Download presentation
Presentation is loading. Please wait.

1
Setting the standards against which clinical quality can be measured
Dr Gillian Leng Deputy Chief Executive, NICE

2
Areas to cover Confirming best practice – developing Quality Standards
Developing and implementing indicators and metrics NHS Evidence – evidence on best practice and NICE pathways

3
Quality Standards A Quality Standard is a set of specific, concise statements that are markers of high-quality, clinical and cost-effective patient care across a pathway or clinical area Topics sequenced by National Quality Board (NQB) Aim: to offer clarity about what high quality care looks like across the 3 dimensions of quality ensuring: Patient care is effective Patient care considers patient experience Patient care is safe Over time a library of 150 topics is likely to be developed Since April 2009, NICE has been commissioned by the Department of Health to develop independent quality standards. Topics for quality standard development are prioritised and referred to NICE annually by the National Quality Board. The purpose of a NICE quality standard is to make it clear what quality care is by providing definitions of high-quality clinical and cost-effective care. When developing the quality standards, it is important to focus on clinical effectiveness, patient experience and patient safety. The long term aim is to develop a library of around 150 quality standards so that all clinical teams can have access to a quality standard relevant to their specialty.
 Aim: to offer clarity about what high quality care looks like across the 3 dimensions of quality ensuring: Patient care is effective. Patient care considers patient experience. Patient care is safe. Over time a library of 150 topics is likely to be developed. Since April 2009, NICE has been commissioned by the Department of Health to develop independent quality standards. Topics for quality standard development are prioritised and referred to NICE annually by the National Quality Board. The purpose of a NICE quality standard is to make it clear what quality care is by providing definitions of high-quality clinical and cost-effective care. When developing the quality standards, it is important to focus on clinical effectiveness, patient experience and patient safety. The long term aim is to develop a library of around 150 quality standards so that all clinical teams can have access to a quality standard relevant to their specialty.")
4
Quality Standards – the evidence base
NICE Quality Standards Based on evidence of best practice and an assessment of current care NICE Quality Standards Guidance and related products Research and audit evidence Summarised evidence- based material: accredited guidance Primary research evidence is synthesised into other products – guidance, audit and service models

5
Standards and high quality care
There is no statutory provision allowing NICE Quality Standards to impact upon registration requirements Quality Standards are advice from NICE to the NHS CB on high quality care. Regulation ( Enforcement against Registration Requirements) Development of commissioning guidance (NHS CB) Commissioning Outcomes Framework Provider Payment Mechanisms Registration requirements Proportion of services NICE quality standards Standard of services Unsafe Substandard Adequate Good Excellent
 Development of commissioning guidance (NHS CB) Commissioning Outcomes Framework. Provider Payment Mechanisms. Registration requirements. Proportion of services. NICE quality standards. Standard of services. Unsafe. Substandard. Adequate. Good. Excellent.")
6
Development of Quality Standards
Topic referral from National Quality Board / Department of Health Topic Expert Group Recruitment Topic Scoping Review of Clinical Guidelines and development of preliminary prioritisation of recommendations with TEG Chair First TEG Meeting: Wording of draft statements and measures agreed Consultation of draft quality standard Second TEG Meeting: Agreement of final quality standard NICE sign off process Co-badging This is a brief summary of the various stages in the quality standards development process. Topics are referred to NICE by the National Quality Board and the Department of Health. At the scoping meeting, the TEG identify the evidence sources to be used and the areas of the care pathway to be addressed. A ‘long’ list of recommendations is then extracted from the relevant guidance and recommendations are prioritised based on the areas highlighted by the TEG. Key Priorities for Implementation from the applicable clinical guideline will normally be prioritised however KPIs may not be measurable and so may not be suitable for development into a quality statement. Also, the KPIs may not cover all the areas of care which need to be included in the quality standard. As a result, this ‘long’ list may include other recommendations based on suggestions made by the TEG, its chair, and the consultant clinical adviser for the Quality Standards team. However, the standards aren’t just based on NICE guidance and there can be quality standards with no relevant NICE guidance. Other relevant policy drivers and audit evidence are disseminated down into the quality standard. They are developed from the whole evidence base. This collated evidence is used by the Topic expert groups to draft statements and measures which are then consulted upon for 4 weeks. The comments received go to the topic expert group at their final meeting and, if necessary, the standard is changed. Topic expert groups are made up of: some of the NICE quality standards team and information specialists topic experts (e.g. from guidance development groups and national collaborating centres) patients and lay people commissioners service providers The quality standard is then published on the NICE website. Publication partners are secured to jointly badge the standard and maximise dissemination. Timing: 12 months following commencement, depending on extent and nature of evidence sources and field testing/consultation
 patients and lay people. commissioners. service providers. The quality standard is then published on the NICE website. Publication partners are secured to jointly badge the standard and maximise dissemination. Timing: 12 months following commencement, depending on extent and nature of evidence sources and field testing/consultation.")
7
Current Work Programme
Stroke COPD Dementia CKD VTE – Prevention Diabetes Specialist Neonatal Care Depression End of Life Care Glaucoma Chronic Heart Failure Breast Cancer Alcohol Dependence Patient Experience The table above shows the QS topics published and currently being developed by NICE.

8
Topics in development Consultation shortly on the ‘Library’ of topics
Acute chest pain Antenatal care Asthma Bipolar disorder in adults Bipolar disorder in children and adolescents Colorectal cancer Diabetes in children Diagnosis and management of hepatitis B Drug use disorders (over-16s) Epilepsy in adults Epilepsy in children Falls in a care setting Head injury Hip fractures Intrapartum care Intravenous fluid therapy in hospitalised adult patients Lung cancer Management of myocardial infarction Management of ulcerative colitis Meningitis in people under 16 Migraine/headache Nutrition in hospital Osteoarthritis Ovarian cancer Postnatal care Pressure ulcers Prostate cancer Pulmonary embolism Reflux disease (gastro- oesophageal reflux disease) Safe prescribing Schizophrenia Consultation shortly on the ‘Library’ of topics
 Epilepsy in adults. Epilepsy in children. Falls in a care setting. Head injury. Hip fractures. Intrapartum care. Intravenous fluid therapy in hospitalised adult patients. Lung cancer. Management of myocardial infarction. Management of ulcerative colitis. Meningitis in people under 16. Migraine/headache. Nutrition in hospital. Osteoarthritis. Ovarian cancer. Postnatal care. Pressure ulcers. Prostate cancer. Pulmonary embolism. Reflux disease (gastro- oesophageal reflux disease) Safe prescribing. Schizophrenia. Consultation shortly on the ‘Library’ of topics.")
9
Social Care Standards Social care – formally added to NICE’s remit in April 2012 Pilot of 2 social care topics for standard development in 2011: Workshop with key group in July 2011 to inform the model Evidence base and underpinning ‘guidance’ is crucial Topics likely to bridge the health and social care interface

10
Example - Stroke Quality Standard
The standards are a web based resource and can be accessed through the web address above.

11
Stroke: quality statement 2
Patients with acute stroke receive brain imaging within 1 hour of arrival at the hospital if they meet any of the indications for immediate imaging. Directly based on NICE clinical guideline recommendation This is an example of one of the quality statements for stroke.

12
Related stroke process measure
Proportion of patients with acute stroke who meet any of the indications for immediate imaging who have had brain imaging within 1 hour of arrival at the hospital. [Numerator & Denominator defined] This is an example of the quality measures which accompany the statement. The structure measures ask for evidence of policies or local arrangements to show that structures are in place to allow a particular service or intervention to occur as laid down in the quality statement. The process measures ask for evidence of actual compliance with the quality statement. All process measures are specified in the form of a numerator and a denominator which define a proportion (numerator/denominator). The numerator is assumed to be a subset of the denominator population.
. The numerator is assumed to be a subset of the denominator population.")
13
Process measures for each statement
Pros Cons A direct measure of the quality of health care Not all process measures directly linked to health outcomes - IF a link has been demonstrated between a given process and outcome Can be a ‘tick box’ exercise - Been done but … - How well has something been done?? More sensitive than outcome measures to differences in quality of care Mortality / morbidity versus Use of therapeutic interventions Can therefore use at local level to assess quality of care Can be open to gaming Easy to interpret Data available?

14
Relevant data sources highlighted
Trusts can collect data via the Sentinel Stroke Audit, Hospital Episode Statistics (HES) data and through local data collection. Sentinel Stroke Audit CV02 Proportion of stroke patients given a brain scan within 24 hours of stroke DH WCC Assurance Framework Acute 36 Percentage of stroke admissions given a brain scan within 24 hours This is an example of the data source which can be used to collect evidence that the measures are being satisfied.
 data and through local data collection. Sentinel Stroke Audit CV02. Proportion of stroke patients given a brain scan within 24 hours of stroke. DH WCC Assurance Framework Acute 36. Percentage of stroke admissions given a brain scan within 24 hours. This is an example of the data source which can be used to collect evidence that the measures are being satisfied.")
15
Outcomes Framework and Standards

16
Stroke and the Outcomes Framework
DOMAIN 1 Preventing people dying prematurely DOMAIN 2 Enhancing quality of life for people with long-term conditions DOMAIN 3 Helping people recover from ill health Overarching indicators Mortality from causes amenable to healthcare Health-related quality of life Emergency readmissions within 28 days Improvement areas Under 75 mortality rate from cardiovascular disease Proportion of people feeling supported to manage their condition Employment of people with long-term conditions Unplanned hospitalisation for chronic ambulatory care sensitive conditions Heath-related quality of life for carers Improving recovery from stroke Proportion of older people still at home 91 days after discharge into rehab services

17
Encouraging use of standards
National Outcomes Framework Triggering a review of local performance against relevant national outcome indicators Local provider payment mechanisms Best practice tariff Commissioning for Quality Improvement Initiatives (CQUIN) Quality Outcomes Framework (QOF) Local commissioning mechanisms Commissioning Outcomes Framework (COF) Indicators for local use
 Quality Outcomes Framework (QOF) Local commissioning mechanisms. Commissioning Outcomes Framework (COF) Indicators for local use.")
18
Commissioning Outcomes Framework
The Commissioning Outcome Framework will be a set of indicators designed to reflect good commissioning. Indicators will be used to: allow the NHS Commissioning Board to identify the contribution of consortia to achieving priorities for health improvement enable consortia to benchmark their performance and identify priorities provide the potential for some indicators to be linked to quality premium payments

19
Summary of key NICE elements
NICE clinical guidelines, public health guidance, technology appraisal guidance and NHS Evidence accredited sources NICE quality standards – quality statements Quality measures – QOF indicators and COF indicators NICE Commissioning guidance NICE Pathways This slide shows the contribution NICE can make through the delivery of NICE products in a process flow. We propose that the quality standards provide the platform for potential COF indicators and also indicators for other purposes such as QOF, commissioning guidance. This will help ensure that the guidance and incentives in the new system are properly integrated. We support the vision that COF indicators measure the contribution to good health outcomes that can be achieved by GP-led commissioning. However, we believe that this can only credibly be done by measuring health care processes that can be directly influenced through the commissioning process and which have a clear, evidence-based link to health outcomes. These healthcare processes will reflect care provided in primary, secondary and community care settings. When attempting to assess how well commissioning activities carried out by GPs lead to improvements in outcomes, issues such as attribution, data quality, case mix and population size (for meaningful denominators), will present challenges which will need to be addressed. We propose that indicators developed to assess the outcomes achieved by GP commissioning consortia, should be evidence-based, consider clinical and cost effectiveness and be developed from NICE guidance and NHS Evidence accredited sources.
, will present challenges which will need to be addressed. We propose that indicators developed to assess the outcomes achieved by GP commissioning consortia, should be evidence-based, consider clinical and cost effectiveness and be developed from NICE guidance and NHS Evidence accredited sources.")
20
We’ve published a lot of guidance!
Products Numbers Cancer service guidance 10 Clinical guidelines 122 Interventional procedures 341 Technology appraisals 222 Medical technologies 3 Public health 34 Safety solutions 2 Total 734 Excludes superseded guidance

21
And so…. NICE pathways To bring together related guidance, between and within topics To link other products – Quality Standards, audit tools etc To provide a useful format for commissioners To improve digital formatting for easier access Easier, quicker access to the evidence

22
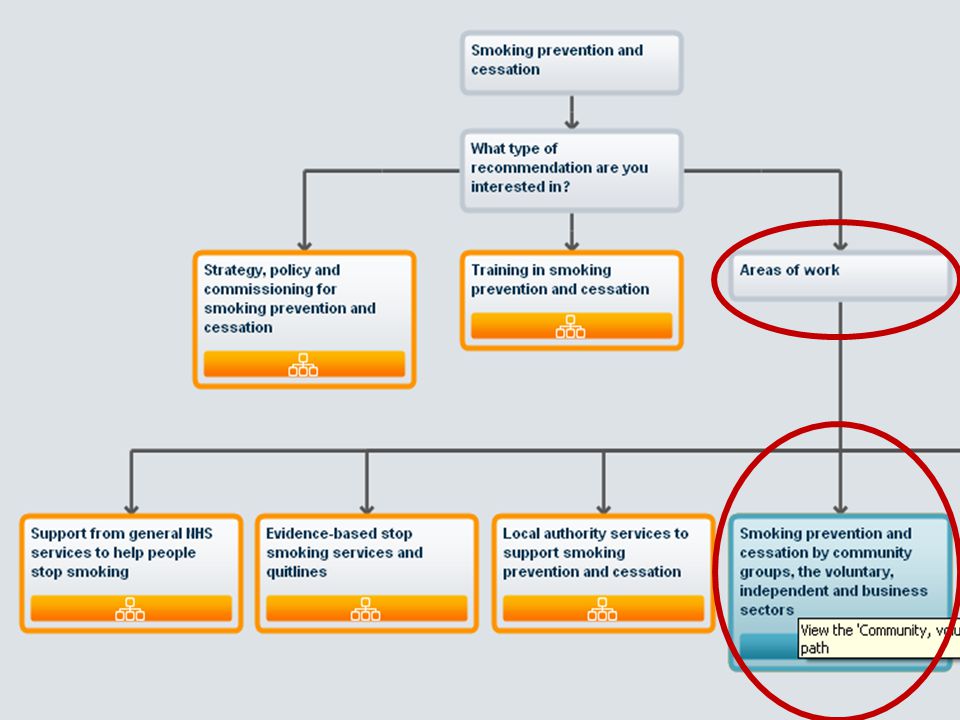
How the Pathways work

24
Information nodes

25
Detailed advice appears on the right

26
Links to other information
Easy access to other supportive information from the toolbar at the top of the screen – including implementation support and commissioning advice Links to quality standards and statements where these exist Future developments will facilitate access to indicators and data collection systems

27
Access via the NICE website

28
…and NHS Evidence

29
Rolling out Pathways 18 topics now launched, based on Quality Standard areas, including: VTE prevention Dementia Stroke Depression Exercise Alcohol Smoking Target for 2011/12 is to produce 60 new NICE Pathways Topics will be prioritised based on: publication of Standards new/updated guidance those cross referenced the most, such as maternity

30
Key messages Quality Standards represent key elements of best practice to drive up quality Meeting Quality Standards will help improve national outcomes and inform local practice and data collection NICE pathways facilitate access to standards and underpinning guidance NHS Evidence provides access to guidance, Standards, support tools and a range of other evidence-based information to inform local decision-making

31
What does this mean for NHS Evidence?
NHS Evidence is a health and social care information service providing access to evidence-based information to deliver high quality care. It aims to: - provide BREADTH of information to all users of NHS Evidence - provide easy OPEN ACCESS to information - maintain the QUALITY of information available to users Feedback Over half a million unique visitors to NHS Evidence each month 1.2 million searches performed each month More than 90% of users believe the information they access through NHS Evidence is robust

32
Search results plus information panels
TOPIC PAGE – clinical The topic page panels, again based on extensive user research, represent a showcase for content that NICE owns and the key sources and types of evidence which NHS Evidence wants to highlight. Each topic page introduction draws from CKS (to be replaced) This improves the consistency in presentation of content across different topics and will hopefully save time for the user who wants to get to the best value evidence-based content that exists for the topic. A feature3 of the new topic panel presentation is the accordion panels – each containing core resources under key areas of interest under a topic such as commissioning etc The search results and filters are also provided for users who want to drill further down.
 This improves the consistency in presentation of content across different topics and will hopefully save time for the user who wants to get to the best value evidence-based content that exists for the topic. A feature3 of the new topic panel presentation is the accordion panels – each containing core resources under key areas of interest under a topic such as commissioning etc. The search results and filters are also provided for users who want to drill further down.")
Similar presentations