Download presentation
Presentation is loading. Please wait.

1
Adaptive Designs for Clinical Trials
Frank Bretz Novartis 24 April 2013, Tel Aviv

2
What are Adaptive Designs?

3
Three definitions of adaptive designs
By adaptive design we refer to a clinical study design that uses accumulating data to decide how to modify aspects of the study as it continues, without undermining the validity and integrity of the trial. PhRMA White Paper (2006) A study design is called “adaptive” if statistical methodology allows the modification of a design element (e.g. sample-size, randomisation ratio, number of treatment arms) at an interim analysis with full control of the type I error. EMEA Reflection Paper (2007) An adaptive design clinical study is defined as a study that includes a prospectively planned opportunity for modification of one or more specified aspects of the study design and hypotheses based on analysis of data (usually interim data) from subjects in the study. FDA Draft Guidance for Industry (2010) 3
 A study design is called adaptive if statistical methodology allows the modification of a design element (e.g. sample-size, randomisation ratio, number of treatment arms) at an interim analysis with full control of the type I error. EMEA Reflection Paper (2007) An adaptive design clinical study is defined as a study that includes a prospectively planned opportunity for modification of one or more specified aspects of the study design and hypotheses based on analysis of data (usually interim data) from subjects in the study. FDA Draft Guidance for Industry (2010) 3.")
4
Major types of adaptive designs
Adaptive randomization Adaptive modifications of treatment randomization probabilities Adaptive dose finding Adaptive dose escalation in, for example, Oncology Phase I trials Adaptive dose finding in Phase II studies Group sequential designs Early stopping either for futility or success (frequentist or Bayesian rules) Adaptive sample size re-estimation Blinded or unblinded sample size re-estimation based on interim data Adaptive designs for confirmatory trials Adaptive designs in the sense of the EMEA Reflection Paper (2007) | Introduction to Drug Development and Pharmaceutical Statistics |Adaptive Design | 2012
 Adaptive sample size re-estimation. Blinded or unblinded sample size re-estimation based on interim data. Adaptive designs for confirmatory trials. Adaptive designs in the sense of the EMEA Reflection Paper (2007) | Introduction to Drug Development and Pharmaceutical Statistics |Adaptive Design |")
5
Adaptive Dose Finding

6
Adaptive dose finding – The idea
Prior to study the true position of dose response curve is unknown In the adaptive dose finding approach, a small number of patients on many initial doses are used to outline the unknown dose-response. Region of interest X X X X X As the dose response emerges more patients are allocated to doses (including new doses) within the dose- range of interest. In addition the number of patients allocated to ‘non-informative’ doses (‘wasted doses’) is decreased. Response X X X X X X Initial doses Dose X = Mean dose response after a pre-defined number of patients
 within the dose- range of interest. In addition the number of patients allocated to ‘non-informative’ doses (‘wasted doses’) is decreased. Response. X. X. X. X. X. X. Initial doses. Dose. X = Mean dose response after a pre-defined number of patients.")
7
Benefit of adaptive dose finding designs
When evaluating adaptive designs from a purely inferential perspective (precision in estimating target dose or dose response) via simulations: moderate gains in most scenarios substantial gains in some scenarios e.g. extreme mis-specification of initial design but sometimes adaptive designs perform similar or even worse than fixed designs Can mathematical/analytical considerations confirm these findings and provide more insight When does an adaptive design pay off? Consider a simplified setup, to remove interfering factors 7 7 7
 via simulations: moderate gains in most scenarios. substantial gains in some scenarios. e.g. extreme mis-specification of initial design. but sometimes adaptive designs perform similar or even worse than fixed designs. Can mathematical/analytical considerations confirm these findings and provide more insight. When does an adaptive design pay off Consider a simplified setup, to remove interfering factors")
8
Results from Dette, Bornkamp and Bretz (2013)
Goal: Estimate the parameters θ in a non-linear model Compare two designs (in terms of mean squared error) Fixed design: N observations according to optimal design based on initial parameter guess θ0 Two-stage adaptive design: Stage 1: N0 = p0N observations according to design based on θ0 Interim: Estimate θ with maximum likelihood Stage 2: Remaining N – N0 observations according to the optimal design based on the interim estimate At trial end calculate the maximum likelihood estimate based on complete set of N observations Which design is more efficient and estimates θ more precisely? 8 8 8
 Fixed design: N observations according to optimal design based on initial parameter guess θ0. Two-stage adaptive design: Stage 1: N0 = p0N observations according to design based on θ0. Interim: Estimate θ with maximum likelihood. Stage 2: Remaining N – N0 observations according to the optimal design based on the interim estimate. At trial end calculate the maximum likelihood estimate based on complete set of N observations. Which design is more efficient and estimates θ more precisely")
9
Analytical approximation
9 9 9
10
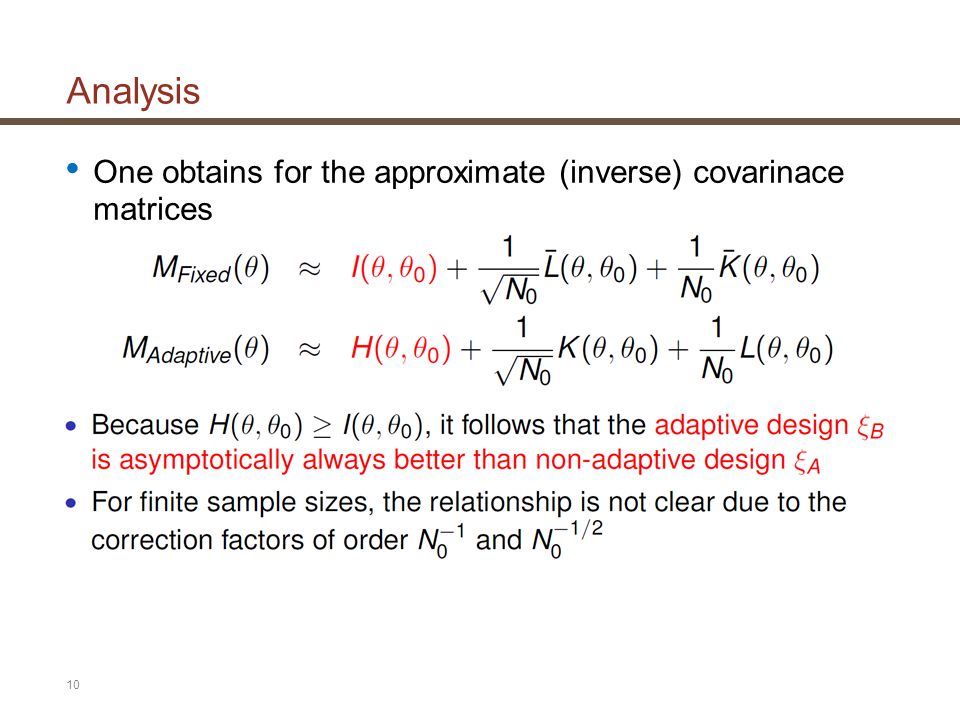
Analysis One obtains for the approximate (inverse) covarinace matrices
10 10 10
11
Exponential Regression Model
Assume the model with unknown parameterguess θ and initial guess guess θ0 Exponential model with unknown parameter θ = 1 and initial guesses θ0 = 1.2, 2, 3 Which design estimates θ more precisely: the fixed design or the two-stage adaptive design? 11 11 11

12
Exponential Regression Model – Results
Relative efficiency of adaptive versus non-adaptive design for N = 100, θ = 1. Efficiency > 1 indicates that the adaptive design is better. Main factors: variability / sample size at interim, timing of interim, suitability of start design 12 12 12

13
Adaptive Designs for Confirmatory Trials

14
Treatment selection Overview
Phase II Phase III Dose A Dose B Dose C Placebo Time Stage 1 Stage 2 Dose A Dose B Dose C Test Dose B against Placebo using data from both stages Placebo Interim Analysis

15
Type I error rate control Sources and related approaches
Sources of potential Type I error rate inflation Approaches for error rate control Early rejection of null hypotheses at interim analysis Classical group sequential plans (e.g. α- spending approach) Adaptation of design features and combination of information across trial stages Combination of p-values (e.g. inverse normal method, Fisher’s combination test) Multiple hypothesis testing (e.g. with adaptive selection of hypotheses at interim analysis) Multiple testing methodology (e.g. closed test procedures) All three approaches can be combined
 Adaptation of design features and combination of information across trial stages. Combination of p-values. (e.g. inverse normal method, Fisher’s combination test) Multiple hypothesis testing (e.g. with adaptive selection of hypotheses at interim analysis) Multiple testing methodology. (e.g. closed test procedures) All three approaches can be combined.")
16
Principles of adaptive designs
Single null hypothesis H (no treatment difference) Two stages, i.e., one interim analysis p 0 Stage 1 reject H Continue to second stage futility stop; retain H Stage 2 q reject H retain H
 Two stages, i.e., one interim analysis. p. 0 1 0 1. Stage 1. reject H. Continue to second stage. futility stop; retain H Stage 2. q. reject H. retain H.")
17
Principles of adaptive designs
Fisher‘s product combination test (Bauer and Köhne, 1994) At interim, stop if p ≤ α1 (reject H) or p ≥ α0 (retain H) Else, α1 < p < α0, continue the study, resulting in q Final decision: Reject H, if and only if Alternatively, define the conditional error function and reject H, if and only if q ≤ A(p) Weighted inverse normal method (Lehmacher and Wassmer, 1999; Cui, Hung, and Wang, 1999) 1) A(p1) is based on the assumption of p1, p2 being independently U[0, 1] distributed (but recall the p-clud condition) 2) A(p1) is the maximum value p2 can achieve, s.t. we reject H at the final stage
 At interim, stop if p ≤ α1 (reject H) or p ≥ α0 (retain H) Else, α1 < p < α0, continue the study, resulting in q. Final decision: Reject H, if and only if. Alternatively, define the conditional error function. and reject H, if and only if q ≤ A(p) Weighted inverse normal method (Lehmacher and Wassmer, 1999; Cui, Hung, and Wang, 1999) 1) A(p1) is based on the assumption of p1, p2 being independently U[0, 1] distributed (but recall the p-clud condition) 2) A(p1) is the maximum value p2 can achieve, s.t. we reject H at the final stage.")
18
Closed test procedure General principle to construct powerful multiple test procedures Schematic diagram for 2 hypotheses H1 and H2: Rejection rule: Reject H1 (say) at overall α, if H1 and H12 are rejected, each at local level α. Operationally: Test H12 at local level α; if rejected, proceed; otherwise stop Test H1 and H2 each at local level α. Reject H1 (H2) overall if H12 and H1 (H2) are rejected locally Type I error rate control in the strong sense
 at overall α, if H1 and H12 are rejected, each at local level α. Operationally: Test H12 at local level α; if rejected, proceed; otherwise stop. Test H1 and H2 each at local level α. Reject H1 (H2) overall if H12 and H1 (H2) are rejected locally. Type I error rate control in the strong sense.")
19
Multiple testing in adaptive designs
Test all (intersection) hypotheses with combination tests 1) So far, we have no adaptive choice of hypotheses at interim. In what follows I will show some examples, on how to adapt the results on this slide to some standard problems (both generic and more specific problems). But before I come to the examples, here is a flow chart ...
 hypotheses with combination tests. 1) So far, we have no adaptive choice of hypotheses at interim. In what follows I will show some examples, on how to adapt the results on this slide to some standard problems (both generic and more specific problems). But before I come to the examples, here is a flow chart ...")
20
Generic example Treatment selection: assume that at interim it is decided to continue with the first treatment H1 is rejected if q1 < min{A(p12), A(p1)} Similar: subgroup selection, endpoint selection
, A(p1)} Similar: subgroup selection, endpoint selection.")
21
Summary Variety of different adaptive designs available for clinical trials Potential advantages offered by adaptive designs need to be balanced against any perceived risks or complexities Some types of adaptations convey limited information for which it seems difficult to envision how the trial might be compromised. Others convey more information, but extra steps might be implemented to mitigate the risk Extensive regulatory guidance is available, mostly applicable in the context of confirmatory drug development.

Similar presentations










 Li and Devan.>")





 and likelihood ratio (LR) test>")


