Download presentation
Presentation is loading. Please wait.

1
Alexander Stein University Cancer Center Hamburg, Germany
ESMO Consensus Conference: Interactive Session on Colorectal Cancer Guidelines A clinical case presentation on advanced colon cancer (first and second line therapy) Alexander Stein University Cancer Center Hamburg, Germany
 Alexander Stein. University Cancer Center Hamburg, Germany.")
2
Disclosure Honoraria from Roche and Merck

3
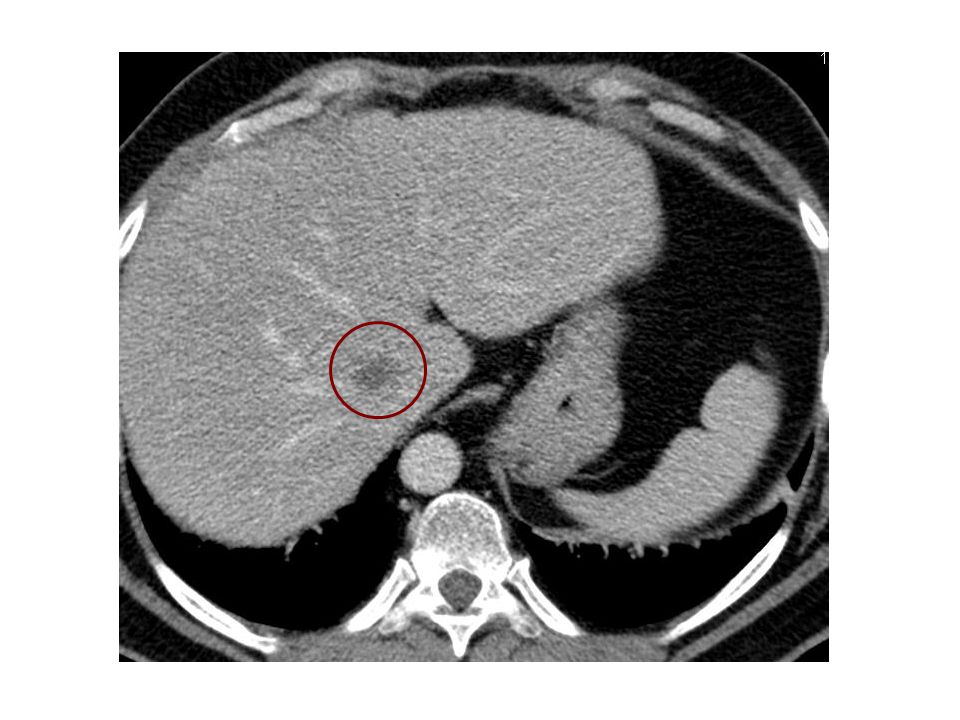
Case presentation male, 64 years of age, ECOG 0
no relevant comorbidity routine abdominal ultrasound revealed suspicious liver lesions CT chest/abdomen 3 liver lesions up to 2.5cm 3 suspicious pulmonary lesions up to 1cm single bone lesion 1.8cm mixed osteoplastic/osteolytic (left os ileum) thickening of colonic wall (descendens)
 thickening of colonic wall (descendens)")
5
Case presentation colonoscopy: non obstructive tumor without bleeding signs colon descendens histology: adenocarcinoma CEA value 245 ng/ml colon carcinoma with synchronous liver and lung metastates and potential bone involvement

6
Further diagnostics PET scan liver and lung lesions positive, bone lesion negative bone scan weakly positive determination of KRAS status wildtype ESMO consensus guidelines for management of patients with colon and rectal cancer 2012. KRAS mutation precludes efficacy of treatment with anti-EGFR antibodies and KRAS status determination is therefore mandatory before treatment [I, A].

7
Acc. to ESMO guidelines next step should be ...
start pure palliative chemotherapy for metastatic disease discuss patient within MDT according to clinical presentation and determine treatment aim and clinical grouping

8
Definition of treatment strategy
The optimal strategy should be developed according to the characteristics of the patient and be discussed in the multidisciplinary team and should incorporate the (potential) view of the patient as well. Patients can be individually divided into the 4 clinical groups, by parameters describing localization, extent, and resectability of the disease, tumour dynamics, co-morbidity, potential of the patient to tolerate chemotherapy and secondary surgical treatment [IV, B].
 view of the patient as well. Patients can be individually divided into the 4 clinical groups, by parameters describing localization, extent, and resectability of the disease, tumour dynamics, co-morbidity, potential of the patient to tolerate chemotherapy and secondary surgical treatment [IV, B].")
9
Clinical groups for first line treatment stratification
clinical presentation treatment aim treatment intensity clearly R0-resectable liver and/or lung metastases cure, decrease risk of relapse nothing or moderate (FOLFOX) 1 liver and/or lung metastases only which might become resectable after induction chemotherapy ±limited/localized metastases to other sites, e.g. locoregional lymphnodes physically able to undergo major surgery (biological age, heart/lung condition) maximum tumour shrinkage upfront most active combination regimen 2 multiple metastases/sites, with rapid progression and/or tumour-related symptoms/risk of rapid deterioration co-morbidity allows intensive treatment clinically relevant tumour shrinkage as soon as possible at least achieve control of progressive disease upfront active combination: at least doublet 3 never option for resection and/or no major symptoms or risk of rapid deterioration and/or severe comorbidity (excluding from later surgery and/or intensive systemic treatment, as for groups 1+2) abrogation of further progression tumour shrinkage less relevant low toxicity most relevant treatment selection according to disease characteristics and patients preference re toxicity and efficacy: “watchful waiting” sequential approach: start with single agent, or doublet with low toxicity exceptional triplets
 1. liver and/or lung metastases only. which. might become resectable after induction chemotherapy. ±limited/localized metastases to other sites, e.g. locoregional lymphnodes. physically able to undergo major surgery (biological age, heart/lung condition) maximum tumour shrinkage. upfront most active combination regimen. 2. multiple metastases/sites, with. rapid progression and/or. tumour-related symptoms/risk of rapid deterioration. co-morbidity allows intensive treatment. clinically relevant tumour shrinkage as soon as possible. at least achieve control of progressive disease. upfront active combination: at least doublet. 3. never option for resection. and/or no major symptoms or risk of rapid deterioration. and/or severe comorbidity (excluding from later surgery and/or intensive systemic treatment, as for groups 1+2) abrogation of further progression. tumour shrinkage less relevant. low toxicity most relevant. treatment selection according to disease characteristics and patients preference re toxicity and efficacy: watchful waiting sequential approach: start with. single agent, or. doublet with low toxicity. exceptional triplets.")
10
Clinical course Patient was considered potentially curative (group 1) by MDT despite the unclear single bone lesion.
 by MDT despite the unclear single bone lesion.")
11
Acc. to ESMO guidelines primary tumor should be managed by ...
resection of primary tumor before chemotherapy upfront chemotherapy and delayed resection in case of major response (but still unresectable mets) upfront chemotherapy and resection only in case of local symptoms
 upfront chemotherapy and resection only in case of local symptoms.")
12
Clinical course primary tumor was left in situ
Potentially resectable metastatic disease after chemotherapy (group 1) For initially unresectable metastatic disease, most active available induction treatment should be chosen [V, C]. If metastases become resectable surgery for primary and metastases should be performed. Palliative surgery, stenting, laser ablation, or (chemo)radiation in case of unresectable disease, even after systemic treatment should be confined to bleeding or obstruction and as minimal invasive as possible and non invasive measures applied first [V, C].
 For initially unresectable metastatic disease, most active available induction treatment should be chosen [V, C]. If metastases become resectable surgery for primary and metastases should be performed. Palliative surgery, stenting, laser ablation, or (chemo)radiation in case of unresectable disease, even after systemic treatment should be confined to bleeding or obstruction and as minimal invasive as possible and non invasive measures applied first [V, C].")
13
Treatment algorithm for synchronous metastatic colon cancer
synchronous metastatic colon cancer with intact primary R0/R1 resectable metastases unresectable metastases single, <2cm liver met 3 months preop FOLFOX intensive upfront chemotherapy resectability achieved? yes no resection of primary and metastases (simultaneous or delayed) continue chemotherapy resectability achieved? 6 months postop FOLFOX 3 months postop FOLFOX continue initial treatment for a total of 6 months yes no surgery of primary: individual decision (e.g. complications or emergency)
 continue chemotherapy. resectability achieved 6 months postop FOLFOX. 3 months postop FOLFOX. continue initial treatment for a total of 6 months. yes. no. surgery of primary: individual decision (e.g. complications or emergency)")
14
Clinical course FOLFOX + bevacizumab
restaging after 2/4 months: partial response (RECIST) restaging after 6 months (PET/CT): liver mets: one remaining with 1.4cm (PET positive) lung lesions: complete response bone lesion: unchanged colonoscopy witout macroscopic evidence of residual primary tumor, biopsy negative (local CR) decreased tolerability with peripheral neuropathy G2 and asthenia G1
 restaging after 6 months (PET/CT): liver mets: one remaining with 1.4cm (PET positive) lung lesions: complete response. bone lesion: unchanged. colonoscopy witout macroscopic evidence of residual primary tumor, biopsy negative (local CR) decreased tolerability with peripheral neuropathy G2 and asthenia G1.")
16
Clinical course major response liver and complete response lung-metastases and primary tumor Decision was made by MDT to classify the patient as potentially curative based on age, ECOG, major response and unchanged bone lesion. However, resection or RFA of remaining central liver met. seemed technically difficult.

17
Further management? maintenance (5FU/Cape and/or bevacizumab)
complete stop of treatment consider locally ablative procedure

18
followed by complete stop of treatment
helical tomotherapy with 10x 4Gy for liver metastasis and as a precaution for the bone lesion followed by complete stop of treatment If metastases are not resectable due to their location additional measures like radiofrequency ablation or stereotactic body radiotherapy (in specialized institutions) should be considered, although the benefit is not formally proven [III, B].
 should be considered, although the benefit is not formally proven [III, B].")
19
Clinical course no evidence of disease for 10 months, followed by progressive disease with 4 new liver and disseminated pulmonary lesions, single bone lesion unchanged remaining toxicity: PNP G1 (12 months after last oxaliplatin administration)
")
20
Acc. to ESMO guidelines further treatment should be ...
restart FOLFOX + bevacizumab change to irinotecan based second line (FOLFIRI +/- targeted agent)
")
21
Reinduction reinduction FOLFOX + bevacizumab
In first line treatment patients should be treated as long as possible by restart of the former first line regimen (reinduction), when the toxicity (especially neurotoxicity) allows such reinduction. restaging after 2 months: stable disease restaging after 4 months: progressive disease (multiple new liver lesions)
, when the toxicity (especially neurotoxicity) allows such reinduction. restaging after 2 months: stable disease. restaging after 4 months: progressive disease (multiple new liver lesions)")
22
Further treatment? FOLFIRI + panitumumab
FOLFIRI/irinotecan + cetuximab FOLFIRI + bevacizumab (beyond progression - TML) FOLFIRI single agent EGFR antibody
 FOLFIRI. single agent EGFR antibody.")
23
Course of second line FOLFIRI + panitumumab
restaging after 3 months: stable disease (SLD -25%), dose reduction FOLFIRI 80% due to neutropenia restaging after 6 months: partial response (SLD -8%) side effects: asthenia G2, cutaneous tox. G1
, dose reduction FOLFIRI 80% due to neutropenia. restaging after 6 months: partial response (SLD -8%) side effects: asthenia G2, cutaneous tox. G1.")
24
Thank you

Similar presentations





 vs FOLFIRI plus bev>")



 and N+, chemotherapy should be added.>")
 Plus Bevacizumab for Patients with Unresectable.>")








: The optimal indication for operable tumors in inoperable patients D.Katsochi 1, S.Kosmidis 1, A.Fotopoulou.>")
