Download presentation
Presentation is loading. Please wait.

1
Maternal Mortality & the MDGs Deborah Maine Professor, International Health Boston University, School of Public Health

2
MDG Goal: Improve maternal health Target: Reduce the MM Ratio by 3/4 by 2015 Indicators: l Maternal mortality ratio l Proportion of births attended by skilled health personnel

3
The MDG for MM Is it realistic ?

4
History MMRs Sri Lanka: 1947 -- 1500 1960 -- 250 1980 -- 100 Malaysia: 1950 > 500 1975 < 100

5
To reduce MM … l Need to understand the epidemiology of maternal mortality [MM] l A counterintuitive phenomenon l Many “obvious” approaches don’t work, e.g. risk screening, training TBAs
![To reduce MM … l Need to understand the epidemiology of maternal mortality [MM] l A counterintuitive phenomenon l Many obvious approaches don’t work, e.g.](http://images.slideplayer.com/19/5756842/slides/slide_5.jpg "risk screening, training TBAs.")
6
Maternal Mortality RegionMM RatioLifetime Risk 1 in … Africa83020 Asia33094 Latin America190160 North America172,500 World40074

7
Causes of Direct Obstetric Deaths The “Big 5” l Hemorrhage l Infection l Hypertensive diseases l Obstructed labor l Unsafe induced abortion

8
The Way Programs Should Work Evidence Interventions Indicators Strategy

9
Interventions Indicators Strategy Assumptions The way it often works

10
Assumption If we just take very good care of pregnant women, few will develop serious obstetric complications.

11
History: Prenatal Care l 1910-15 first clinics in UK (and US) l By 1930, 80% pregnant women in UK have prenatal care l But maternal mortality did not decline
 l By 1930, 80% pregnant women in UK have prenatal care l But maternal mortality did not decline")
12
TBAs & “Clean Delivery” In Matlab, Bangladesh, TBAs were trained to use clean delivery practices. The did use these practices, but maternal deaths due to infection did not decline.

13
Assumption Through prenatal screening, We can identify the women who will need medical care

14
The Math of Prediction It works for groups but not for individuals.

15
Example: Matlab, Bangladesh 1968-70 Maternal Age 10-1420-29 MM Ratio 1770450 Relative Risk 3.91 # Births 50911,286 # Deaths 951

16
Example: United Kingdom 1985-87 Maternal Age20-2445+ MM Ratio37188 Relative Risk1 5.1 # Deaths242

17
Risk and Prediction (cont.) A big risk in a small population = few deaths A small risk in a big population = many deaths
 A big risk in a small population = few deaths A small risk in a big population = many deaths")
18
In Short... Once a woman is pregnant most serious obstetric complications cannot be predicted or prevented, but they can be treated.

19
So All pregnant women need access to emergency obstetric care (EmOC)
")
20
Sri Lanka & Malaysia How did they do it ? l Expanding access to effective maternity care by midwives and doctors l Improving utilization and quality of care with emphasis on making life-saving care free. The World Bank, 2003

21
Assumption EmOC is “Hi-Tech”

22
Signal Functions of Basic EmOC : l Parenteral antibiotics, oxytocics, anticonvulsants l Manual removal of placenta l Removal of retained products l Assisted vaginal delivery l Neonatal resuscitation (new) Should be at health centers
 Should be at health centers")
23
Signal Functions of Comprehensive EmOC: l All Basic EmOC functions l Blood transfusion l Surgery (c-section) Should be at District Hospitals
 Should be at District Hospitals")
24
EmOC is not “Hi Tech” It is mostly 1950s medicine !

25
EmOC is the foundation Emergency Obstetric Care Skilled Attendant Referral Risk Screening Social Mobilization Waiting Homes TBA Training Antenatal Care

26
Assumption EmOC is too expensive Community-based workers are more affordable

27
A cost-effectiveness exercise: unit cost Dollars $350 $10,000 $30,000

28
Cost (cont.) Suppose, per district, there are: l 100 MCHW s l 4 health centers l 1 district hospital
 Suppose, per district, there are: l 100 MCHW s l 4 health centers l 1 district hospital")
29
Estimated program cost (in $000s) Dollars 30 40 35
 Dollars")
30
Estimated obstetric deaths prevented (%) 50 Percent 25 15
 50 Percent 25 15")
31
Estimated cost per death averted ($000) $580 $845 $217
 $580 $845 $217")
32
In short … Something that is not effective can never be cost-effective.

33
Measuring Progress: Are we measuring the right things?

34
The Way It Should Work Evidence Interventions Indicators Strategy But sometimes …

35
MDG Goal: Improve maternal health Target: Reduce the MM Ratio by 3/4 by 2015 Indicators: l Maternal mortality ratio l Proportion of births attended by skilled health personnel

36
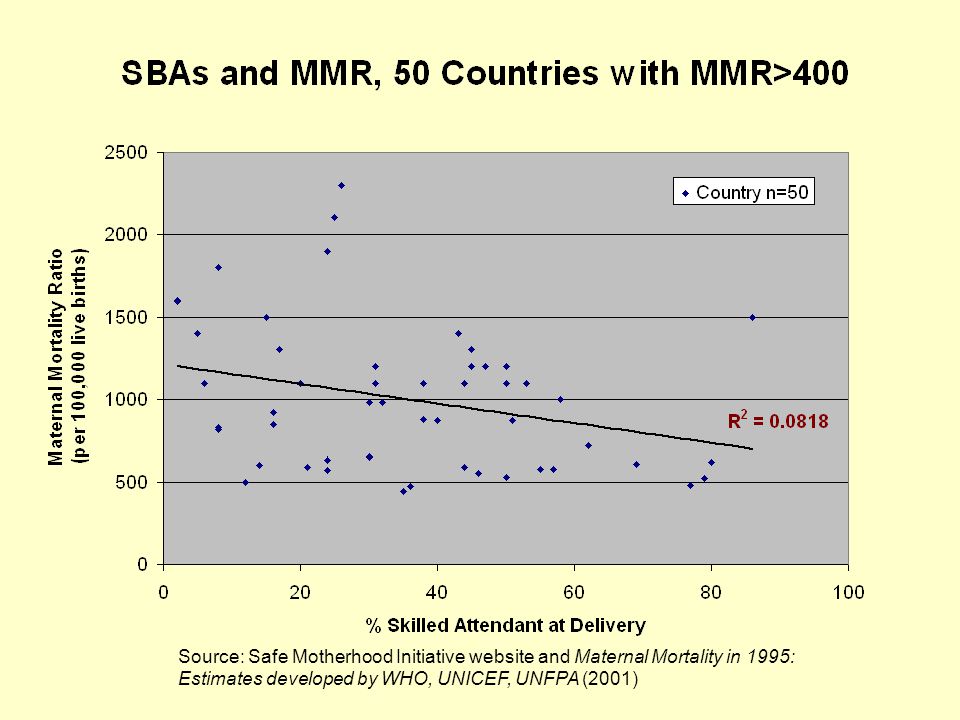
Promoting SBAs What is the evidence base for this policy?

37
Source: Safe Motherhood Initiative website and Maternal Mortality in 1995: Estimates developed by WHO, UNICEF, UNFPA (2001)
")
39
This shows: the relationship between delivery by SBAs and MMR is not strong for high-mortality countries

40
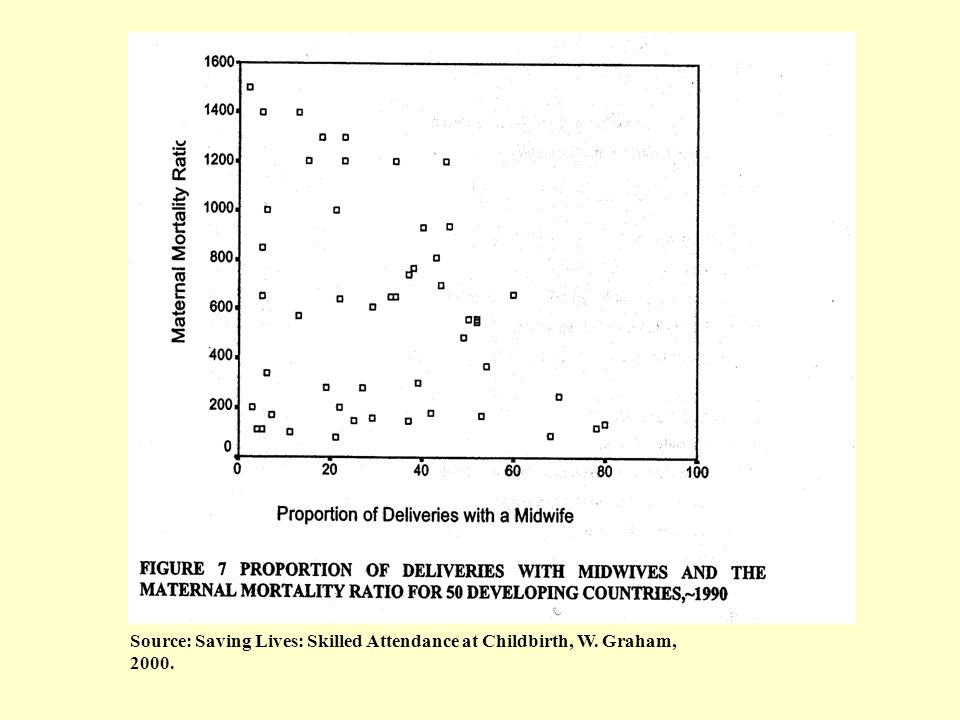
Source: Saving Lives: Skilled Attendance at Childbirth, W. Graham, 2000.

42
This shows: the relationship between delivery by midwives and reduced MMR is not clearcut – probably due to regional variation in what midwives are trained and permitted to do.

43
Skilled Attendants need to be part of a functioning health system To Be Effective

44
Sri Lanka, 1970s > Health Facilities SBAs

45
Many Proposed Programs Health Facilities SBAs

46
In Reducing Maternal Deaths There are really only 3 issues: l COVERAGE OF SERVICES l QUALITY OF CARE l UTILIZATION OF SERVICES

47
The Road toMaternal Mortality Reduction: Shortcuts or Detours ?

48
Pseudo-Interventions l “Safe Birth Kits”: No evidence of effectiveness in reducing maternal deaths, but consume effort, attention and funds. l Advocacy for Advocacy: If not linked to programs, advocacy can be a detour.

49
1-Complication MM Programs Example: Home-based prevention of post-partum hemorrhage (PPH) Hemorrhage = 25% of maternal deaths Perhaps ½ preventable = 12.5%
 Hemorrhage = 25% of maternal deaths Perhaps ½ preventable = 12.5%")
50
Semi-Skilled Attendants If you leave the skills out of Skilled Birth Attendant what do you get?

51
Institutional Delivery Targets Easy to measure, but no indication of quality of care You can reach the target But miss the goal !

52
“In the Meantime …” If we don’t get started now fixing health systems in 20 years we will still be in the meantime.

53
General Lesson: We must build health systems l Need a strong evidence base l Training and equipment are never enough l Management systems are crucial l Even skilled personnel need support l Learn from expensive failures

Similar presentations