Download presentation
Presentation is loading. Please wait.

1
How Marginal can the Marginal Donor Be? J H DARK Freeman Hospital University of Newcastle

2
NUMBER OF LUNG TRANSPLANTS REPORTED BY YEAR AND PROCEDURE TYPE ISHLT NOTE: This figure includes only the lung transplants that are reported to the ISHLT Transplant Registry. As such, this should not be construed as representing changes in the number of lung transplants performed worldwide. 2009

4
Number of solid organ donors and lung transplantations- UK UK Transplant

5
Up to 40% of donors yielding lungs for transplant in some parts of the World

6
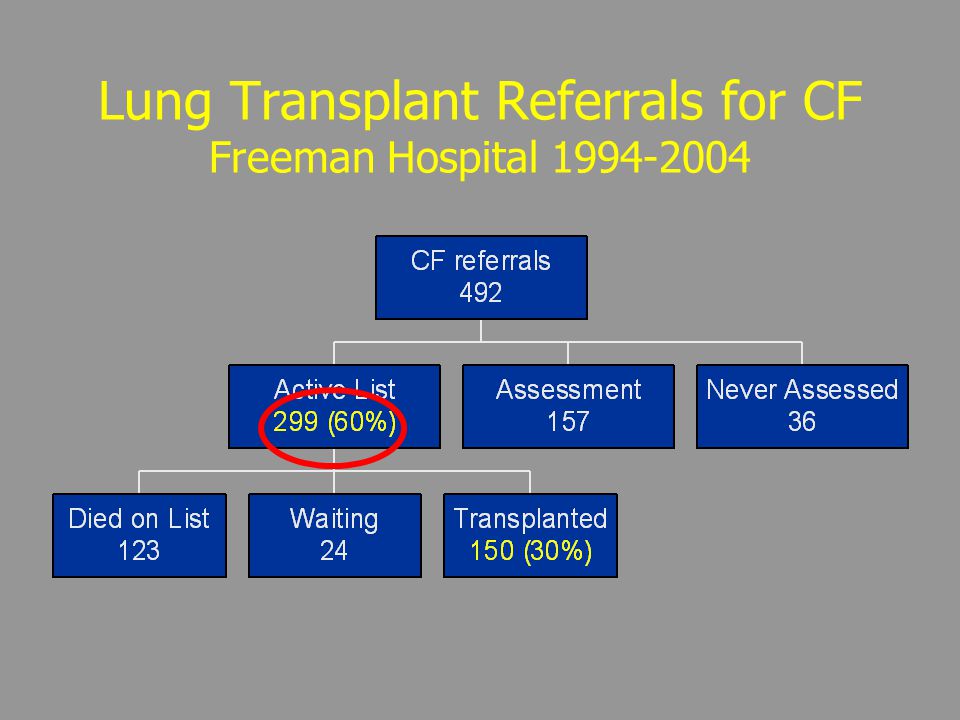
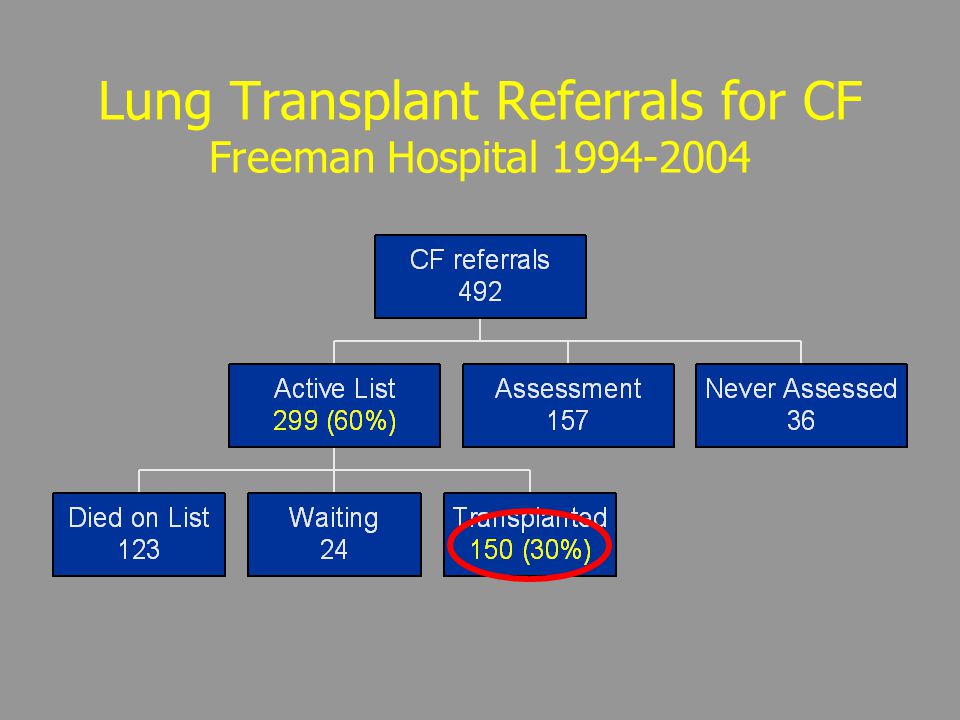
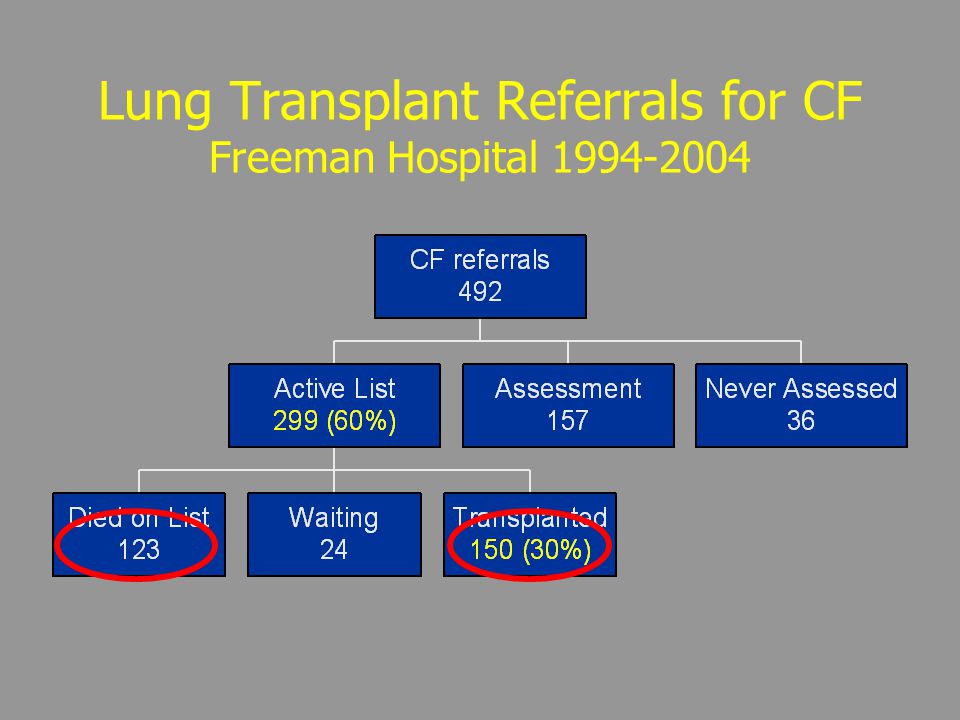
Lung Transplant Referrals for CF Freeman Hospital 1994-2004

10
Lung Transplantation for Cystic Fibrosis Actual Survival

12
Marginal Donors Landmarks Classical Criteria Harjula et al JTCVS 1987; 94:874-880

13
Ideal lung donor selection criteria Age < 55 yr ABO compatibility Clear chest radiograph PaO 2 (FiO 2 100 % + 5 cm H 2 O PEEP) > 40 kPa (PaO 2 /FiO 2 ) Smoking < 20 pack-years Absence of chest trauma Lack of previous cardiopulmonary surgery Absence of organisms on sputum Gram stain Absence of purulent bronchoscopic secretions Aggressive management of lung donors classified as unacceptable: Excellent recipient survival one year after transplantation Straznicka, M et al., JTCVS August 2002, Volume 124, Number 2 250-258
 > 40 kPa (PaO 2 /FiO 2 ) Smoking < 20 pack-years Absence of chest trauma Lack of previous cardiopulmonary surgery Absence of organisms on sputum Gram stain Absence of purulent bronchoscopic secretions Aggressive management of lung donors classified as unacceptable: Excellent recipient survival one year after transplantation Straznicka, M et al., JTCVS August 2002, Volume 124, Number")
14
Marginal Donors Landmarks Classical Criteria Sudaresan et al “Successful outcome of lung transplantation is not compromised by the use of marginal donor lungs” JTCVS, 1995; 109:1075-79

15
Marginal Donors Landmarks Classical Criteria Sudaresan et al “Successful outcome of lung transplantation is not compromised by the use of marginal donor lungs” JTCVS, 1995; 109:1075-79 Orens et al “A review of lung transplant donor acceptability criteria” JHLT 2003; 22:1183-1200

16
TABLE IISUMMARY OF LITERATURE FOR THE USE OF OLDER LUNG DONORS nDesign Outcome Novick et al (1999) 284/5,052RetrospectiveDecreased survival Meyer et al (2000) 23/1,800RetrospectiveNo adverse affect on intermediate survival Bhorade et al (2000) 9/52RetrospectiveNo adverse affect on ventilator time, hospital stay or hospital survival Hosenpud et al (2001) 15,465RetrospectiveRisk factor for 1- and 5-year mortality. Adapted from Orens et al, JHLT 2003;22:1183-1200

17
TABLE III SUMMARY OF LITERATURE FOR DONOR BLOOD GASES (PaO2/F1O2 <300) n Study Design Outcome Harjula et al (1987) 1 Case report Primary graft failure Shumway et al (1994) 25 (1) Case series No adverse affect Sandaresan et al (1995) 6 Retrospective review No adverse affect Adapted from Orens et al, JHLT 2003;22:1183-1200
 n Study Design Outcome Harjula et al (1987) 1 Case report Primary graft failure Shumway et al (1994) 25 (1) Case series No adverse affect Sandaresan et al (1995) 6 Retrospective review No adverse affect Adapted from Orens et al, JHLT 2003;22:")
18
TABLE IV SUMMARY OF LITERATURE FOR ABNORMAL DONOR CHEST X-RAY Reference nDesign Outcome (survival) Gabbay et al (1999) 39/64 Retrospective review No adverse affect Sundaresan et al (1995) 39/44 Retrospective review No adverse affect Bhorade et al (2000) 5/52 Retrospective review No adverse affect Adapted from Orens et al, JHLT 2003;22:1183-1200
 Gabbay et al (1999) 39/64 Retrospective review No adverse affect Sundaresan et al (1995) 39/44 Retrospective review No adverse affect Bhorade et al (2000) 5/52 Retrospective review No adverse affect Adapted from Orens et al, JHLT 2003;22:")
19
TABLE V SUMMARY OF LITERATURE FOR DONOR LUNG ISCHEMIC TIME (ISCHEMIC TIME >5 TO 6 HOURS) Reference nDesign Outcome (survival) Snell et al (1996) 63/106 Retrospective review Reduced long term Novick et al (1999) 5,052 Retrospective review No adverse affect of registry data except when older donor age Gammie et al (1999) 60/392 Retrospective review No adverse affect Fiser et al (2001) 15/136 Retrospective review No adverse affect Kshettry et al (1996) 8/83 Retrospective review No adverse affect Adapted from Orens et al, JHLT 2003;22:1183-1200
 Reference nDesign Outcome (survival) Snell et al (1996) 63/106 Retrospective review Reduced long term Novick et al (1999) 5,052 Retrospective review No adverse affect of registry data except when older donor age Gammie et al (1999) 60/392 Retrospective review No adverse affect Fiser et al (2001) 15/136 Retrospective review No adverse affect Kshettry et al (1996) 8/83 Retrospective review No adverse affect Adapted from Orens et al, JHLT 2003;22:")
20
TABLE VII SUMMARY OF LITERATURE FOR DONOR SMOKING HISTORY Reference nDesign Outcome (survival) Gabbay et al (1999) 5/64 Retrospective review No adverse affect Sundaresan et al (1995) 9/44 Retrospective review No adverse affect Bhorade et al (2000) 15/52 Retrospective review No adverse affect (average 36 pack- years) No differences in short-term outcome with regard to post-operative ventilation or oxygenation, nor long-term survival to 2.5 to 3 years. Adapted from Orens et al, JHLT 2003;22:1183-1200

21
Marginal Donors Is there other Evidence?

22
Marginal Donors Is there other Evidence? Ware et al, (Lancet 2002) assessed 29 pairs of lungs rejected for use. 83% had no or mild pulmonary oedema, 74% had intact alveolar fluid clearance and 62% had normal histology
 assessed 29 pairs of lungs rejected for use. 83% had no or mild pulmonary oedema, 74% had intact alveolar fluid clearance and 62% had normal histology.")
23
Marginal Donors Is there other Evidence? Fisher et al (Thorax 2004) assessed inflammatory markers in lungs not used for transplant. There was no difference in BAL IL8 or neutrophil counts in the excluded lungs. Trend towards more infection in used lungs
 assessed inflammatory markers in lungs not used for transplant. There was no difference in BAL IL8 or neutrophil counts in the excluded lungs. Trend towards more infection in used lungs.")
24
Marginal Donors What is New? Where are we in 2010? What are the limits?

25
Marginal Donors AGE

26
TABLE IISUMMARY OF LITERATURE FOR THE USE OF OLDER LUNG DONORS nDesign Outcome Novick et al (1999) 284/5,052RetrospectiveDecreased survival Meyer et al (2000) 23/1,800RetrospectiveNo adverse affect on intermediate survival Bhorade et al (2000) 9/52RetrospectiveNo adverse affect on ventilator time, hospital stay or hospital survival Hosenpud et al (2001) 15,465RetrospectiveRisk factor for 1- and 5-year mortality. Adapted from Orens et al, JHLT 2003;22:1183-1200

27
ADULT LUNG TRANSPLANTS (1/1995-6/2001) Risk Factors for 1 Year Mortality Donor Age
 Risk Factors for 1 Year Mortality Donor Age")
28
ADULT LUNG TRANSPLANTS (1/1995-6/1997) Risk Factors for 5 Year Mortality Donor Age
 Risk Factors for 5 Year Mortality Donor Age")
29
HEART TRANSPLANTS : Donor Age by Year of Transplant

30
MEAN AGE OF CARDIAC DONORS IN THE UK, 1990 - 2002

31
Cause of Death of all Organ Donors(%) UK 1989-2002
 UK")
32
Marginal Donors OXYGENATION

33
TABLE III SUMMARY OF LITERATURE FOR DONOR BLOOD GASES (PaO2/F1O2 <300) n Study Design Outcome Harjula et al (1987) 1 Case report Primary graft failure Shumway et al (1994) 25 (1) Case series No adverse affect Sandaresan et al (1995) 6 Retrospective review No adverse affect Adapted from Orens et al, JHLT 2003;22:1183-1200 No Lower limit defined from the literature
 n Study Design Outcome Harjula et al (1987) 1 Case report Primary graft failure Shumway et al (1994) 25 (1) Case series No adverse affect Sandaresan et al (1995) 6 Retrospective review No adverse affect Adapted from Orens et al, JHLT 2003;22: No Lower limit defined from the literature")
34
From Luckraz et al JHLT 2005;24:470-473

35
Marginal Donors OXYGENATION Luckraz et al JHLT 2005;24:470-473 350 patients, all paired lungs, one institution Higher 30 day mortality No overall increase But 300 were HLTx, Ischaemic times c 3hrs

36
Aggressive management of lung donors classified as unacceptable: Excellent recipient survival one year after transplantation Straznicka, M et al. JTCVS August 2002, Volume 124, Number 2 250-258 Division of Cardiothoracic Surgery, University of California, Davis Medical Centre, Sacramento

37
Hypothesis Donor lungs with unacceptable PaO 2 /FiO 2 ratios (<20 kPa) can be made acceptable with aggressive management and that 30-day and 1- year recipient outcomes with these lungs would not be significantly different than outcomes of recipients with traditionally ideal lungs Aggressive management of lung donors classified as unacceptable: Excellent recipient survival one year after transplantation Straznicka, M et al., JTCVS August 2002, Volume 124, Number 2 250-258
 can be made acceptable with aggressive management and that 30-day and 1- year recipient outcomes with these lungs would not be significantly different than outcomes of recipients with traditionally ideal lungs Aggressive management of lung donors classified as unacceptable: Excellent recipient survival one year after transplantation Straznicka, M et al., JTCVS August 2002, Volume 124, Number")
38
Results of OPO management Aggressive management of lung donors classified as unacceptable: Excellent recipient survival one year after transplantation Straznicka, M et al., JTCVS August 2002, Volume 124, Number 2 250-258 103 = 13.7 kPa 463 = 61.7 kPa

39
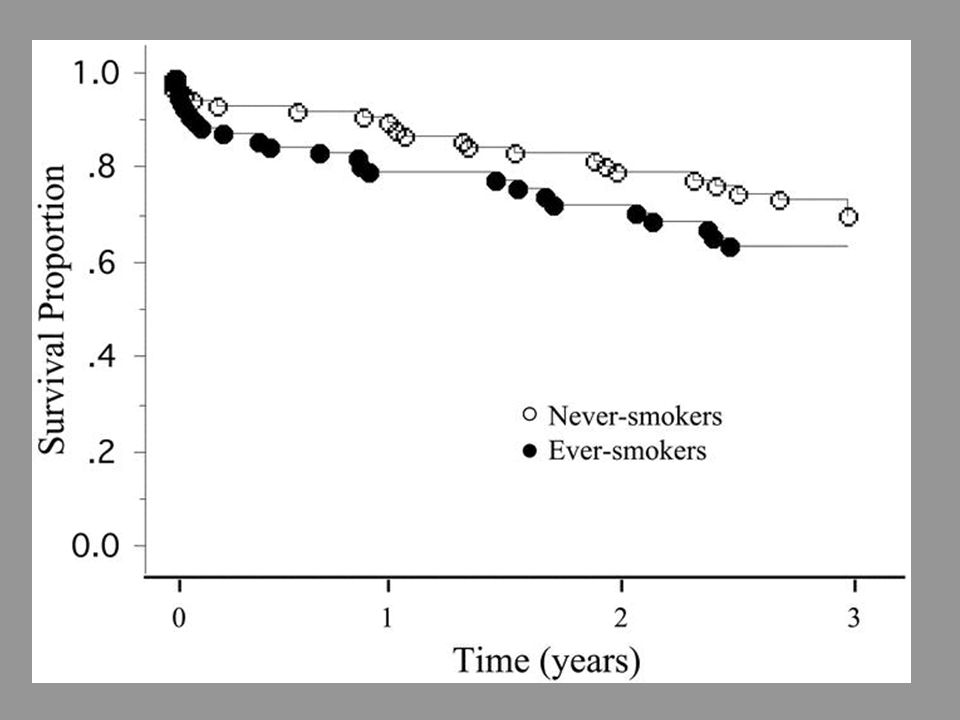
Kaplan-Meier survival curves Aggressive management of lung donors classified as unacceptable: Excellent recipient survival one year after transplantation Straznicka, M et al., JTCVS August 2002, Volume 124, Number 2 250-258

40
Conclusion Aggressive organ procurement management of donors initially considered unacceptable may increase the number of lungs available for transplantation Aggressive management of lung donors classified as unacceptable: Excellent recipient survival one year after transplantation Straznicka, M et al., JTCVS August 2002, Volume 124, Number 2 250-258

41
Marginal Donors SMOKING?

42
TABLE VII SUMMARY OF LITERATURE FOR DONOR SMOKING HISTORY Reference nDesign Outcome (survival) Gabbay et al (1999) 5/64 Retrospective review No adverse affect Sundaresan et al (1995) 9/44 Retrospective review No adverse affect Bhorade et al (2000) 15/52 Retrospective review No adverse affect (average 36 pack- years) No differences in short-term outcome with regard to post- operative ventilation or oxygenation, nor long-term survival to 2.5 to 3 years. Adapted from Orens et al, JHLT 2003;22:1183-1200

43
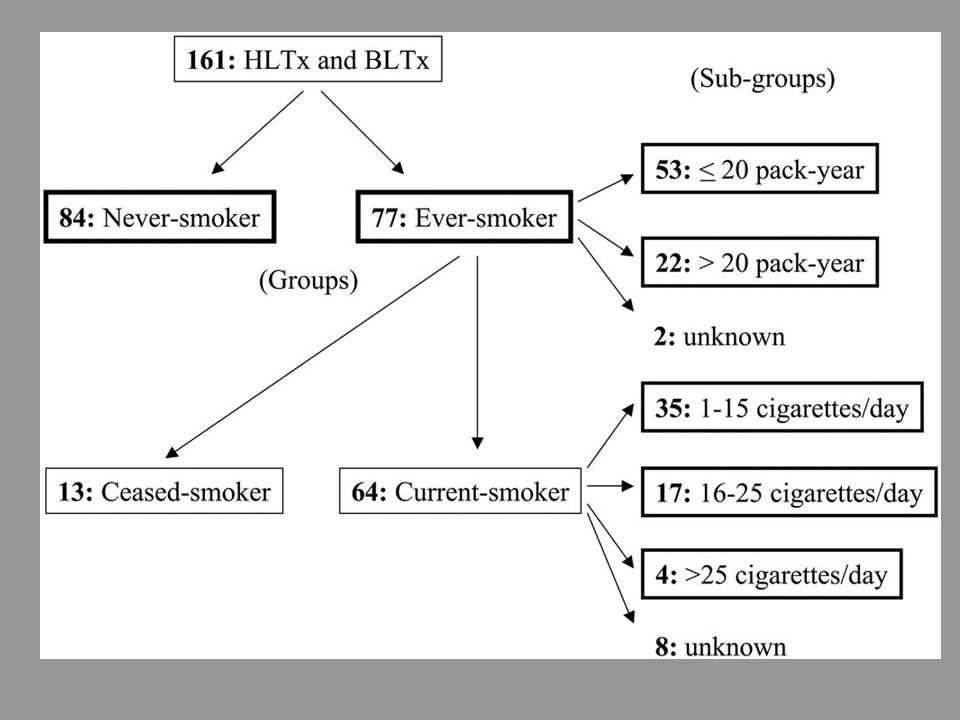
Marginal Donors SMOKING? Oto et al Transplantation 2004; 78:599-606 Significant early effect on oxygenation, ventilation time, and hospital stay, particularly for current and heavy dose smokers

46
Marginal Donors SMOKING? Oto et al Transplantation 2004; 78:599-606 Significant early effect on oxygenation, ventilation time, and hospital stay, particularly for current and heavy dose smokers Almost half donors fell into the high-risk category

47
Marginal Donors INFECTION?

48
Marginal Donors INFECTION? A positive donor gram stain does not predict outcome following lung transplantation Weill et al JHLT 2002; 21:555-558

49
Marginal Donors INFECTION? A positive donor gram stain does not predict outcome following lung transplantation Weill et al JHLT 2002; 21:555-558 Bacterial colonisation of the donor lower airways is a predictor of poor outcome in lung transplantation Avlonitis et al, EJCTS 2003; 24:601-607

50
Marginal Donors Bacterial colonisation of the donor lower airways is a predictor of poor outcome in lung transplantation Avlonitis et al, EJCTS 2003; 24:601-607 115 patients, donor BAL cultured 46% positive culture Longer ventilation, ITU, hospital stay for recipients with bacterially infected donors Worse short and log-term outcome No increase in BOS in one-year survivors

51
Avlonitis et al, EJCTS 2003; 24:601-607

52
Total Marginal Organs

53
Mean duration of Ventilation

54
Re-intubated (%)
")
55
Tracheostomy

56
Transplantation 2006;82:1273-9

57
Marginal Donors Conclusions Many indicators of “Marginality” have a price, at least in terms of early dysfunction, and eventually overall survival These risks, minimised by better donor care and improved post-op management, are still worth taking for our recipient population

58
Marginal Donors Conclusions Many indicators of “Marginality” have a price, at least in terms of early dysfunction, and eventually overall survival These risks, minimised by better donor care and improved post-op management, are still worth taking for our recipient population Who receives the marginal organ is unresolved

59
THE END

Similar presentations


: 1083-1141.>")

: 965-978 2013.>")
: 1009-1024.>")

: 1045-1095.>")
 吳惠東.>")



, FCCP. Assistant Professor.>")



: 1045-1095.>")



