aggressive drug Rx..")
2
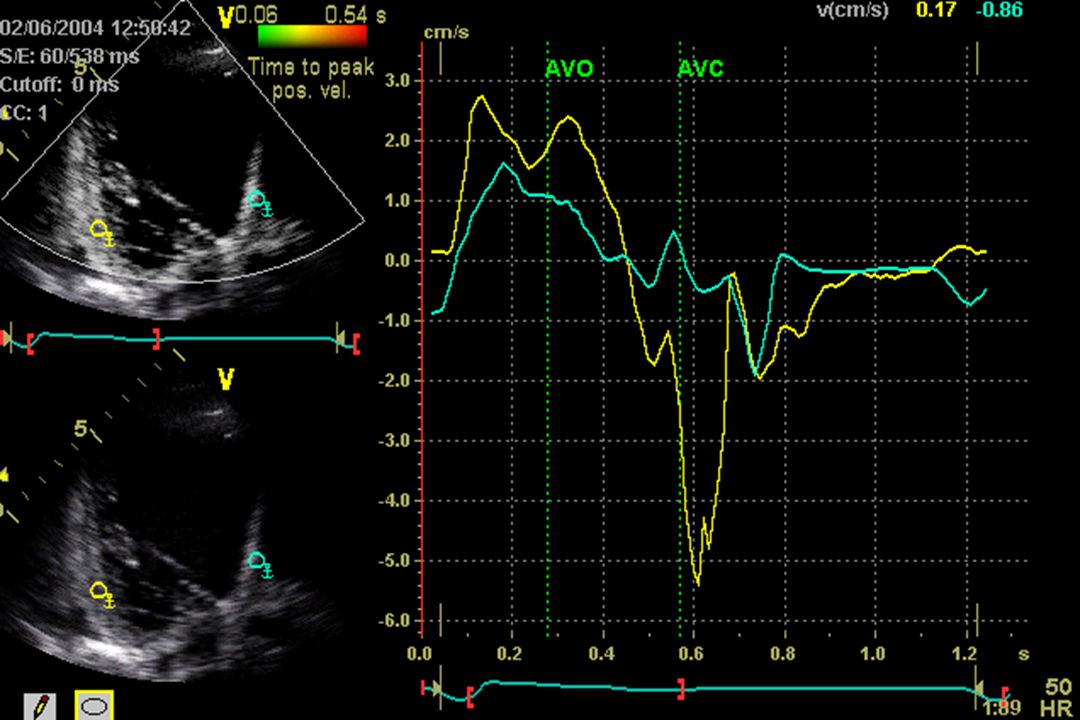
Work-up revealed a QRS duration of 120-130 ms (paced). His EF was 25% on echo, with a severely dilated LV, 4+ MR, and a PA pressure of 54 mm. Additional echo Doppler assessment for CRT demonstrated a prolonged aortic pre- ejection interval (350ms, >160 ms suggests response to CRT) and tissue Doppler findings of a prolonged interval (100 ms) between earliest and latest peak systolic velocity (comparing 6 basal wall segments). Work-up revealed a QRS duration of 120-130 ms (paced). His EF was 25% on echo, with a severely dilated LV, 4+ MR, and a PA pressure of 54 mm. Additional echo Doppler assessment for CRT demonstrated a prolonged aortic pre- ejection interval (350ms, >160 ms suggests response to CRT) and tissue Doppler findings of a prolonged interval (100 ms) between earliest and latest peak systolic velocity (comparing 6 basal wall segments).
 and tissue Doppler findings of a prolonged interval (100 ms) between earliest and latest peak systolic velocity (comparing 6 basal wall segments). Work-up revealed a QRS duration of ms (paced). His EF was 25% on echo, with a severely dilated LV, 4+ MR, and a PA pressure of 54 mm. Additional echo Doppler assessment for CRT demonstrated a prolonged aortic pre- ejection interval (350ms, >160 ms suggests response to CRT) and tissue Doppler findings of a prolonged interval (100 ms) between earliest and latest peak systolic velocity (comparing 6 basal wall segments)..")
3
The patient underwent upgrade of his ICD to a CRT-D device in 3/04, as part of a clinical trial investigating the utility of sequential biventricular pacing in CRT (InSync III Trial, Medtronic). The patient underwent upgrade of his ICD to a CRT-D device in 3/04, as part of a clinical trial investigating the utility of sequential biventricular pacing in CRT (InSync III Trial, Medtronic).
..")
4
Six months post implant, the patient is NHHA Class I (asymptomatic). He exercises 3 days weekly for approximately 2 hours at a time. His Six Minute Hall Walk Test in 9/04 measured 2000 feet, almost a 300% increase from his baseline of 675 feet pre-CRT. His BP was 114/67 prior to his walk and 132/70 after ambulation, with an increase in HR from 60 to 66 with ambulation and an O2 sat of 99% during ambulation. Six months post implant, the patient is NHHA Class I (asymptomatic). He exercises 3 days weekly for approximately 2 hours at a time. His Six Minute Hall Walk Test in 9/04 measured 2000 feet, almost a 300% increase from his baseline of 675 feet pre-CRT. His BP was 114/67 prior to his walk and 132/70 after ambulation, with an increase in HR from 60 to 66 with ambulation and an O2 sat of 99% during ambulation.
. He exercises 3 days weekly for approximately 2 hours at a time. His Six Minute Hall Walk Test in 9/04 measured 2000 feet, almost a 300% increase from his baseline of 675 feet pre-CRT. His BP was 114/67 prior to his walk and 132/70 after ambulation, with an increase in HR from 60 to 66 with ambulation and an O2 sat of 99% during ambulation..")
10
Cardiac Resynchronization Therapy (CRT) In patients with significant symptoms of CHF, intraventricular conduction delay on ECG (QRS>120 ms), and EF 120 ms), and EF <35%, CRT is safe and well toleratedis safe and well tolerated improves quality of life, functional class, exercise capacityimproves quality of life, functional class, exercise capacity improves cardiac structure and function improves cardiac structure and function
 In patients with significant symptoms of CHF, intraventricular conduction delay on ECG (QRS>120 ms), and EF 120 ms), and EF <35%, CRT is safe and well toleratedis safe and well tolerated improves quality of life, functional class, exercise capacityimproves quality of life, functional class, exercise capacity improves cardiac structure and function improves cardiac structure and function")
11
Bradley JAMA 2003

12
COMPANION Trial ( ) : Hypothesis COMPANION Trial (Comparison of Medical Therapy, Pacing and Defibrillation in Heart Failure) : Hypothesis “Prophylactic cardiac resynchonization therapy in the form of biventricular stimulation with a pacemaker, with or without a defibrillator, will reduce the risk of death and hospitalization in patients with advanced chronic heart failure and intraventricular conduction delays.”
 : Hypothesis COMPANION Trial (Comparison of Medical Therapy, Pacing and Defibrillation in Heart Failure) : Hypothesis Prophylactic cardiac resynchonization therapy in the form of biventricular stimulation with a pacemaker, with or without a defibrillator, will reduce the risk of death and hospitalization in patients with advanced chronic heart failure and intraventricular conduction delays.")
13
Key Inclusion Criteria NYHA Class III or IV NSR, >=QRS 120 ms, PR interval >150ms LVEF =60 mm Optimal pharmacological therapy Beta blocker (for at least 3 months) Diuretic, ACEI/ARB, spironolactone (1 month); +/- digoxin Hx of CHF hospitalization (or equivalent) 1 month prior to enrollment No bradycardiac or tachyarrhythmic device indication at the time of enrollment
 Diuretic, ACEI/ARB, spironolactone (1 month); +/- digoxin Hx of CHF hospitalization (or equivalent) 1 month prior to enrollment No bradycardiac or tachyarrhythmic device indication at the time of enrollment")
14
Study Design OPT 1 CRT + 2 OPT CRT-D + 2 Randomization Parallel Randomized design

15
Results (n=1520 patients) Secondary endpoint – Death from any cause
 Secondary endpoint – Death from any cause")
16
The Data Based on these results:Based on these results: 14 CRT-D devices would have to be placed to save one life at 12 mos.14 CRT-D devices would have to be placed to save one life at 12 mos. The majority of events, and the driving force behind the endpoints was hospitalizations.The majority of events, and the driving force behind the endpoints was hospitalizations. This study was not adequately powered to determine a difference between CRT and CRT-D.This study was not adequately powered to determine a difference between CRT and CRT-D.

17
Relative Cost of CRT

18
Not all patients benefit from CRT Electrical dyssynchrony on ECG does not necessarily indicate mechanical dyssynchrony.Electrical dyssynchrony on ECG does not necessarily indicate mechanical dyssynchrony. Tissue doppler may have a role in optimizing the selection of patients for CRT.Tissue doppler may have a role in optimizing the selection of patients for CRT.

Similar presentations


















 failure is the state in which the heart is unable to pump blood.>")


 Implantation indications and outcomes Guy Amit, MD; Mahmoud Suleiman, MD; Mark Kazatsker,>")


