Download presentation
Presentation is loading. Please wait.

1
Benign diseases of the vulva, vagina and cervix

2
The vulva Is the part of the female genital tract located between the genitocrural folds laterally, the mons pubis anteriorly, and the anus posteriorly. Embryologically, it is the result of the junction of the cloacal endoderm, urogenital ectoderm, and paramesonephric mesodermal layers. This hollow structure contains LABIA MAJORA LABIA MINORA CLITORIS VESTIBULE URINARY MEATUS VAGINAL ORIFICE HYMEN BARTHOLIN GLANDS SKENE DUCTS.

4
The vulva Different epithelia, from keratinized squamous epithelium to squamous mucosa, cover the vulva. The labia minora are rich with sebaceous glands but have few sweat glands and no hair follicles. The epithelium of the vestibule is neither pigmented nor keratinized and contains eccrine glands.

5
BENIGN LESIONS OF THE VULVA
According to the International Society for the Study of Vulvar Disease (ISSVD) in 1989: Inflammatory diseases. Blistering diseases. Pigmentary changes. Benign tumors, hamartomas and cysts Congenital malformations.
 in 1989: Inflammatory diseases. Blistering diseases. Pigmentary changes. Benign tumors, hamartomas and cysts. Congenital malformations.")
6
Inflammatory diseases
Lichen sclerosus Squamous cell hyperplasia (+/- atypia) Lichen simplex chronicus (localized neurodermatitis) Primary irritant dermatitis Intertrigo Allergic contact dermatitis Fixed drug eruption Erythema multiforme Toxic epidermal necrolysis Atopic dermatitis Seborrheic dermatitis Psoriasis Reiter disease Lichen planus Lupus erythematosus Darier disease Aphthosis and Behçet disease Pyoderma gangrenosum Crohn disease Hidradenitis suppurativa Fox-Fordyce disease Plasma cell vulvitis Vulvar vestibulitis syndrome
 Lichen simplex chronicus (localized neurodermatitis) Primary irritant dermatitis. Intertrigo. Allergic contact dermatitis. Fixed drug eruption. Erythema multiforme. Toxic epidermal necrolysis. Atopic dermatitis. Seborrheic dermatitis. Psoriasis. Reiter disease. Lichen planus. Lupus erythematosus. Darier disease. Aphthosis and Behçet disease. Pyoderma gangrenosum. Crohn disease. Hidradenitis suppurativa. Fox-Fordyce disease. Plasma cell vulvitis. Vulvar vestibulitis syndrome.")
7
Blistering diseases Familial benign chronic pemphigus (Hailey-Hailey disease) Bullous pemphigoid Cicatricial pemphigoid

8
Pemphigus vulgaris Erythema multiforme Epidermolysis bullosa

9
Pigmentary changes Acanthosis nigricans Lentigo Melanocytic nevus
Postinflammatory hyperpigmentation Postinflammatory hypopigmentation Vitiligo

10
Benign tumors, hamartomas, and cysts
Hidradenoma Lipoma Chronic Inflammatory swellings Hemangioma Lymphangioma Angiokeratoma Pyogenic granuloma Sebaceous gland hyperplasia Papillomatosis Bartholin cysts Epidermal inclusion cyst (Dermoid cyst) Endometriosis Hydrocele of the canal of Nuck Skene duct cyst Seborrheic keratosis Acrochordon (fibroepithelial polyp) Fibroma, fibromyoma, and dermatofibroma
 Endometriosis. Hydrocele of the canal of Nuck. Skene duct cyst. Seborrheic keratosis. Acrochordon (fibroepithelial polyp) Fibroma, fibromyoma, and dermatofibroma.")
11
BENIGN LESIONS OF THE VULVA
BARTHOLIN’s CYST ATROPHIC LICHEN (LICHEN SCLEROSUS ET ATROPHICUS) SQUAMOUS HYPERPLASIA LICHEN SIMPLEX CHRONICUS HIDRADENOMA PAPILLIFERUM
 SQUAMOUS HYPERPLASIA. LICHEN SIMPLEX CHRONICUS. HIDRADENOMA PAPILLIFERUM.")
12
Bartholin’s Cyst/Abscess
Medial to labia minor Blockage of duct following infection N. gonorrhea Staphylococci Anaerobes

14
Thomas Bartholin Danish professor In 1652 he gave the first full description of the human lymphatic system.

15
Marsupalization

16
lichen

17
What is lichen? A fungus, usually of the class Ascomycetes, that grows symbiotically with algae, resulting in a composite organism that characteristically forms a crustlike or branching growth on rocks or tree trunks.

18
In pathology…. Any of various skin diseases characterized by patchy eruptions of small, firm papules.

19
Lichen Sclerosus et Atrophicus
Most patients are post-menopausal women Stenosis of the introitus develops

20
Lichen Sclerosus et Atrophicus
Note the white, parchment-like or plaque-like lesion

21
Lichen Sclerosus et Atrophicus
During early stages the patient may not have symptoms. Some patients develop intractable pruritus Burning and pain are less likely manifestations. Figure-of-8 or keyhole configuration. In late stages normal architecture may be lost atrophy of the labia minora, constriction of the vaginal orifice (kraurosis), synechiae, ecchymoses, fissures. Squamous cell carcinoma develops in 3-6% cases
, synechiae, ecchymoses, fissures. Squamous cell carcinoma develops in 3-6% cases.")
22
Lichen Sclerosus et Atrophicus
Thinning of the surface epithelium with some hyperkeratosis.

23
Lichen Sclerosus et Atrophicus
Etiology Unknown. A higher prevalence of the disease in postmenopausal women suggests hormonal factors, but this has not been confirmed. Studies identifying an infection are inconclusive Weakly linked to autoimmune diseases and genetic factors Local factors (eg, trauma, friction, chronic infection and irritation) Recurrence near vulvectomy scars has been observed.
 Recurrence near vulvectomy scars has been observed.")
24
Lichen Sclerosus et Atrophicus
Treatment Potent topical corticosteroids Testosterone propionate is ineffective and has many adverse effects Close follow-up -----epithelial cancer.

25
Squamous Hyperplasia Associated with a response to hormonal influences or exposure to exogenous irritants Precursor of squamous cell CA if cells are atypical

26
Squamous Hyperplasia This lesion produces hyperplastic thickening of the superficial squamous epithelium. This lesion is a precursor of squamous cell carcinoma of the vulva

27
Squamous Hyperplasia Note the keratin horn cysts and the infiltrate of inflammatory cells at the base of the lesion.

28
Squamous Hyperplasia ITCHING is a common symptom.
If hyperkeratosis is not prominent, lesions may appear as reddish plaques. The clitoris, labia minora, and inner aspects of the labia majora are more commonly affected. Extensive lesions may result in stenosis of the vaginal introitus.

29
itch-scratch-itch cycle.
Squamous Hyperplasia Etiology Repetitive scratching or rubbing from irritants Treatment is aimed at halting the itch-scratch-itch cycle.

30
Squamous Hyperplasia Treatment The same as lichen sclerosus
General attention to proper hygiene. If the skin is moist or macerated, aluminum acetate 5% solution applied 3-4 times daily for minutes is beneficial. Systemic antihistamines or tricyclic antidepressants Refractory lesions, intralesional injections of triamcinolone acetonide may be an alternative.

31
lichen simplex chronicus
Hyperkeratotic, usually ill-defined, grayish, thickened, and sometimes excoriated lesion. Usually located over the labia majora. Hyperpigmentation. Itching is always present and may be intense.

32
lichen simplex chronicus
Lichen simplex chronicus of the vulva is the end stage of the itch-scratch-itch cycle. The initial stimulus to itch may be: Underlying seborrheic dermatitis. Intertrigo Tinea. Psoriasis. In most cases, the underlying cause is not evident and may have been transient vulvitis or vaginal discharge. Any itching disease of the vulva may become secondarily lichenified.

33
lichen simplex chronicus
Epidermal and epithelial hyperplasia, Hyperkeratosis. Fibrotic vertical streaks of collagen between the hyperplastic rete are present.

34
lichen simplex chronicus
Treatment Includes removal of irritants and/or allergens Topical application of mild-to-high–potency corticosteroids. Avoid soaps and cleansing agents other than aqueous cream. Discourage excessive cleaning of the genital area; use of hot water; overheating; and wearing of synthetic, rough, and/or tight clothing. Lichen simplex chronicus may be associated with underlying diseases (eg, Paget disease, Bowen disease)
")
35
Lichen planus Three types:
Papulosquamous Erosive Hypertrophic Malignancy is possible in long-standing and ulcerative lichen planus.

36
Lichen planus The papulosquamous form:
Occurring as part of a generalized disease Is the most common and is characterized by: Flat-topped Polyhedral, Violaceous, shiny, and itchy papules located on keratinized skin of the labia and mons pubis. Delicate and whitish reticulated papules may be present on the mucosa, but no atrophy or scarring is observed.

37
Lichen planus The erosive form:
Involves the mucous membranes of the mouth and vulvovaginal area and may be locally destructive, leading to atrophy and scarring. Synonyms include erosive vaginal lichen planus, desquamative inflammatory vaginitis, vulvovaginal-gingival syndrome, and ulcerative lichen planus. Itching is rare, but pain, burning, and irritation occur and may be responsible for dyspareunia and dysuria.

38
Lichen planus The rare hypertrophic form:
Resembling lichen sclerosus, manifests with extensive white scarring of the periclitoral area with variable degrees of hyperkeratosis. It may be very itchy. Extensive vaginal involvement may result in a malodorous discharge. Large denuded areas may become adherent, causing stenosis of the vaginal introitus and dyspareunia. Marked atrophy may develop with time.

39
ID/CC. A 75 year old woman visits her gynecologist
ID/CC A 75 year old woman visits her gynecologist for a routine checkup and is found to have white spots on her genitalia HPI She complains of slight outer vaginal itching but denies any postmenopausal bleeding, vaginal discharge, or drug intake PE Hypochromic macules on labia majora extending to perineum and inner thighs in patchy distribution with scale formation; skin is thickened

40
Pruritus vulva Causes: General Examination Local examination: General
Psychosomatic Idiopathic General Examination Local examination: Smears Culture and sensitivity BIOPSY: KEYE’s Dermatological knife

41
BENIGN LESIONS OF THE Vagina
CYSTIC SWELLINGS SOLID TUMORS ATROPHIC VAGINITIS VAGINAL ADENOSIS

42
Cystic swellings Gartner’s Cyst Epithelial inclusion cysts
Dilatation of the Gartner’s (Wollfian) duct Anterior and lateral vaginal walls Epithelial inclusion cysts Endometrioma Uretheral diverticulum
 duct. Anterior and lateral vaginal walls. Epithelial inclusion cysts. Endometrioma. Uretheral diverticulum.")
43
Solid Tumors Fibromyoma Condyloma accuminata Bilharzial polyps

44
Atrophic vaginitis Thinning and atrophy of vaginal epithelium
Most common in postmenopausal women with low estrogen levels Dyspareunia and vaginal spotting (differential includes uterine cancer)
")
45
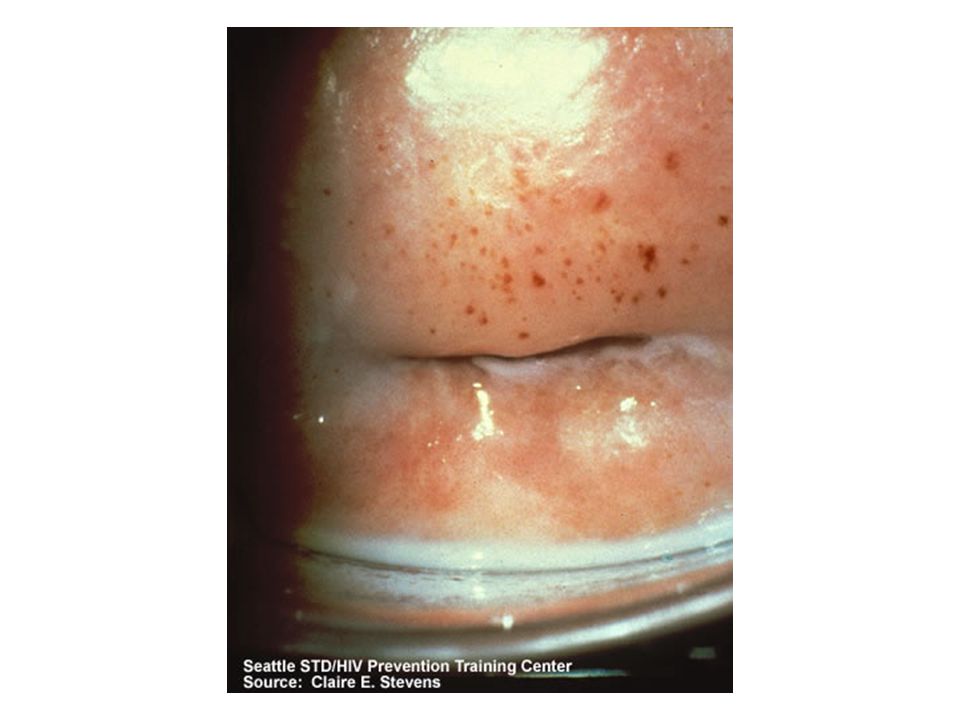
Vaginal Adenosis Persistent Mullerian columnar epithelium in the anterior wall and upper 1/3 of vagina Manifestation of maternal DES exposure Red, granular patches Precursor of clear cell adenocarcinoma

46
Vaginal Adenosis Note the red granular patches on the vaginal mucosa on the left. The slide on the right shows glandular development. Most patients are 7-35 years of age

47
BENIGN LESIONS OF THE cervix
CERVICITIS EROSION POLYPS

48
Inflammatory Lesions of the Cervix
Cervicitis (acute) Symptoms: backache, bearing-down feeling in the pelvis, dull pain in the lower part of the abdomen, urinary tract symptoms
 Symptoms: backache, bearing-down feeling in the pelvis, dull pain in the lower part of the abdomen, urinary tract symptoms.")
51
Erosion of the Cervix Characterized by columnar epithelium replacing squamous epithelium, grossly resulting in an erythematous area Causes: Physiological: Cervicitis: Acute or Chronic Hormonal therapy

53
Erosion of the Cervix Erosion of the cervix following delivery. A normal cervix is on the left

54
SMEAR Erosion of the Cervix If infection---- Treat cause
IF CIN Manage according to stage

55
Chronic Cervicitis Chronic inflammation, sometimes ulceration with repair, atypia or dysplasia, nabothian cysts from endocervical glands Backache is a common symptom

56
Chronic Cervicitis Nabothian Cysts
Endocervical glands blocked by inflammation or scarring.

57
Chronic Cervicitis Chronic inflammation underlies an area of cervical dysplasia

58
Endocervical Polyps Postcoital bleeding and irregular vaginal spotting
Inflammatory proliferations of cervical mucosa; not true neoplasms Soft; may protrude through the cervical os

Similar presentations









- Organs mature, pubic and armpit hair, regulates release of.>")


 Pathogenesis` (Mechanisms:inflammation) Clinical Features (Signs and Symptoms) Fever,>")





 2. Perception(in.>")




