Download presentation
Presentation is loading. Please wait.

1
Current status of adjuvant HER2 targeting therapy Valentina Guarneri, MD, PhD Istituto Oncologico Veneto IRCCS University of Padova

2
Trastuzumab plus chemotherapy: the gold standard for HER2 positive early breast cancer Improving on cardiac toxicity: different regimens and different treatment durations Improving on treatment efficacy: dual blockade and new anti-HER2 agents Toward personalized cancer medicine: challenging the gold standard for specific patient subgroups Outline

3
Trastuzumab plus chemotherapy: the gold standard for HER2 positive early breast cancer Improving on cardiac toxicity: different regimens and different treatment durations Improving on treatment efficacy: dual blockade and new anti-HER2 agents Toward personalized cancer medicine: challenging the gold standard for specific patient subgroups Outline

5
Meta-analysis of adjuvant trastuzumab trials: Disease-free Survival Moja L, et al. The Cochrane Library 2012, Issue 4

6
Meta-analysis of adjuvant trastuzumab trials: Overall Survival Moja L, et al. The Cochrane Library 2012, Issue 4

7
OS : ∆ 5.5% at 6y ∆ 8.8% at 10y DFS : ∆ 11.9% at 6y ∆ 11.5% at 10y

8
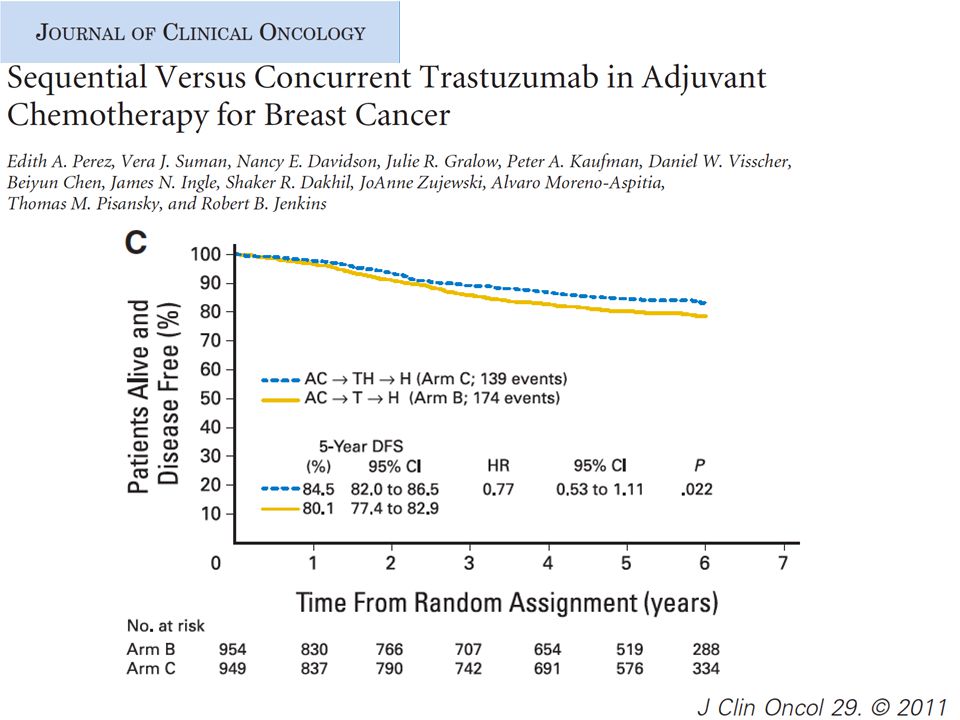
Are all trastuzumab adjuvant trials the same? BCIRG 006 DC x 6+ H AC x 4D x 4+ H Trastuzumab up to 1 yr FIN-HER D/N+H x 9 wks FECx 3 HERA Adjuvant CT (Any) RT N9831 Sequential arm wT x 12 AC x 4 Joint analysis of NSABP B31 & N9831 AC x 4T x 4 + H PACS 04 FEC/ED x 6 RT RandomizationTrastuzumab start T= paclitaxel; D= docetaxel Concurrent administration Sequential administration
 RT N9831 Sequential arm wT x 12 AC x 4 Joint analysis of NSABP B31 & N9831 AC x 4T x 4 + H PACS 04 FEC/ED x 6 RT RandomizationTrastuzumab start T= paclitaxel; D= docetaxel Concurrent administration Sequential administration.")
9
Moja L, et al. The Cochrane Library 2012, Issue 4 Overall Survival stratified by concurrent or sequential administration

12
Trastuzumab plus chemotherapy: the gold standard for HER2 positive early breast cancer Improving on cardiac toxicity: different regimens and different treatment durations Improving on treatment efficacy: dual blockade and new anti-HER2 agents Toward personalized cancer medicine: challenging the gold standard for specific patient subgroups Outline

13
Low competing mortality risk score High competing mortality risk score Cancer ahead pub 2010

14
Congestive heart failure (CHF): all studies. Moja L, et al. The Cochrane Library 2012, Issue 4
: all studies. Moja L, et al. The Cochrane Library 2012, Issue 4")
15
LVEF decline-all studies.

16
BCIRG 006: Adjuvant Breast Cancer Node Positive and High Risk Node Negative 4x AC 60/600 mg/m 2 4x Docetaxel 100 mg/m 2 HER2+ (central FISH) N+ or High risk N- N=3,222 pts 6 x Docetaxel 75 mg/m 2 +Carboplatin AUC 6 1 Year Trastuzumab AC T AC TH TCH
 N+ or High risk N- N=3,222 pts 6 x Docetaxel 75 mg/m 2 +Carboplatin AUC 6 1 Year Trastuzumab AC T AC TH TCH")
17
Slamon D, NEJM 2011.

19
Slamon et al. SABCS 2006. Abstract 52. Slamon D, NEJM 2011.

20
Moja L, et al. The Cochrane Library 2012, Issue 4 CHF by trastuzumab duration

21
Moja L, et al. The Cochrane Library 2012 DFS by trastuzumab duration Log (Hazard ratio)HR weight HR (IV,random, 95%CI)
HR weight HR (IV,random, 95%CI).")
22
Overall survival stratified by duration of trastuzumab treatment Moja L, et al. The Cochrane Library 2012, Issue 4

26
SABCS, 2012

29
www.esmo2012.org PHARE* Trial results comparing 6 to 12 months of trastuzumab in adjuvant early breast cancer Xavier Pivot, Gilles Romieu, Hervé Bonnefoi, Jean-Yves Pierga, Pierre Kerbrat, Thomas Bachelot, Alain Lortholary, Marc Espié, Pierre Fumoleau, Daniel Serin, Jean-Philippe Jacquin, Christelle Jouannaud, Maria Rios, Sophie Abadie-Lacourtoisie, Nicole Tubiana-Mathieu, Laurent Cany, Stéphanie Catala, David Khayat, Iris Pauporté, Andrew Kramar. Protocol of Herceptin ® Adjuvant with Reduced Exposure *lighthouse in French

30
www.esmo2012.org Study design trastuzumab 6 months trastuzumab up to 12 months stop trastuzumab Clinical exam LVEF 3 Mammography 69121518212430 mos … 0 R R R: Randomization after informed consent Up to 60 mos… Stratification 1. ER pos / neg 2. Chemo: conco/ seq

31
www.esmo2012.org Statistical Methods Non inferiority randomized trial – 2% variation in terms of absolute difference of recurrence – The 95% CI HR margins should not cross the 1.15 boundary – 1040 DFS events required for 80% power at 5% level or 4 years of accrual and at least 2 years of follow-up – HR were estimated from the stratified Cox model Accrual target: 3400 patients

32
www.esmo2012.org Primary endpoint scenarii

33
www.esmo2012.org Patient Characteristics 12 months n=1690 6 months n=1690 Age, median (range)54 (21 – 86)55 (23 – 85) Tumor : 0 – 2 cm 2 – 5 cm >5 cm 54.7% 38.5% 6.8% 52.4% 39.8% 7.8% Nodes: negative 1 – 3 nodes 4 nodes 55.4% 30.0% 14.6% 54.7% 30.2% 15.1% Positive Estrogen receptor57.6%58.8% Inflammatory disease3.5%3.4% SBR:I II III 3.1% 41.0% 55.6% 3.3% 40.9% 55.8%
54 (21 – 86)55 (23 – 85) Tumor : 0 – 2 cm 2 – 5 cm >5 cm 54.7% 38.5% 6.8% 52.4% 39.8% 7.8% Nodes: negative 1 – 3 nodes 4 nodes 55.4% 30.0% 14.6% 54.7% 30.2% 15.1% Positive Estrogen receptor57.6%58.8% Inflammatory disease3.5%3.4% SBR:I II III 3.1% 41.0% 55.6% 3.3% 40.9% 55.8%")
34
www.esmo2012.org Treatment Characteristics 12 months n=1690 6 months n=1690 Type of Chemotherapy : No Anthracyclines Anthracyclines no Taxanes Anthracyclines and Taxanes 10.2% 15.9% 73.9% 11.8% 15.5% 72.7% Concomitant Chemotherapy Sequential Chemotherapy 57.8% 42.2% 57.7% 42.3% Radiotherapy87.7%88.2% Hormonotherapy50.6%50.2% Trastuzumab duration, mean (sd)11.8 (6.3)6.3 (1.46)
11.8 (6.3)6.3 (1.46)")
35
www.esmo2012.org Cardiac toxicity 12 months (n=1690) 6 months (n=1690) P Cardiac events*5.7%1.9%<0.0001 LVEF** < 50%6.3%4.7%0.04 LVEF** 10% 4.8%3.6%0.071 LVEF** > 50% and > 15% 7.4%7.0%NS * Investigator reported events (composite with clinical and LFEV finding) ** Based on more than > 25,000 assessments
 6 months (n=1690) P Cardiac events*5.7%1.9%< LVEF** < 50%6.3%4.7%0.04 LVEF** 10% 4.8%3.6%0.071 LVEF** > 50% and > 15% 7.4%7.0%NS * Investigator reported events (composite with clinical and LFEV finding) ** Based on more than > 25,000 assessments")
36
www.esmo2012.org DFS Events 12 mos (n=1690) 6 mos (n=1690) DFS Events (n=395)10.4%13.0% Local Recurrence Regional Recurrence Distant Recurrence Controlateral Breast Cancer 2 nd Primary Malignancy Death 1.1% 0.6% 6.4% 0.4% 1.5% 0.4% 1.4% 0.5% 8.3% 0.7% 1.5% 0.5% 42.5mos. median Follow-up

37
www.esmo2012.org Disease Free Survival * Cox model stratified by ER status and concomitant chemotherapy 95.5 91.2 87.8 84.9 97.0 93.8 90.7 87.8 Events HR 95%CIp-value H 12m 176 H 6m 219 1.28 (1.05 – 1.56) 0.29
 0.29")
38
www.esmo2012.org Overall Survival * Cox model stratified by ER status and concomitant chemotherapy 42.5mos. median FU 99.3 97.2 95.2 93.1 99.9 98.7 96.9 95.0 Events HR 95%CIp-value H 12m 66 H 6m 931.47(1.07 – 2.02)
.")
39
www.esmo2012.org Equivalent Superior Non Inferior Inferior A B C D E.8511.151.31.451.6 HR Primary endpoint scenarii PHARE trial

40
Trastuzumab duration effects in patient subgroups in the PHARE* trial Protocol of Herceptin ® Adjuvant with Reduced Exposure *lighthouse in French Xavier Pivot, Gilles Romieu, Hervé Bonnefoi, Jean-Yves Pierga, Pierre Kerbrat, Thomas Bachelot, Alain Lortholary, Marc Espié, Pierre Fumoleau, Daniel Serin, Jean-Philippe Jacquin, Christelle Jouannaud, Maria Rios, Sophie Abadie-Lacourtoisie, Nicole Tubiana-Mathieu, Laurent Cany, Stéphanie Catala, David Khayat, Iris Pauporté, Andrew Kramar. SABCS 2012

41
Subgroup Results ER- status & Sequential modality Other groups

42
Short-HER: study design R RT/HT Trastuzumab 4 mg/kg loading dose 2 mg/kg weekly 3 mos6 mos 9 mos 12 mos 18 mos : LVEF measurement PI: PF Conte Sample size 1250 pts FEC (600/60/600) AC60/600 or EC90/600 Trastuzumab 8 mg/kg loading dose 6 mg/kg q 3 wks Docetaxel 100 EUDRACT-2007-004326-25, NCT00629278
 AC60/600 or EC90/600 Trastuzumab 8 mg/kg loading dose 6 mg/kg q 3 wks Docetaxel 100 EUDRACT , NCT")
43
Enrollment as of May, 2013 1176 patients –Arm A (Long) 586 patients –Arm B (Short) 590 patients
 586 patients –Arm B (Short) 590 patients")
44
Trastuzumab plus chemotherapy: the gold standard for HER2 positive early breast cancer Improving on cardiac toxicity: different regimens and different treatment durations Improving on treatment efficacy: new anti-HER2 agents and multiple dual blockade Toward personalized cancer medicine: challenging the gold standard for specific patient subgroups Outline

45
TEACH Trial Placebo qd × 1 yr Lapatinib 1500 mg qd × 1 yr Stratification Time from diagnosis ≤4 vs >4 yrs Lymph node +ve vs -ve ER+ and/or PgR+ vs ER–/PgR– 4 yr Eligibility HER2+ Local IHC3+ or FISH +ve Resected Stage I-IIIc primary BRCA No prior trastuzumab Neo-/adjuvant chemotherapy (CMF, anthracycline, or taxane) Appropriate endocrine therapy N=3147 Aug 2006-May 2008 33 countries RANDOMIZERANDOMIZE Diagnosis Disease-free survival (DFS):local, regional, distant recurrence,contralateral BRCA,other 2 nd primary cancers,death from any cause Goss, SABCS 2011
 Appropriate endocrine therapy N=3147 Aug 2006-May countries RANDOMIZERANDOMIZE Diagnosis Disease-free survival (DFS):local, regional, distant recurrence,contralateral BRCA,other 2 nd primary cancers,death from any cause Goss, SABCS 2011")
46
0.0 TEACH Primary Endpoint: K-M Plot of DFS in ITT Population—Time From Randomization a p value based on 2-sided stratified log-rank test Lapatinib Placebo HR 0.83 (0.70-1.00); p=0.053 a Median Follow up: 4 years Number of patients at risk Lapatinib 1500 mg 1571143113491293123311681001661299 Placebo1576148714121343129512471048706327 No improvement in OS demonstrated with use of lapatinib: HR: 0.99 (95% CI: 0.74-1.31; P =.966) Goss, SABCS 2011
; p=0.053 a Median Follow up: 4 years Number of patients at risk Lapatinib 1500 mg Placebo No improvement in OS demonstrated with use of lapatinib: HR: 0.99 (95% CI: ; P =.966) Goss, SABCS 2011")
47
TEACH: Forest Plot of DFS for Subgroups in ITT Population L=lapatinib; P=placebo. Goss, SABCS 2011

48
Phase III NeoALLTO study Phase II CHER-LOB study Dual anti-HER2 blockade (neoadjuvant studies)
")
49
Baselga J et al. Lancet 2012 Guarneri V et al, J Clin Oncol 2012 pCR (breast & axilla) 0 10 20 30 40 50 60 Arm A: CT + TArm B: CT + L Arm C: CT + T + L Exploratory p=0.0187 Dual Anti-HER2 blockade significantly increases the pCR rate 25%26.3% 46.7%
 Arm A: CT + TArm B: CT + L Arm C: CT + T + L Exploratory p= Dual Anti-HER2 blockade significantly increases the pCR rate 25%26.3% 46.7%.")
50
ALTTO study design (8000 patients)
")
53
Aphynity R 6-8 cycles Adj CHT 6-8 cycles Adj CHT 52 weeks Trastuzumab i.v. 8 mg/kg LD then 6 mg/kg, q3w Pertuzumab 840 mg i.v. LD then 420 mg, q3w Placebo i.v., q3w HER2+ BC N+ or high-risk N0 Expected enrollment: 3806 pts T, P/Pl concomitant to taxane-based CT IBCSG 39-11 / BIG 4-11 (APHINITY)
.")
54
Trastuzumab plus chemotherapy: the gold standard for HER2 positive early breast cancer Improving on cardiac toxicity: different regimens and different treatment durations Improving on treatment efficacy: dual blockade and new anti-HER2 agents Toward personalized cancer medicine: challenging the gold standard for specific patient subgroups Outline

55
Authormedian FUCohort#Relapses %P value Amar S SABCS 20073 y. HR+/HER2-3501.3 0.007 HER2+277.4 TN2412.5 Zambelli A AIOM 2008 4 y.HER2-3093 0.038 HER2+3113 Ananthakrishnan P SABCS 2008 4 y.HER2- 770 3.0 ns HER2+9.0 Tovey SM SABCS 2008 5 y.HER2-3094 0.001 HER2+5832 Curigliano G JCO 2009 4.6 yHR+/HER2-1581.3 0.09 HER2+/HR-717 HER2+/HR+797.6 TN717 Gonzalez-Angulo A JCO 2009 6.2 yHER2-8675.9 <0.001 HER2+9821.4 Outcome of HER2+ T1a,b N0 tumors (w/o Trastuzumab )
.")
56
Trastuzumab Adjuvant trials: subset analysis N = node 1–3+ nodes 00.52.51.01.52.0 1–3+ nodes ≥4+ nodes Not assessed N9831/B-31 N– 4–9+ nodes >10+ nodes TCH N– N+ BCIRG 006 N– AC TH N– HERA Favours trastuzumabFavours no trastuzumab HR Slamon, et al. SABCS 2006 Perez, et al. ASCO 2007; Smith, et al. Lancet 2007 32 % N0 7% N0 29% N0

57
Characteristic Adjuvant trastuzumab trials (B31/N9831/HERA/FinHer/BCIRG006/PACS04) Modena Cancer Registry Age (median) 4959 T1N0 %~ 238.8 HER2+ EBC patients Adjuvant trastuzumab trials vs Modena Cancer Registry Piccart N Engl J Med 2005; Romond N Engl J Med 2005; Joensuu N Engl J Med 2006; Slamon D, SABCS 2006; Spielmann M et al, SABCS 2007; Federico M, RTM 1998-2009
 Modena Cancer Registry Age (median) 4959 T1N0 %~ HER2+ EBC patients Adjuvant trastuzumab trials vs Modena Cancer Registry Piccart N Engl J Med 2005; Romond N Engl J Med 2005; Joensuu N Engl J Med 2006; Slamon D, SABCS 2006; Spielmann M et al, SABCS 2007; Federico M, RTM")
58
pCR by Hormone Receptor Status Baselga J et al. SABCS 2010; Gianni et al, SABCS 2010, Guarneri et al, ASCO 2011 pCR rate* HR +HR - Neo-ALLTOLapatinib (L) +paclitaxel16.2%33.8% Trasuzumab (T) +paclitaxel22.7%36.5% L+T+ paclitaxel41.6%61.3% Cher-LOBL + P-FEC22.7%35.7% T + P-FEC25%26.6% L+T+ P-FEC35.7%56.2% Neo-SphereDocetaxel-T20%36.8% Docetaxel + T+ Pertuzumab26%63.2% T+pertuzumab5.9%29.1% Docetaxel + pertuzumab17.4%30%
 +paclitaxel16.2%33.8% Trasuzumab (T) +paclitaxel22.7%36.5% L+T+ paclitaxel41.6%61.3% Cher-LOBL + P-FEC22.7%35.7% T + P-FEC25%26.6% L+T+ P-FEC35.7%56.2% Neo-SphereDocetaxel-T20%36.8% Docetaxel + T+ Pertuzumab26%63.2% T+pertuzumab5.9%29.1% Docetaxel + pertuzumab17.4%30%.")
59
Chang, JCO 2013 Neoadjuvant trastuzumab + lapatinib w/o chemotherapy

60
Summary of HER2+ EBC CT+ 1yr trastuzumab is the standard regimen Studies evaluating optimal trastuzumab duration in terms of efficacy and safety are critical: to take into account the sustainability for the NHS to facilitate the introduction of new antiHER2 treatments Neoadjuvant studies are essential to rank treatment activity, prior to move to large adjuvant studies A dual HER2 inhibition seems a winner strategy New promising agents are entering the adjuvant phase The possibility to avoid chemotherapy in case of small T size, N0, HR+, elderly and frail patients is intriguing, but still matter of study

Similar presentations











 Phase III trial comparing AC (x4)taxane (x4) with taxane (x8) as adjuvant therapy for node-positive breast cancer: Results of N-SAS-BC02.>")



 on the Efficacy.>")


 in combination with chemotherapy: pivotal metastatic breast cancer survival data 1.>")



: a randomised phase 3 trial Speaker: 陳鴻明.>")





