Download presentation
Presentation is loading. Please wait.

1
Andres Ferber MD September 15 2009
Vitamin K and Coumadin Andres Ferber MD September

2
Coumadin is an anticoagulant because….
It inhibits blood coagulation It prevents the (protein) synthesis of factors 2,7,9,10 Its action results in hypo functioning factors 2,7,9,10 All of the above
 synthesis of factors 2,7,9,10. Its action results in hypo functioning factors 2,7,9,10. All of the above.")
3
Vitamin K

4
Gamma Carboxylation Introduction of an additional carboxylic group in the position gamma of glutamic acid The vitamin K dependent factors; II,VII, IX,X,Protein C,Protein S,Protein Z and the Bone proteins; Bone Gla protein and Matrix Gla protein have a Gla domain where several glutamic acids are clustered and get gamma carboxylated. Other proteins including GAS-6 (growth arrest protein), two thyroid and spinal cord proteins and certain peptide toxin from mollusks contain Gla domains. In the coagulation factors gamma carboxylation increases Calcium binding. Upon Ca++ binding a conformational change of the molecule occurs exposing an three hydrophobic residues that are responsible for phospholipid membrane binding. This in turn produces a marked increased in the activity of the factor.
, two thyroid and spinal cord proteins and certain peptide toxin from mollusks contain Gla domains. In the coagulation factors gamma carboxylation increases Calcium binding. Upon Ca++ binding a conformational change of the molecule occurs exposing an three hydrophobic residues that are responsible for phospholipid membrane binding. This in turn produces a marked increased in the activity of the factor.")
5
Anticoagulant factors
Procoagulant factors Anticoagulant factors

6
Gamma Carboxylation gCarboxylase gCarboxylation in Progress mRNA
Endoplasmic Reticulum gCarboxylase mRNA gCarboxylation in Progress

7
Gamma Carboxylation gCarboxylation in Progress
Last gCarboxylation Event

8
Cleavage of the propetide peptide
Golgi Ca++

9
Enzyme/Cofactor/membrane complex activation vs “activation”
Vitamin K dependent factor Ca++ gCarboxylation

10
F X VIIa+TF Va Ca++ F Xa Ca++ F Xa Ca++

11
The carboxylation reaction
The vitamin K dependent carboxylase requires Oxigen and Uses CO2 as a source of carbon. The reduced vitamin K is converted to the epoxide during the reaction. The vitamin K dependent step is the removal of the H from the gamma carbon,the reduced vitamin K is the oxygen acceptor in the step and gets oxydized. The carboxylase has a glutamate and a propeptide binding sites. Both carboxylation and epoxidase activity are in the same protein.

12
The Gammacarboxylation reaction
Vitamin K Hydroquinone Vitamine K Epoxide gCarboxyglutamate Glutamate O2 CO2

14
Recycling of vitamin K After forming part of the polypeptide and after proteolyis free gamma carboxyglutamic acid enters the circulation and it is not re-used.It is excreted in the urine.Therefore there is a 1:1 ratio of the number of Gla residues and the conversion of KH2 into KO. On the basis of nutritional intake of vitamin K and urinary Gla excretion it can be calculated that the number of carboxylation events exceeds the number of vitamin K molecules by several thousand folds. Vitamin K is recycled The enzyme KO reductase accomplishes that function.

15
gCarboxyglutamate Recycling of Vitamin K VKOR Glutamate O2 CO2
Hydroquinone Vitamine K Epoxide gCarboxyglutamate Glutamate O2 CO2

16
Coumadin

17
Coumadin Coumadin interferes with KO reductase
Recycling of KO is blocked and results in exhaustion of KH2 stores resulting in apparent vitamin K deficiency

18
Mechanism of action of warfarin
VKOR Vitamin K Hydroquinone Vitamine K Epoxide X gCarboxyglutamate Glutamate O2 CO2

19
Coumadin Because conversion of vitamin K to KH2 is not affected the coumadin effect can be bypassed by administration of exogenous vitamin K

20
Exogenous vitamin K can revert coumadin effect
Warfarin VKOR Exogenous Vitamin K Vitamin K Hydroquinone Vitamine K Epoxide gCarboxyglutamate Glutamate O2 CO2

21
Vitamin K1 is reduced to vitamin KH2
Vitamin K1 is reduced to vitamin KH2. The major warfarin-sensitive enzyme in this reaction is the vitamin K oxide reductase mainly inhibited by the S enantiomer of warfarin. S-warfarin is metabolized by the p450 cytochrome enzyme, CYP2C9. Ansell J et al. Chest 2008;133:160S-198S ©2008 by American College of Chest Physicians

22
VKOR genetic polymorphisms
Warfarin Sensitive Warfarin Resistant

24
Coumarins Most clinically used coumarins have relatively short half life acenocoumarol 10hs warfarin 40hs phenprocoumon 100hs Rodents have developped resistance to this first generation coumarins by mutating their KO reductase to a form that has less affinity for coumarins Second generation coumarins or super warfarins are used now as rodenticides.Their half life is 6 months or more. Treatment of intoxication with these products may require high doses of vitamin K (up to 200mg/day) for several years.
 for several years.")
26
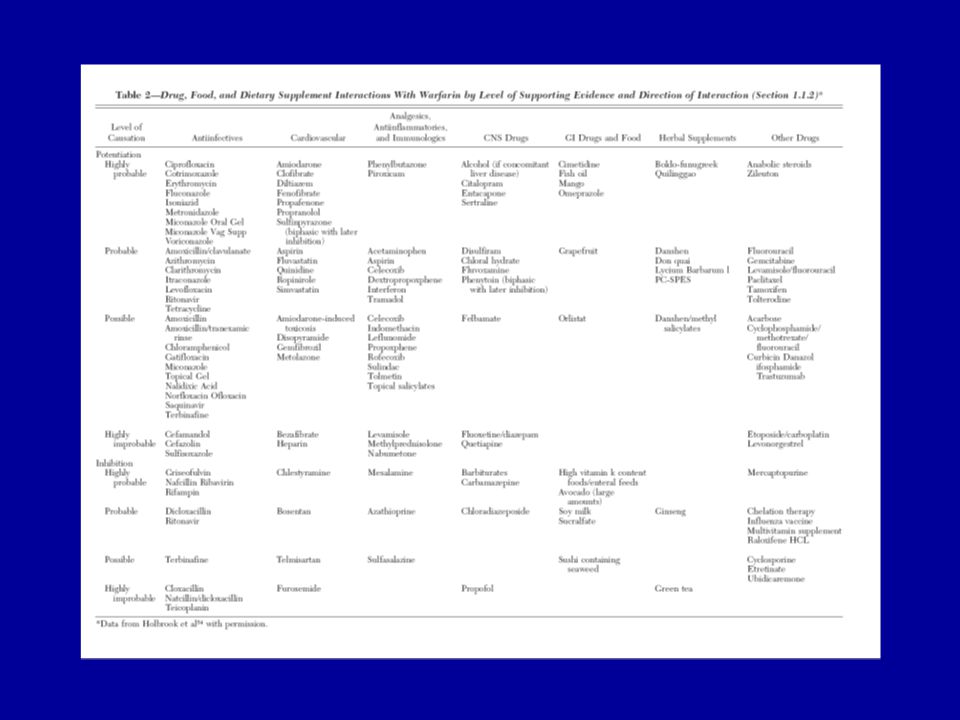
My patient INR is too high What to do?

27
My patient INR is too high What to do?
Condition Intervention INR more than therapeutic range but < 5.0; no significant bleeding Lower dose or omit dose; monitor more frequently and resume at lower dose when INR therapeutic; if only minimally above therapeutic range, no dose reduction may be required (Grade 1C). INR ≥ 5.0, but < 9.0; no significant bleeding Omit next one or two doses, monitor more frequently, and resume at an appropriately adjusted dose when INR in therapeutic range. Alternatively, omit dose and give vitamin K (1–2.5 mg po), particularly if at increased risk of bleeding (Grade 1C). If more rapid reversal is required because the patient requires urgent surgery, vitamin K (≤ 5 mg po) can be given with the expectation that a reduction of the INR will occur in 24 h. If the INR is still high, additional vitamin K (1–2 mg po) can be given (Grade 2C). INR ≥ 9.0; no significant bleeding Hold warfarin therapy and give higher dose of vitamin K (2.5–5 mg po) with the expectation that the INR will be reduced substantially in 24–48 h (Grade 1B). Monitor more frequently and use additional vitamin K if necessary. Resume therapy at an appropriately adjusted dose when INR is therapeutic. Serious bleeding at any elevation of INR Hold warfarin therapy and give vitamin K (10 mg by slow IV infusion), supplemented with FFP, PCC, or rVIIa, depending on the urgency of the situation; vitamin K can be repeated q12h (Grade 1C). Life-threatening bleeding Hold warfarin therapy and give FFP, PCC, or rVIIa supplemented with vitamin K (10 mg by slow IV infusion). Repeat, if necessary, depending on INR (Grade 1C). Administration of vitamin K In patients with mild to moderately elevated INRs without major bleeding, give vitamin K orally rather than subcutaneously (Grade 1A).
. INR ≥ 5.0, but < 9.0; no significant bleeding. Omit next one or two doses, monitor more frequently, and resume at an appropriately adjusted dose when INR in therapeutic range. Alternatively, omit dose and give vitamin K (1–2.5 mg po), particularly if at increased risk of bleeding (Grade 1C). If more rapid reversal is required because the patient requires urgent surgery, vitamin K (≤ 5 mg po) can be given with the expectation that a reduction of the INR will occur in 24 h. If the INR is still high, additional vitamin K (1–2 mg po) can be given (Grade 2C). INR ≥ 9.0; no significant bleeding. Hold warfarin therapy and give higher dose of vitamin K (2.5–5 mg po) with the expectation that the INR will be reduced substantially in 24–48 h (Grade 1B). Monitor more frequently and use additional vitamin K if necessary. Resume therapy at an appropriately adjusted dose when INR is therapeutic. Serious bleeding at any elevation of INR. Hold warfarin therapy and give vitamin K (10 mg by slow IV infusion), supplemented with FFP, PCC, or rVIIa, depending on the urgency of the situation; vitamin K can be repeated q12h (Grade 1C). Life-threatening bleeding. Hold warfarin therapy and give FFP, PCC, or rVIIa supplemented with vitamin K (10 mg by slow IV infusion). Repeat, if necessary, depending on INR (Grade 1C). Administration of vitamin K. In patients with mild to moderately elevated INRs without major bleeding, give vitamin K orally rather than subcutaneously (Grade 1A).")
28
PCCs (Replace factors)
Prothrombin Complex Concentrates Variable amount of vit K factors including IX Variable amounts of factor VII No activated factors Heparin Natural anticoagulants

29
Recombinant factor VIIa (Activates Blood Coagulation X to Xa)
")
30
Tissue Factor Bearing cell
TISSUE FACTOR BEARING STRUCTURE Tissue Factor Bearing cell

31
Mode of Action

Similar presentations