Download presentation
Presentation is loading. Please wait.

1
Diagnostic Imaging Approach to a Supratentorial SOL in an Adult
Antoinette Reinders Dept of Diagnostic and Interventional Radiology University of the Free State Aug 2012

2
Approach Age Location Tumour spread Characteristics on CT and MRI
Intra vs extra axial Anatomical compartment Midline crossing Tumour spread Characteristics on CT and MRI Spectroscopy Calcification/edema/mass effect Enhancement Differential diagnoses “Tumor mimickers”

3
Brain Tumours Smithuis R, Montanera W. Brain Tumor – systematic approach. Available from URL:

4
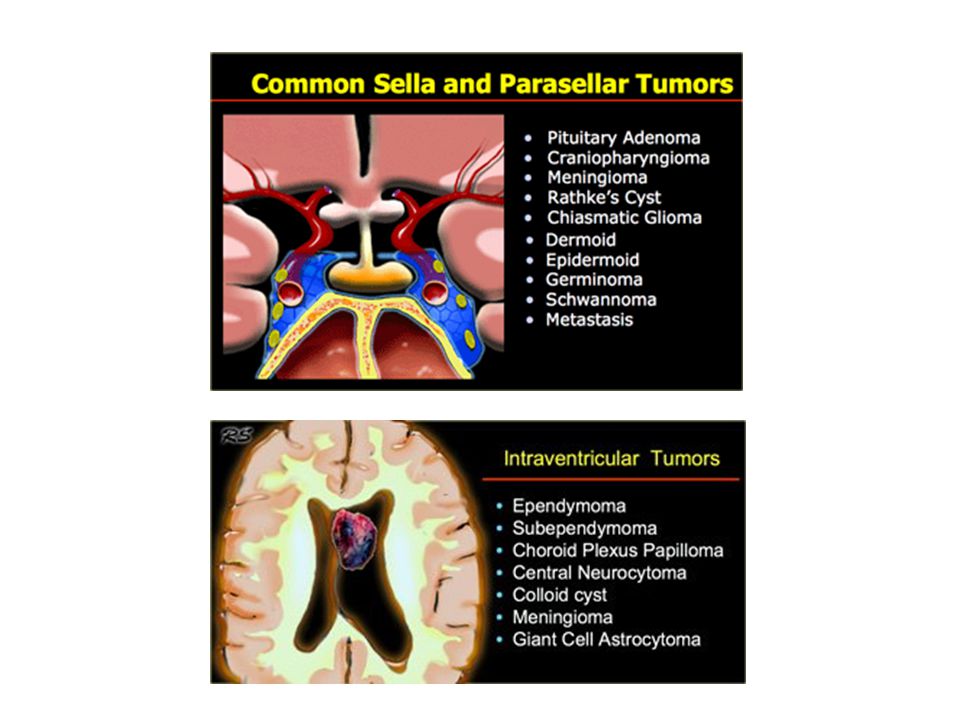
Major Anatomical considerations
Intra axial Hemispheres (cerebrum/cerebellum) Brainstem Sellar/supraseller Pineal Ventricular Extra axial Dural based Bone tumours Nasopharyngeal tumours
 Brainstem. Sellar/supraseller. Pineal. Ventricular. Extra axial. Dural based. Bone tumours. Nasopharyngeal tumours.")
5
Approach Location Intra-axial vs Extra-axial
Smithuis R, Montanera W. Brain Tumor – systematic approach. Available from URL:

6
Extra axial tumour Smithuis R, Montanera W. Brain Tumor – systematic approach. Available from URL:

7
Intra vs Extra axial Smithuis R, Montanera W. Brain Tumor – systematic approach. Available from URL:

8
Approach Location Grey matter White matter Grey/white matter interface
Cortical/subcortical White matter Grey/white matter interface Dural surface Abut the meninges Ventricles Foramen of Monroe Trigonum of the lateral ventricles Pineal gland Sella/suprasellar

9
Robert Wood Johnson University Hospital. Available from URL:

11
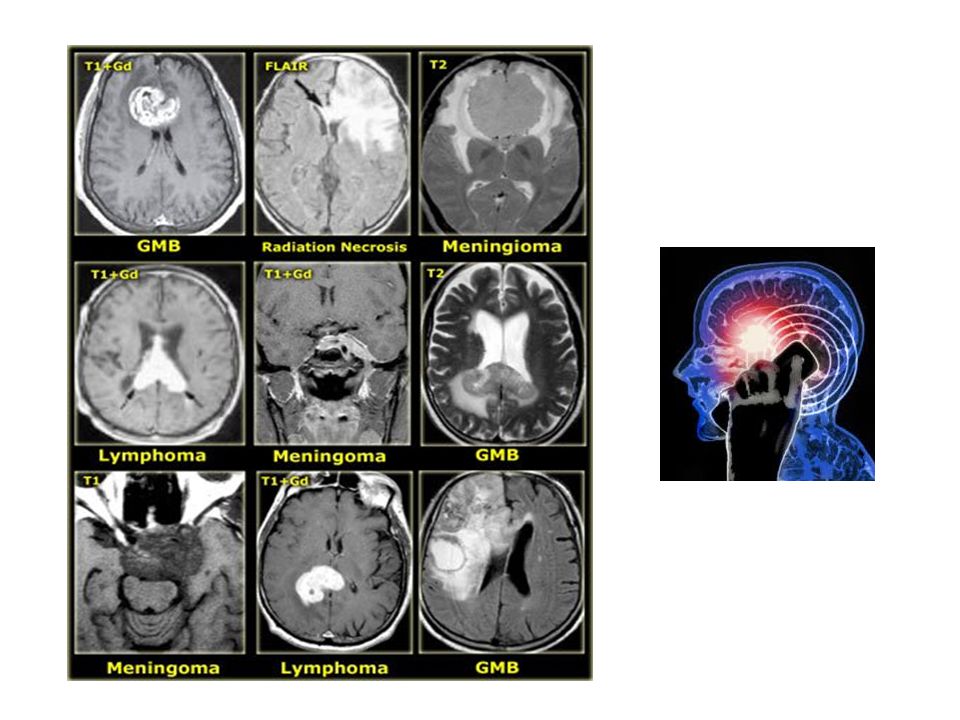
Approach Cross midline Multifocal disease
Glioblastoma Multiforme, Radiation necrosis, Meningioma, Lymphoma, Epidermoid cyst, MS Multifocal disease Phacomatoses NF1: Optic gliomas, astrocytomas NF2: Meningiomas, Ependymomas, Schwannomas, Choroid plexus papillomas TS: Subependymal tubers, Giant cell astrocytomas VHL: Hemangioblastomas

13
Approach Tumour spread Subarachnoid seeding WM Tracts Foramina PNET
Ependymoma GBM Lymphoma Oligodendroglioma WM Tracts Astrocytoma Pilocytic, Fibrillary, Gemistocytic, Protoplasmic Foramina

14
Tumour Spread Pleomorphic xantoastrocytoma Ependymoma of 4th ventricle

15
Approach Characteristics MRI CT Edema Cystic Mass effect
Fat containing Spectroscopy CT Calcifications Haemorrhage Homogenous or heterogenous appearance Periosteal reaction

16
Characteristics on CT

17
Haemorrhage Common haemorrhage Not common haemorrhage
Glioblastoma multiforme Germ cell tumours Metastases Choroid Thyroid Bronchus Mamma/melanoma Renal Medulloblastoma Craniopharyngioma Colloid cysts/central neurocytoma Oligodendrogliomas Ependymal Giant cell astrocytomas Chordoma Epidermoid/dermoid

18
Characteristics on MRI

19
Characteristics on MRI

20
Diffusion Weighted Imaging
Abscesses, infarcts have ABNORMAL diffusion – restriction Tumours have NORMAL diffusion – no restriction

21
Approach Enhancement Destruction of BBB in order to enhance
Homogenous vs heterogenous enhancement Enhancement of gliomas = higher grade of malignancy NB in follow up Diffusion weighted Restricted diffusion in abscesses and not in tumours Smithuis R, Montanera W. Brain Tumor – systematic approach. Available from URL:

22
Approach No Enhancement Patchy Enhancement Homogenous Enhancement
Low grade astrocytomas Metastases Cystic non tumour lesions Oligodendroglioma Lymphoma Dermoid GBM Germinoma and pineal tumours Epidermoid Radiation necrosis Pituatary macroadenoma Arachnoid cyst Pilocytic astrocytoma Hemangioblastoma Gangliocytoma Meningioma Schwannoma

23
Common things..... Astrocytoma Oligodendroglioma

24
Approach Differential diagnoses
Dural based – Meningioma, Dural metastases, Sarcoid, Haemangiopericytomas, pineoblastoma, lymphoma Cortical based – Dural AV malformation, Herpes encephalitis Multifocal disease – Septic emboli, Abscesses and Multiple Sclerosis Sellar - Aneurysm

25
Take home points... Age of patient Location Tumour spread
Intra vs extra axial Crossing midline Multifocal disease Tumour spread Characteristics on CT/MRI Calcifications Haemorrhage Spectroscopy Enhancement pattern Differential diagnoses

26
Cellphones? “Although our results overall do not indicate an increased risk of glioma in relation to mobile phone use, the possible risk in the most heavily exposed part of the brain with long-term use needs to be explored further before firm conclusions can be drawn.” Int J Cancer Apr 15;120(8): Mobile phone use and risk of glioma in 5 North European countries. Raised risks of glioma with mobile phone use, as reported by one (Swedish) study forming the basis of the IARC's re-evaluation of mobile phone exposure, are not consistent with observed incidence trends in US population data, although the US data could be consistent with the modest excess risks in the Interphone study. BMJ Mar 8;344:e1147. doi: /bmj.e1147. Mobile phone use and glioma risk: comparison of epidemiological study results with incidence trends in the United States. BMJ May 1;344:e3083; author reply e3088. doi: /bmj.e3083. Association of mobile phone use with adult brain cancer remains plausible Davis DL, Miller AB, Philips A
: Mobile phone use and risk of glioma in 5 North European countries. Raised risks of glioma with mobile phone use, as reported by one (Swedish) study forming the basis of the IARC s re-evaluation of mobile phone exposure, are not consistent with observed incidence trends in US population data, although the US data could be consistent with the modest excess risks in the Interphone study. BMJ Mar 8;344:e1147. doi: /bmj.e1147. Mobile phone use and glioma risk: comparison of epidemiological study results with incidence trends in the United States. BMJ May 1;344:e3083; author reply e3088. doi: /bmj.e3083. Association of mobile phone use with adult brain cancer remains plausible. Davis DL, Miller AB, Philips A.")
27
Bibliography Smithuis R, Montanera W. Brain Tumor – systematic approach. Available from URL: Koeller KK, Sandberg GD. Cerebral intraventricular Neoplasms: Radiologic-Pathologic correlation. RadioGraphics 2002; 22: Hoon Shin J, Kyu Lee H, Khang SK et al. Neuronal tumors of the central nervous system: radiologic findings and pathologic correlation. RadioGraphics 2002; 22: Robert Wood Johnson University Hospital. Available from URL: Dahnert W. Radiology Review Manual 6th ed. Lippincott Williams & Wilkins 2007 Weissleder et al. Primer of Diagnostic Imaging 4th ed. Mosby Elsevier 2007

Similar presentations