Download presentation
Presentation is loading. Please wait.

1
Indications of ICD in 2010 Dr Mervat Aboulmaaty Professor of Cardiology Ain Shams University DAF 1 st EP course 2010

2
SCD Burden

3
SCD Risk

4
ICD Implantable Cardiovertor Defibrillator

5
First human implants Thoracotomy, multiple incisions Primary implanter= cardiac surgeon General anesthesia Long hospital stays Complications from major surgery Perioperative mortality up to 9% Nonprogrammable therapy High-energy shock only Device longevity 1.5 years Fewer than 1,000 implants/year 1980: Large Devices, Limited Battery Life, Abdominal Implant, Epicardial Leads

6
First-line therapy for VT/VF patients Treatment of atrial arrhythmias Cardiac resynchronization therapy for HF Transvenous, single incision Local anesthesia; conscious sedation Short hospital stays and few complications Perioperative mortality < 1% Programmable therapy options Single- or dual-chamber therapy Battery longevity up to 9 years* More than 100,000 implants/year Today: Small Devices, Long Battery Life, Pectoral Implant, Endocardial Leads *Battery longevity information in slide notes.

7
Atrium & Ventricle Bradycardia sensing & Pacing Atrium AT/AF tachyarrhythmia detection Antitachycardia pacing Cardioversion Ventricle VT/ VF detection Antitachycardia pacing Cardioversion Defibrillation Therapies Provided by Today’s Dual-Chamber ICDs

8
CRT-D Multisite ICD

9
Indications for ICDs Primary – Prevent a SCD event before it occurs Define patients at risk Secondary – Prevent SCD event after an initial event survival Exclude transient or reversible causes for VF

12
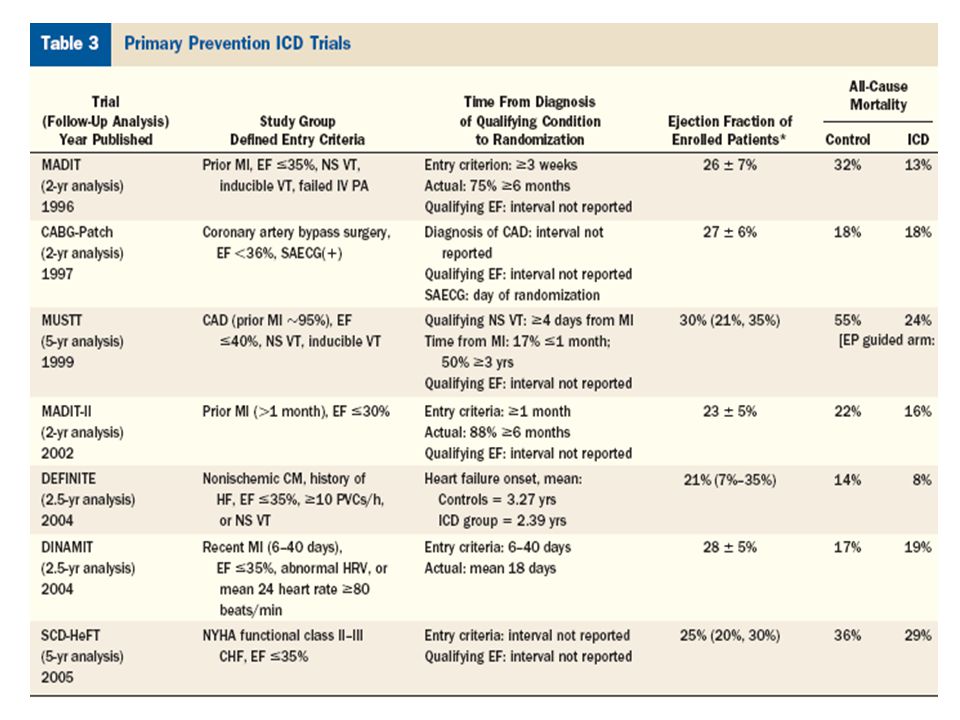
MADIT 1996 (196 patients) MADIT 1996 (196 patients) * M ild HF”:NYHA Class I and II ; High-risk”:EF ≤30%; QRS ≥130ms MADIT II 2002 (1232 patients) MADIT II 2002 (1232 patients) MADIT-CRT 2005 (1820 patients) MADIT-CRT 2005 (1820 patients) Clinical Question: Can prophylactic ICD therapy improve survival in high risk HF patients when compared to medical therapy alone? Endpoint: All-cause mortality. Key Finding: Use of ICDs resulted in a 54% reduction in the mortality rate in the ICD group as compared to the conventional medical therapy group (p value: 0.009) Clinical Question: Can heart attack survivors with impaired heart function (EF≤30%), and no other risk stratification, benefit from ICD therapy versus conventional therapy alone? Endpoint: All-cause mortality. Key Finding: Use of ICDs resulted in a 31% reduction in the risk of death in heart attack survivors (p value: 0.016). As a result, patients no longer have to undergo invasive electrophysiological testing to receive the ICD therapy Clinical Question: Does early intervention with CRT-D slow the progression of HF in high-risk patients* with mild HF* when compared to ICD-only therapy? Endpoint: All-cause mortality OR first HF event. Key finding: CRT-D therapy is associated with a significant 34% reduction in death or first HF event when compared to ICD therapy alone (p value: 0.001)
 Clinical Question: Can heart attack survivors with impaired heart function (EF≤30%), and no other risk stratification, benefit from ICD therapy versus conventional therapy alone. Endpoint: All-cause mortality. Key Finding: Use of ICDs resulted in a 31% reduction in the risk of death in heart attack survivors (p value: 0.016). As a result, patients no longer have to undergo invasive electrophysiological testing to receive the ICD therapy Clinical Question: Does early intervention with CRT-D slow the progression of HF in high-risk patients* with mild HF* when compared to ICD-only therapy. Endpoint: All-cause mortality OR first HF event. Key finding: CRT-D therapy is associated with a significant 34% reduction in death or first HF event when compared to ICD therapy alone (p value: 0.001).")
13
1 Moss AJ. N Engl J Med. 1996;335:1933-40. 2 Buxton AE. N Engl J Med. 1999;341:1882-90. 3 Moss AJ. N Engl J Med. 2002;346:877-83 4 Moss AJ. Presented before ACC 51st Annual Scientific Sessions, Late Breaking Clinical Trials, March 19, 2002. 5 The AVID Investigators. N Engl J Med. 1997;337:1576-83. 6 Kuck K. Circ. 2000;102:748-54. 7 Connolly S. Circ. 2000:101:1297-1302. ICD mortality reductions in primary prevention trials are equal to or greater than those in secondary prevention trials. 13, 42 5 7 6 Reductions in Mortality with ICD Therapy 54% 75% 55% 76% 31% 61% 27 months39 months20 months 31% 56% 28% 59% 20% 33% % Mortality Reduction w/ ICD Rx 3 Years

15
Class I Documented survivors of SCD due to VF 40days post MI + LVEF≤ 35 + NYHA II/III 40 days post MI + LVEF≤ 30 + NYHA I Non ischemic cardiomyopathy + LVEF≤ 35 + NYHA II/III Non sustained VT post MI + sustained VT/VF by EPS+ LVEF ≤ 40 Structural heart disease + sustained VT Syncope + unstable VT/VF by EPS

16
Class IIA LQTS + syncope/VT (on β blockers) Unexplained syncope + DCM + significant LV dysfunction Sustained VT + normal LV CPVT + syncope/VT (on β blockers) High risk ARVD High risk HCM Brugada syndrome + syncope/VT
 Unexplained syncope + DCM + significant LV dysfunction Sustained VT + normal LV CPVT + syncope/VT (on β blockers) High risk ARVD High risk HCM Brugada syndrome + syncope/VT")
18
Indications for ICD in HF patients

19
Guidelines of ICD in a Pocket

20
Indications for ICD implantation Class III ICD is NOT indicated IN Syncope of undetermined cause no VT induced NO structural HD Incessant VT VF VT/VF resulting from arrhythmias amenable for ablation as WPW Fasicular VT VT due to reversible disorder Significant psychological disorder Terminal illness life expectancy <6months

21
55 yr old, first hour of Acute MI

22
ICDs are reliable devices that have the potential to add quality years of life for appropriate candidates. There are scientifically-derived guidelines for their prescription that are limited by the scope of the clinical trials and observational data. Cardiologists should recommend ICD devices to their individual patients based on the current guidelines. Conclusions

23
ICD Programming Zone Rate (bpm) Cycle Length (ms) No. of Beats to DetectTherapies VF> 250<24018 of 2430 J × 6 FVT201-250299-240 18 Burst (1), 30 J × 6 VT< 150-200400-30016Burst (2), ramp (1), 20 J, 30 J × 3
, 30 J × 6 VT< Burst (2), ramp (1), 20 J, 30 J × 3.")
24
How ICD works?

25
I C D I N T E R R O G A T I O N

26
VT Burst 1 Sinus I C D I N T E R R O G A T I O N

27
Burst Acc. VT VT I C D I N T E R R O G A T I O N

28
DC Sinus Acc.VT Cont.

29
Thank you

Similar presentations











 Arthur J. Moss, MD for the MADIT-RIT Executive Committee AHA Late Breaking Trials November.>")



>")


 Janet McComb Freeman Hospital Newcastle upon Tyne.>")



