Download presentation
Presentation is loading. Please wait.

1
Diabetic Foot Infection: A challenge for primary and secondary care? Dr Tony Berendt Consultant Physician Bone Infection Unit NOC NHS Trust, Oxford

2
Disclosure of Potential Conflicts of Interest Has received honoraria, travel expenses and hospitality for serving on speakers bureaux and advisory boards for RPR (Synercid), Pfizer (Linezolid) MSD (Ertapenem) and MacroChem (Pexiganin) Vice-Chair of IDSA Clinical Practice Guidelines Committee for Diabetic Foot Infections; Chair of IWGDF Osteomyelitis Sub-group Member of Oxfordshire Priorities Forum and ORH- NOC Medicines Advisory Committee DIPC at NOC, Chair of TV (South Central) CHAIN and Steering Group for pan-Oxfordshire C. difficile intervention project

3
Infection and Healing Wound Healing Lose footwear Off- loading Infection Replace footwear Amputation

4
Learning objectives Be able to discuss the epidemiological importance of DFI Know how to assess risk of diabetic foot ulceration and infection Be able to assess a patient with a diabetic foot infection, in the context of published guidelines, and make rational antibiotic choices Epidemiology Pathophysiology Microbiology Assessment Biomechanics

5
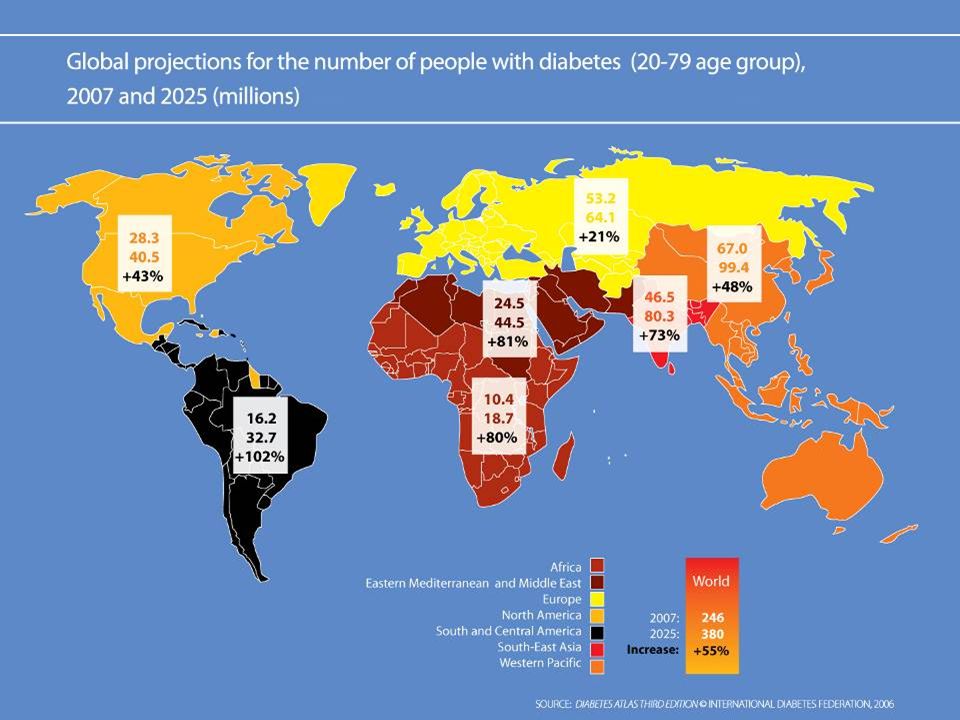
General epidemiology 252 million diabetics worldwide Epidemiology Pathophysiology Microbiology Assessment Biomechanics

7
General epidemiology 252 million diabetics worldwide Foot problems account for largest number of hospital bed days used for diabetic patients 1-4% of diabetics develop foot ulcer annually, 25% in lifetime 45-75% of all lower extremity amputations are in diabetics 85% of these preceded by foot ulcer Two-thirds of elderly patients undergoing amputation do not return to independent life Studies have shown less costs for saving a limb cf. amputation Epidemiology Pathophysiology Microbiology Assessment Biomechanics

8
Pathophysiology: diabetic foot ulceration Neuropathy

10
Pathophysiology: diabetic foot ulceration Neuropathy Sensory Loss of protective sensation Motor Abnormal foot biomechanics Autonomic Reduced skin compliance and lubrication Ulceration Infection Vascular insufficiency

11
30-second foot examination Any previous diabetes related foot problems? Are both foot pulses palpable? Is protective sensation intact? Is there evidence of significant foot deformity?

13
Two-minute foot examination Examine feet for ulcers, callus, blisters, maceration, skin breaks, infection Examine the toenails Identify nature of any foot deformity Examine the shoes Observe patient’s ability to perform foot care and examination (by observing them replace socks and shoes) Establish need for patient education
 Establish need for patient education")
14
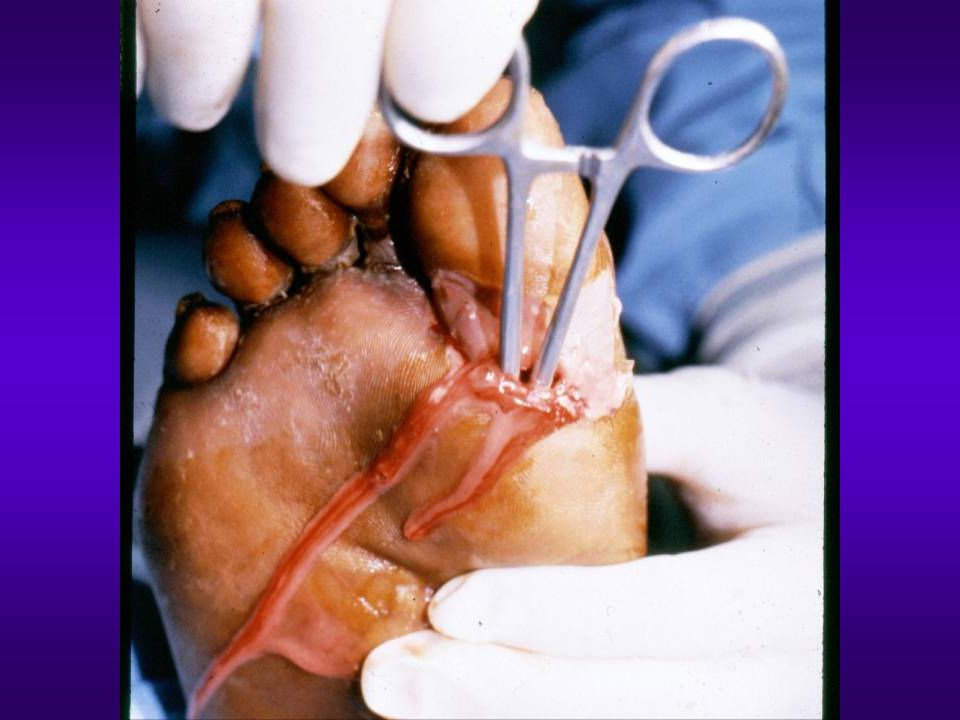
Standard ulcer care Evaluate for infection Debride ulcer, remove callosities Check for sensation (monofilament) Check for circulation (pulses, Dopplers) Probe to bone? Adequate offloading Antibiotics if infected Secondary prevention of ulcer and of major diabetes related events Epidemiology Pathophysiology Microbiology Assessment Biomechanics

15
Overview of Diabetic Foot Infections Slide courtesy of Ben Lipsky, Puget Sound VA, Seattle

16
Independent Risk Factors* for Foot Infection : Diabetex Prospective Trial Variable Risk Ratio (95%CI) p Value Wound depth to bone 6.7 (2.3–19.9) 0.001 Wound duration >30 days 4.7 (1.6–13.4) 0.004 Recurrent foot wound 2.4 (1.3–4.5) 0.006 Traumatic wound etiology 2.4 (1.1–5.0) 0.02 Peripheral vascular disease 1.9 (1.0–3.6) 0.04 Lavery, Armstrong, Lipsky et al, Diabetes Care 2006;29:1288 *stepwise logistic regression model, excluding ulceration
 p Value Wound depth to bone 6.7 (2.3–19.9) Wound duration >30 days 4.7 (1.6–13.4) Recurrent foot wound 2.4 (1.3–4.5) Traumatic wound etiology 2.4 (1.1–5.0) 0.02 Peripheral vascular disease 1.9 (1.0–3.6) 0.04 Lavery, Armstrong, Lipsky et al, Diabetes Care 2006;29:1288 *stepwise logistic regression model, excluding ulceration")
17
Microbiology Popular mythology = all infections are polymicrobial Epidemiology Pathophysiology Microbiology Assessment Biomechanics

18
Gram positive cocci Microbial complexity Microbial burden Clinical risk 1 234 Anaerobes Aerobic Gram-negative rods Prior Rx NecrosisDepthSeverity

19
Treatment: myths Treat uninfected ulcers to promote healing Treat infected ulcers until the ulcer is healed Treat all the organisms isolated from the microbiological specimens Hospitalise all infections Give lots of intravenous therapy

20
Timeline of Staphylococcal antibiotic resistance 19401950196019701980199020002010 Penicillin-resistance GISACA-MRSAVRSASporadic MRSA Epidemic MRSA

22
www.idsociety.orgwww.idsociety.org Clinical Infectious Diseases 2004;39:885-910 www.idsociety.org

24
Evaluating the Patient with a DFI PatientPatient –Systemic response Fever, chills, sweats, cardiovascular status –Metabolic status Hyperglycaemia, electrolyte imbalance, hyperosmolality, renal impairment –Cognitive function Delirium, depression, dementia, psychosis –Social situation Support, self-neglect · Limb/Foot · Wound Epidemiology Pathophysiology Microbiology Assessment Biomechanics

25
Evaluating the Patient with a DFI PatientPatient Limb or Foot –Biomechanics –Vascular Ischaemia Venous insufficiency –Neuropathy –Infection Wound –Size, depth –Necrosis, gangrene –Infection Epidemiology Pathophysiology Microbiology Assessment Biomechanics

27
Clinical Classification of Diabetic Foot Infection Mild 2 Moderate 3 Severe 4 Wound without purulence or other evidence of inflammation More than 2 of purulence, erythema, pain, tenderness, warmth or induration. Any cellulitis/erythema extends ≤2 cm around ulcer and infection is limited to skin/superficial subcut tissues. No local complications or systemic illness Infection in patient who is systemically well & metabolically stable but has any of: cellulitis extending >2 cm; lymphangitis; spread beneath fascia; deep tissue abscess; gangrene; muscle, tendon, joint or bone involved Infection in a patient with systemic toxicity or metabolic instability Clinical Manifestations of Infection Clinical Manifestations of Infection Uninfected 1 Epidemiology Pathophysiology Microbiology Assessment Biomechanics

28
Outcomes By IDSA DFI Severity Classification Armstrong, Lavery, Peters, Lipsky. Clin Infect Dis 2007 LE Amputation X 2 trend = 108, p < 0.0001 None Mild Moderate Severe None Mild Moderate Severe Hospitalization X 2 trend = 118.6, <0.0001 None Mild Moderate Severe 1666 patients enrolled in prospective diabetic foot study

32
Table 8 Table 8: Suggested Antibiotic Regimens: DFI Advised RouteOral for MostOral or IVParenteral Dicloxacillin Yes Clindamycin Yes Cephalexin Yes TMP/SMX Yes Amoxicillin/clavulanate Yes Levofloxacin Yes Cefoxitin Yes Ceftriaxone Yes Ampicillin/sulbactam Yes Linezolid (± aztreonam) Yes Daptomycin (± aztreonam) Yes Ertapenem Yes Cefuroxime (± metronidazole) Yes Ticarcillin/clavulanate Yes Piperacillin/tazobactam Yes Levo- or Cipro- floxacin + Clindamycin Yes Imipenem-cilastatin Yes Vanco + Ceftazidime ± metronidazole Yes Agent(s)Mild Moderate Severe
 Yes Daptomycin (± aztreonam) Yes Ertapenem Yes Cefuroxime (± metronidazole) Yes Ticarcillin/clavulanate Yes Piperacillin/tazobactam Yes Levo- or Cipro- floxacin + Clindamycin Yes Imipenem-cilastatin Yes Vanco + Ceftazidime ± metronidazole Yes Agent(s)Mild Moderate Severe")
33
SiteSeverityRouteLocationDuration Soft tissue only Mild Topical or oralOutpatient7-14 days ; extend up to 28 d if slow to resolve Moderate Oral (or initial parenteral) Outpatient/ inpatient 2-4 weeks Severe Initial IV, switch to oral when possible Inpatient, to outpatient 2-4 weeks Bone or joint Extent of surgery Route Duration No residual infected tissue (e.g. post amputation) Parenteral or oral 2-5 days Residual infected soft tissue only Parenteral or oral 2-4 weeks Residual infected (but viable) bone Initial IV, then consider oral switch 4-6 weeks No surgery, or residual dead bone post-op. Initial IV, then consider oral switch >3 months
 Parenteral or oral 2-5 days Residual infected soft tissue only Parenteral or oral 2-4 weeks Residual infected (but viable) bone Initial IV, then consider oral switch 4-6 weeks No surgery, or residual dead bone post-op. Initial IV, then consider oral switch >3 months.")
35
The diabetic foot: Charcot foot with “rocker bottom” deformity

36
Charcot foot –grossly disordered architecture and biomechanics –midfoot ulceration –instability of midfoot –note previous minor amputations –still well-vascularised

37
Bone resorption and destruction

38
Bone regeneration on antibiotic therapy

39
Conclusions Ulceration is a common consequence of diabetic neuropathy To understand and treat ulceration, understand the pathophysiology and biomechanics Infection (DFI) is a common and frequently serious consequence of diabetic foot ulceration (DFU) A structured approach to assessment and treatment, using international or local guidelines, provides a means to rationalise care and improve outcomes Care must be multidisciplinary to achieve this; agreed pathways, health service management and audit are required
 is a common and frequently serious consequence of diabetic foot ulceration (DFU) A structured approach to assessment and treatment, using international or local guidelines, provides a means to rationalise care and improve outcomes Care must be multidisciplinary to achieve this; agreed pathways, health service management and audit are required")
40
Doctor treating a patient in his surgery: 17 th Century, after Teniers the younger (by kind permission of National Gallery, London) Does it need antibiotics, doctor? You must be joking mate! Debridement and offloading more like it! Besides, they won’t be discovered for another 300 years!

Similar presentations