Download presentation
Presentation is loading. Please wait.

1
LYMPHOMA

2
*Def: malignant tumor of the lymphoid system. *Sites:
I. Lymphoid tissues: a. Nodal: from lymph nodes. b. Extra nodal: spleen, bone marrow, liver and lymphoid collections (tonsils, adenoids, payer’s patches and solitary lymphoid follicle of the large intestine). II.Non-lymphoid tissues: as skin, CNS, kidneys & testis. *Classification: I. Hodgkin’s lymphoma. II. Non-Hodgkin’s lymphoma.
. II.Non-lymphoid tissues: as skin, CNS, kidneys & testis. *Classification: I. Hodgkin’s lymphoma. II. Non-Hodgkin’s lymphoma.")
3
HODGKIN’S LYMPHOMA *Incidence: common
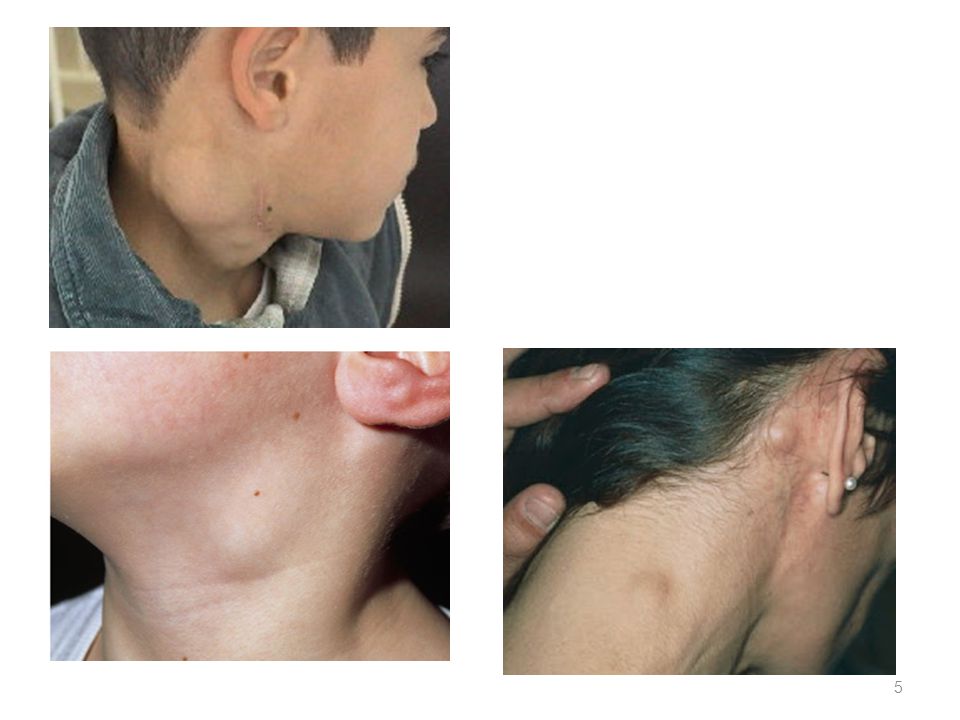
*Age: 2 peaks: in young adults & in middle age. *Pathology: -Starts nodal (in axial L.Ns as cervical, mediastinal and para aortic) and then involve the extra nodal tissues and less commonly involve the non-lymphoid tissues.
 and then involve the extra nodal tissues and less commonly involve the non-lymphoid tissues.")
4
I. Lymph Nodes: * N/E: Enlarged, firm, discrete. C/S: hemorrhage & necrosis. * M/P: Loss of the nodal architecture and replacement by two component;, neoplastic component & inflammatory background.

6
A. Neoplastic component: (Reed-Sternberg giant cell (RSC)):
Giant cells contain multiple nuclei in the center. Surrounded by clear halo. The cytoplasm is abundant & esinophilic. The nuclei are arranged in pairs with mirror image appearance. The nuclei are vesicular with thick irregular nuclear mm. The nuclei show prominent esinophilic nucleoli surrounded by clear halo giving Owl eye look. B. Reactive inflammatory background: Formed of lymphocytes, plasma cells, macrophages, eosinophils & neutrophils with fibrosis.

9
II. Extra nodal involvement:
Splenomegally in 75%. Hepatomegally in 50%. Bone marrow in 15%. III. Extra lymphoid organ involvement: Less common.

10
* Classification of Hodgkin’s lymphoma:
A. Classic Hodgkin’s lymphoma: Nodular sclerosis type. Mixed cellularity type. Lymphocytic predominance type. Lymphocytic depleted type. B. Nodular lymphocytic predominance Hodgkin's lymphoma (NLPHL).
.")
11
* Systemic manifestation of Hodgkin’s lymphoma: Includes:
Pel-Ebestein fever. Anemia. Leucocytosis. Eosinophilia. Pruritis. Depressed T-cell function. The patient is classified A (absent manifestation) or B (present manifestation). When present indicates bad prognosis.
 or B (present manifestation). When present indicates bad prognosis.")
12
* Staging of lymphoma: Stage I: involvement of a single L.N region.
Stage II: involvement of two or more L.N regions on the same side of the diaphragm. Stage III: multiple sites above and below the diaphragm. Stage IV: involvement of extra lymphatic organs + or – L.N involvement.

14
NON HODGKIN’S LYMPHOMA (NHL)
*Incidence: less common than Hodgkin’s lymphoma. *Age: any age. *Pathology: The disease may be localized or disseminated from the start. Extra-nodal & Non-lymphoid tissue involvement is common and may be the first presentation.

15
Lymph nodes show: N/E: M/P: Enlarged, soft, fused.
C/S: hemorrhage & necrosis. M/P: Loss of normal nodal architecture & replacement by single cell type of transformed lymphocytes.

16
Lymph nodes; NHL

17
NHL

18
NHL

19
*Types of NHL: B. Cell lymphomas Precursor B. cell lymphoma:
Lymphoblastic leukemia/Iymphoma B. Peripheral B. Cell lymphoma: Chronic Iymphocytic leukemia/small Iymphocytic Iymphoma. Diffuse large B. cell lymphoma. Lymphoplasmacytic lymphoma Mantle cell Iymphoma. Follicular Iymphoma Marginal Zone Lymphoma. Burkitt Iymphoma

20
B-cell lymphomas constitute the vast majority of lymphomas, accounting for nearly 90% of all lymphomas. Immunosuppression, specifically due to HIV infection and immunosuppressive therapy, is associated with a markedly increased incidence of developing mature B-cell lymphomas, particularly diffuse large B-cell lymphoma and Burkitt's lymphoma.

21
Diffuse large B-cell lymphoma and follicular lymphoma are the most common types.
Follicular lymphoma, chronic lymphocytic leukemia/small lymphocytic lymphoma, marginal zone B-cell lymphoma and lymphoplasmacytic lymphoma, which are generally indolent lymphoma, but incurable and usually present in a disseminated stage with bone marrow involvement.

22
Mantle cell lymphoma and diffuse large B-cell lymphoma represent “intermediate-grade B-cell lymphomas” that generally show a more aggressive clinical behavior, but are potentially curable. Burkitt's lymphoma and precursor B-lymphoblastic leukemia/lymphoma are high-grade B-cell lymphomas.

23
T. CELL and NK cell lymphomas
Precursor T cell lymphoma: - Lymphoblastic leukemia/lymphoma. B. Peripheral T-cell and NK cells lymphomas: Aggressive NK cell leukemia Mycosis fungoides and sezary syndrome . Angio-immunoblastic T-cell Iymphoma. Adult T-cell leukemia/lymphoma (HTLV1+). anaplastic large cell Iymphoma (ALCL). Peripheral T. cell lymphoma, unspecified.
. anaplastic large cell Iymphoma (ALCL). Peripheral T. cell lymphoma, unspecified.")
24
Mature T. cell and natural killer (NK) cell lymphomas are rare, accounting for only 10% of all Non-Hodgkin lymphoma, and usually are more aggressive than B-cell lymphomas. The most common subtypes are peripheral T-cell lymphoma, unspecified and anaplastic large cell lymphoma.

Similar presentations







>")




>")









>")