Download presentation
Presentation is loading. Please wait.

1
Recurrent And De Novo GN After Renal Transplantation

2
Introduction The 1 year kidney allograft survival rate has
improved dramatically during the last decade with the introduction of newer IS agents Development and progression of recurrent and de novo disease does not seem to have been influenced by the use of those agents

3
Introduction Clinically, recurrent GN manifests primarily as
an increase in proteinuria in the allograft, usually associated with progressive loss of renal function or chronic kidney disease (CKD).
.")
4
Introduction 30- 50 % of KT recipients have GN as the
underlying cause of their ESRD Those patients are at risk of the recurrence of their original disease.

5
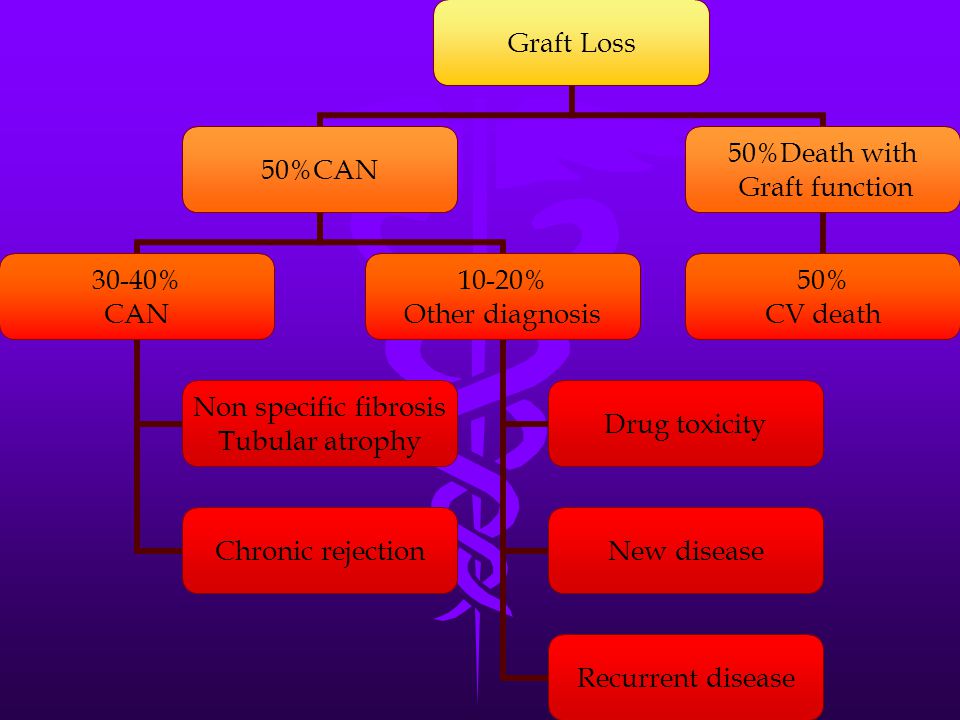
Introduction Among these patients, more than 40% develop
significant proteinuria, and around 15% develop persistent nephrotic syndrome The most common cause of post transplantation proteinuria is chronic allograft nephropathy (50%), followed by recurrent (15%) and de novo (10%) glomerulonephritis
, followed by recurrent (15%) and de novo. (10%) glomerulonephritis.")
6
Introduction Persistent proteinurea is associated with a
significantly reduced rate of graft survival but often can be controlled with non-disease specific therapy including ACEI and ARB

7
Introduction In patients who develop recurrent and de novo
disease , there is a 190% increased risk of losing the graft compared with those without recurrent and de novo disease. Glomerulonephritis in the allograft is also associated with a reduction in long-term (5-year) survival
 survival.")
9
Introduction Variables that have been found to be associated
with recurrence included younger age, male gender, underlying GN as a cause of ESRD and retransplants Higher prevalence in young ages is probably explained by the more frequent occurrence of GN in this group.

10
Introduction No penalty paid in terms of increased recurrence
of GN for recipients who received their transplants for GN and were maintained on steroids-free IS regimen.

12
Focal glomerular sclerosis
FGS is the disease entity that carries the highest incidence of clinically significant recurrent disease with the greatest impact on graft survival of any of the glomerular diseases

13
Focal glomerular sclerosis
The overall recurrence rate in FGS is about 30% 50% of these grafts are lost from recurrent disease in 5 years .

14
Focal glomerular sclerosis
The mean time to recurrence of FGS is short, 10- 14 days, but recurrences have been reported within hours and up to 6 months after transplantation.

15
Focal glomerular sclerosis
Up to 50% of patients with recurrent FGS also develop acute renal failure, 80% become nephrotic, and hypertension and hematuria are common

16
Focal glomerular sclerosis
Clearly, recurrence is more common in younger patients. Patients under 5 years of age have a 50% likelihood of recurrence versus only 10%-15% in patients older than 30 years

17
Focal glomerular sclerosis
Caucasian recipients seem more likely to have recurrences than African-Americans. Rapid progression of the underlying disease from initial diagnosis to development of ESRD, particularly if it occurs within 3 years, also predicts recurrence.

18
Focal glomerular sclerosis
Recurrence itself is a very bad prognostic sign that predicts recurrence in second allograft. Over 70% of such grafts have another recurrence and most are lost. Thus, a history of graft loss from recurrent FGS virtually precludes subsequent successful transplantation in that recipient.

19
Focal glomerular sclerosis
The pathogenesis of FGS is unclear, however a circulating permeability factor that is removed by plasmaphresis has been suspected to play a role However recent data suggested the absence or loss of an inhibitor factor could be the cause

20
Focal glomerular sclerosis
Further complicating the picture is the recognition of the pivotal role of podocytes proteins(podocin, nephrin, and actinin) in FSG
 in FSG.")
21
Focal glomerular sclerosis
Early institution of plasmaphresis is important as the effectiveness of treatment decreases with increased number of sclerosed glomeruli. Relapses after cessation of plasmaphresis can be prevented by chronic phresis or concurrent cyclosporine or cyclophosphamide therapy

22
Focal glomerular sclerosis
The role of preemptive perioperative plasmaphresis in high risk groups still awaits further studies. There is one recent case report of complete remission of FSG with rituximab

23
Focal glomerular sclerosis
A number of case reports reported the development of de novo FSG when cyclosporine was switched to sirolimus with subsequent improvement after switching back to cyclo. Paradoxically sirolimus has achieved complete remission in 12 out of 21 steroid resistant FSG in another study

24
Membranous Nephropathy
Secondary causes of MN (infection, malignancy… etc) should be screened Idiopathic MN recurs in 10-30% Recurrent disease should be differentiated from de novo disease which is the most common de novo GN in renal allograft
 should be screened. Idiopathic MN recurs in 10-30% Recurrent disease should be differentiated from. de novo disease which is the most common de. novo GN in renal allograft.")
25
Membranous Nephropathy
The clinical presentation of recurrent MN is characterized by nephrotic range proteinuria with a mean onset time of (10-24) months post- transplant as compared with the more insidious and later onset of de novo MN (24-36) months
 months post- transplant as compared with the more insidious. and later onset of de novo MN (24-36) months.")
26
Membranous Nephropathy
Recent studies showed antibodies against ‘neutral endopeptidase’, a protein expressed on the human podocyte cell membrane might be playing a role in MG Risk factors for recurrence include male sex, rapid course of initial disease and LRD kidneys Graft failure from recurrence is 10-15%

27
Membranous Nephropathy
Cyclosporine and MMF which have been used in the treatment of primary MN do not prevent or change the course of recurrent disease No reports to suggest superiority of tacrolimus or cyclophosphamide over cyclosporine

28
MPGN Secondary causes of MPGN should be treated to
reduce the risk of recurrence. Type I and II primary MPGN have high rate of recurrence after transplantation, 20-50% and 80- 100 %respectively

29
MPGN Risk of recurrence increases in those with HLA-
B8DR3, LRD and previous graft loss due to MPGN Recurrent disease is more common in type II and presents with non-nephrotic range proteinurea Complement level has nothing to do with the risk of recurrence

30
MPGN Type II usually has more aggressive golmerular
changes and a poorer prognosis No effective therapy is available

31
Pauci-Immune Crescentic GN
Pretransplantation course, cANCA, pANCA titer, disease subtype(WG, MPAN or CGN) in the absence of clinically active disease, duration of follow up or donor type, do not predict recurrence. Recurrence rate is around 20%
 in the. absence of clinically active disease, duration of. follow up or donor type, do not predict. recurrence. Recurrence rate is around 20%")
32
Pauci-Immune Crescentic GN
It is advisable to defer transplant until the disease is inactive Patients with renal relapses showed good response to cyclophopsphamide.

33
Pauci-Immune Crescentic GN
For patients with cellular crescent and high ANCA titer, favorable outcome has been reported with combined cyclophosphamide, plasmaphresis with or without intravenous immunoglobulin

34
SLE Histological recurrence has been reported in 30%
Clinically significant recurrence occurs in 2-9% Most center postpone re-transplant until the disease is quiescent for 6-9 months

35
SLE The duration of dialysis before transplantation
and the serological markers in the absence of clinically active disease do not predict recurrence MMF has been shown to be very efficient. Graft loss due to recurrent lupus is uncommon, 2-4%

36
SLE Long term patients and graft survival are similar
to kidney allograft recipients with other underlying disease.

37
Anti-GBM Histological recurrence has been reported in 50%
if transplantation is performed while circulating anti-GBM antibodies are still present Defer transplantation until the disease become quiescent and the anti-GBM antibodies become undetectable for 12 months

38
Anti-GBM Good response has been reported in one patient
with steroids, plasmaphresis and cyclophosphamide, another patient responded well to immune adsorption and cyclophosphamide

39
Immunoglobulin A Nephropathy
IgAN is the commonest GN worldwide and accounts for 20 % of renal failure of all renal transplant cases. Great variation in the incidence of recurrence has been reported by many centers as most centers perform biopsies only when patients are symptomatic, underestimating the real number

40
Immunoglobulin A Nephropathy
For centers where routine biopsies were being carried out, histological recurrence had been reported in % Recurrence rate for patients with renal biopsies done for clinical symptoms ranges from 13-50%

41
Immunoglobulin A Nephropathy
Recurrent disease is not as benign as had been reported previously Graft loss from the severest form ranges from 1.3 to 16 % No single parameter including age, gender, race, HLA or biochemical characteristic can predict recurrence

42
Immunoglobulin A Nephropathy
The relationship between recurrence and donor type remains controversial except in the familial form of IgAN where recurrence is high in LRD cases Renal allograft survival in the first 10 years after transplantation is better when compared to other primary disease

43
Immunoglobulin A Nephropathy
The situation is different for patients with prior graft loss due to IgAN where the recurrence risk in the second transplant is %, and patients should be excluded from LRD list There is no effective therapy to prevent recurrent IgAN

44
Immunoglobulin A Nephropathy
Despite initial enthusiasm about MMF, recent data are not substantiated Data on sirolimus is limited Steroids-free or rapid steroid withdrawal regimen does not seem to affect recurrence risk

45
Immunoglobulin A Nephropathy
ACE-I and ARB are used in proteinuric patients. HSP recurrence rate after transplantation is similar to IgAN

46
Conclusion With improving long-term renal allograft
survival, recurrent disease has increased prominence as a significant contributor to late graft loss. Knowledge of the risk factors for recurrence, onset time and impact on graft function is prerequisite to informed decisions

47
Conclusion Apart from plasmaphresis for patients
with recurrent FSGS, there is no consensus on Strategies to prevent or treat recurrent glomerular disease in the kidney allograft.

48
Conclusion Also, in spite of the controversy over the risk of
recurrence with certain types of glomerulonephritis when the source of allograft is from living donors, the graft survival is largely comparable to patients with other causes of end- stage renal failure. Thus, living related kidney Donation can still be encouraged

49
Conclusion Caution should be exercised in patients
with previous rapid graft loss due to recurrent disease in view of the markedly increased risk with subsequent transplants.

Similar presentations