Download presentation
1
SPINAL CORD INJURIES Anatomy & Pathophysiology
J C King

2
Definition Insult to spinal cord resulting in a change,
in the normal motor, sensory or autonomic function. This change is either temporary or permanent.

3
Mechanisms: Direct trauma Compression by bone fragments / haematoma / disc material Ischemia from damage / impingement on the spinal arteries

4
Statistics: National Spinal Cord Injury Database { USA Stats }
MVA % Falls % Violence % Sports % 55% cases occur in 16 – 30yrs of age 81.6% are male!

5
South African Statistics (GSH Acute Spinal Cord Injury Unit 2007)
MVA % Falls % Gunshot Injuries 11% Blunt Assault 6% Diving Accidents 5% Stab Wounds 4% Sport Injuries 3%

6
Other causes: Vascular disorders Tumours Infectious conditions Spondylosis Iatrogenic Vertebral fractures secondary to osteoporosis Development disorders

7
Anatomy : Spinal cord: Extends from medulla oblongata – L1
Lower part tapered to form conus medullaris

9
On the surface : Deep anterior median fissure Shallower posterior median sulcus Spinal cord segment : Section of the cord from which a pair of spinal nerves are given off

10
Hence: 31 pairs of spinal nerves:
8 cervical 12 thoracic 5 lumbar 5 sacral 1 coccygeal

12
Dorsal root – sensory fibres
Ventral root – motor fibres Dorsal and ventral roots join at intervertebral foramen to form the spinal nerve

14
Physiology and function
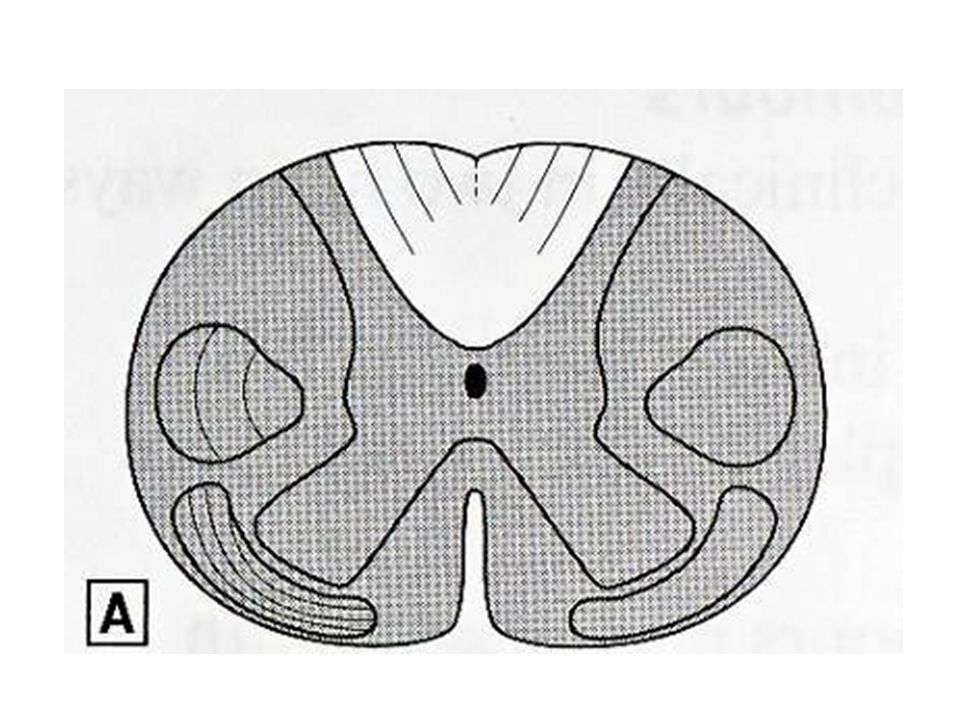
Grey matter – sensory and motor nerve cells White matter – ascending and descending tracts Divided into - dorsal - lateral - ventral

16
Tracts : 1) Posterior column: Fine touch Light pressure Proprioception
 Posterior column: Fine touch Light pressure Proprioception")
17
2) Lateral corticospinal tract :
Skilled voluntary movement 3) Lateral spinothalamic tract : Pain & temperature sensation
 Lateral spinothalamic tract : Pain & temperature sensation.")
18
Posterior column and lateral corticospinal tract crosses over at medulla oblongata
Spinothalamic tract crosses in the spinal cord and ascends on the opposite side NB to understand this as it helps to understand the clinical features of injury patterns and the neurological deficit

19
Dermatomes Area of skin innervated by sensory axons within a particular segmental nerve root Knowledge is essential in determining level of injury Useful in assessing improvement or deterioration

20
Downloaded from: Rosen's Emergency Medicine (on 29 April 2009 06:34 PM)
© 2007 Elsevier

21
Downloaded from: Rosen's Emergency Medicine (on 29 April 2009 06:34 PM)
© 2007 Elsevier

22
Myotomes : Segmental nerve root innervating a muscle
Again important in determining level of injury Upper limbs: C5 - Deltoid C 6 - Wrist extensors C 7 - Elbow extensors C Long finger flexors T Small hand muscles

23
Lower Limbs : L Hip flexors L3,4 - Knee extensors L4,5 – S1 - Knee flexion L5 - Ankle dorsiflexion S1 - Ankle plantar flexion

24
Spinal Cord Injury Classification
Quadriplegia : injury in cervical region all 4 extremities affected Paraplegia : injury in thoracic, lumbar or sacral segments 2 extremities affected

25
Injury either: Complete Incomplete

26
Complete: Loss of voluntary movement of parts innervated by segment, this is irreversible Loss of sensation Spinal shock

27
Incomplete: Some function is present below site of injury More favourable prognosis overall Are recognisable patterns of injury, although they are rarely pure and variations occur

28
Injury defined by ASIA Impairment Scale
ASIA – American Spinal Injury Association : A – Complete: no sensory or motor function preserved in sacral segments S4 – S5 B – Incomplete: sensory, but no motor function in sacral segments

29
C – Incomplete: motor function preserved below level and power graded < 3
D – Incomplete: motor function preserved below level and power graded 3 or more E – Normal: sensory and motor function normal

30
Muscle Strength Grading:
5 – Normal strength 4 – Full range of motion, but less than normal strength against resistance 3 – Full range of motion against gravity 2 – Movement with gravity eliminated 1 – Flicker of movement 0 – Total paralysis

31
Spinal Shock vs Neurogenic Shock
Transient reflex depression of cord function below level of injury Initially hypertension due to release of catecholamines Followed by hypotension Flaccid paralysis Bowel and bladder involved Sometimes priaprism develops Symptoms last several hours to days

32
Neurogenic shock: Triad of i) hypotension ii) bradycardia iii) hypothermia More commonly in injuries above T6 Secondary to disruption of sympathetic outflow from T1 – L2

33
Loss of vasomotor tone – pooling of blood
Loss of cardiac sympathetic tone – bradycardia Blood pressure will not be restored by fluid infusion alone Massive fluid administration may lead to overload and pulmonary edema Vasopressors may be indicated Atropine used to treat bradycardia

35
Types of incomplete injuries
Central Cord Syndrome Anterior Cord Syndrome Posterior Cord Syndrome Brown – Sequard Syndrome Cauda Equina Syndrome

36
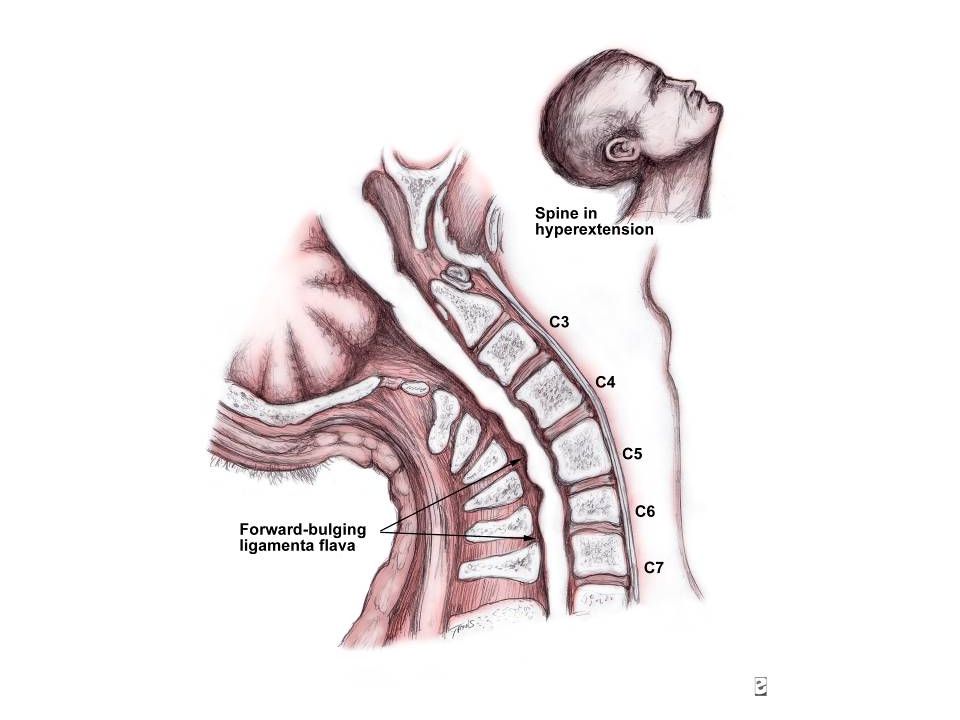
Central Cord Syndrome :
Typically in older patients Hyperextension injury Compression of the cord anteriorly by osteophytes and posteriorly by ligamentum flavum

37
Also associated with fracture dislocation and compression fractures
More centrally situated cervical tracts tend to be more involved hence flaccid weakness of arms > legs Perianal sensation & some lower extremity movement and sensation may be preserved

40
ii) Anterior cord Syndrome:
Due to flexion / rotation Anterior dislocation / compression fracture of a vertebral body encroaching the ventral canal Corticospinal and spinothalamic tracts are damaged either by direct trauma or ischemia of blood supply (anterior spinal arteries)
")
41
Clinically: Loss of power Decrease in pain and sensation below lesion Dorsal columns remain intact

43
ii) Posterior Cord Syndrome:
Hyperextension injuries with fractures of the posterior elements of the vertebrae Clinically: Proprioception affected – ataxia and faltering gait Usually good power and sensation

45
iv) Brown – Sequard Syndrome:
Hemi-section of the cord Either due to penetrating injuries: i) stab wounds ii) gunshot wounds Fractures of lateral mass of vertebrae
 stab wounds. ii) gunshot wounds. Fractures of lateral mass of vertebrae.")
46
Clinically: Paralysis on affected side (corticospinal) Loss of proprioception and fine discrimination (dorsal columns) Pain and temperature loss on the opposite side below the lesion (spinothalamic)
")
48
v) Cauda Equina Syndrome:
Due to bony compression or disc protrusions in lumbar or sacral region Clinically Non specific symptoms – back pain - bowel and bladder dysfunction - leg numbness and weakness - saddle parasthesia

49
In conclusion; Spinal Cord Injuries:
Devastating event to both patient and family. Huge impact on society After receiving First – World care in tertiary institutions, many of our patients return to impoverished communities Here they face huge challenges in terms of survival

50
thank you

51
References: Andrew T Raftery, et al. Applied Basic Science for Basic Surgical Training. Second edition 2008;8: ATLS, et al. Student Course Manual. 7th Edition 2004;7: Keith L Moore et al. Clinically Orientated Anatomy. 3rd Edition1992;4: Segun T Dawodu et al. eMedicine Specialities. March 2009 K Frielingsdorf, R N Dunn et al. SAMJ. March 2007,Vol. 97,No. 3




















 and Nerves. NERVOUS SYSTEM 1.Collect sensory input 2.Integrate sensory input 3.Motor output Functions of Nervous System.>")








