Download presentation
Presentation is loading. Please wait.

1
The seven sins and 10 commandments of epidemiology 18th IEA World Congress of Epidemiology, Brazil 2008: Course on Epidemiologic Research and New Directions Session Theme: Dilemmas and conundrums from epidemiologic research: have we learned the lessons? Published as Raj Bhopal. Seven mistakes and potential solutions in epidemiology, including a call for a World Council of Epidemiology and Causality. Emerging Themes in Epidemiology 2009, 6:6 Raj Bhopal CBE, DSc (hon), MD, MPH, FRCP(E) Professor of Public Health, University of Edinburgh
, MD, MPH, FRCP(E) Professor of Public Health, University of Edinburgh.")
2
Introduction: dilemmas and conundrums
Dilemmas arise when difficult choices needed to be made Conundrums are difficult questions with some twist or riddle They make us think

3
Errors, sins, virtues, commandments
Sciences make mistakes Epidemiological errors may maim and kill e.g. hormone replacement therapy Epidemiology saves lives tobacco Learn lessons

4
My 7 sins and 10 commandments
Title reflects culture on right and wrong Grandjean’s seven deadly sins of environmental epidemiology frailties of epidemiologists seven precautionary virtues (Epidemiology 2008; 19(1): )
: )")
5
Common Vices in Environmental Epidemiology and the Virtues Suggested by the Precautionary Principle,
The seven sins of Grandjean Pride Preoccupation with methodology Envy Failure to recognize achievements by others Wrath Self-righteous intimidation of competitors Lust Desire for academic honors Gluttony Excessive craving for publications Greed Benefit from vested interests Sloth Callousness to injustice

6
My chosen 7 Sins Failing to provide the context and definitions of study populations. Insufficient attention to evaluation of error. Not demonstrating comparisons are like-for-like. Either overstatement or understatement of the case for causality based on associations. Not providing both absolute and relative summary measures. In intervention studies not demonstrating general health benefits. Failure to utilise study data to benefit health.

7
Sin 1: Failing to provide the context and definitions of study populations
epidemiology is a population science populations differ by place, their characteristics and time results may not generalise timing of fieldwork is essential for time trends without the study population’s details it is not possible to draw appropriate conclusions health service/public health purposes also applies to causal research elementary epidemiology, but possibly the commonest sin

8
Examples: Fieldwork dates missing in recent reviews (no
Examples: Fieldwork dates missing in recent reviews (no. of studies on left column) 72 CV cohorts 0 0% 12 BP in UK EM groups – S. Asians 5 42% 14 BP in UK EM groups – Africans 8 57% 28 Trends in obesity in W. Africa 8 29% 21 Trends in diabetes in W. Africa 7 33%
 72 CV cohorts 0 0% 12 BP in UK EM groups – S. Asians 5 42% 14 BP in UK EM groups – Africans 8 57% 28 Trends in obesity in W. Africa 8 29% 21 Trends in diabetes in W. Africa 7 33%")
9
Ethnic composition of sample missing
No description or discussion of study in relation to ethnicity or race 72 CV cohorts 39 54% - USA 6 19% - Europe 33 80%

10
Commandments I and II for sin 1:
I. State the location and timing of fieldwork II Describe the study population in detail

11
Sin 2: Insufficient attention to evaluation of error
motivations to ignore error desiring a rapid, inexpensive and conclusive outcome rectifying errors requires scarce time and resources funding is not easy to obtain minimise external criticism achieve publication financial rewards

12
Errors: Sin 2 Possible Actions: Ignore Acknowledge
Act – qualitative interpretation (hedging) – quantitative Maldonado – no adjustment assumes study imperfections have no important impact-advocates and demonstrates quantitative adjustment of relative risk using error terms. J Epidemiol Community Health 2008; 62(7):
 – quantitative. Maldonado – no adjustment assumes study imperfections have no important impact-advocates and demonstrates quantitative adjustment of relative risk using error terms. J Epidemiol Community Health 2008; 62(7):")
13
Error: Sin 2 examples Cross-cultural validity of:
Self report (self evident but often ignored) Physical measures (BMI, waist, birth weight, growth) Clinical measures (ECG) Biochemical measures e.g. normal values of cholesterol, glucose and metabolism during OGTT
 Physical measures (BMI, waist, birth weight, growth) Clinical measures (ECG) Biochemical measures e.g. normal values of cholesterol, glucose and metabolism during OGTT.")
14
Sin 2, Commandments Sin 2, commandment III: Don’t pretend error does not exist If possible measure it If not, say so Sin 2, commandment IV: pay close attention to cross-cultural validity of all measures

15
Sin 3: Not demonstrating comparisons are like-for-like
epidemiologists study human health immense privilege but at a price experimentation is largely barred time honoured scientific principle of like-for-like comparison rarely possible sin is failing to make efforts to demonstrate comparisons are not like-for-like

16
Sin 3 example: alcohol and cardiovascular disease
Association remains (and will remain) controversial. Naimi et al compared moderate (men 2 drinks, and women 1 drink, per day) and non-drinkers. 27/30 CVD risk factors commoner in non-drinkers. Given this and confounders not included in a telephone survey - impossible to adjust for confounders? American Journal of Preventive Medicine 2005; 28(4):
 controversial. Naimi et al compared moderate (men 2 drinks, and women 1 drink, per day) and non-drinkers. 27/30 CVD risk factors commoner in non-drinkers. Given this and confounders not included in a telephone survey - impossible to adjust for confounders American Journal of Preventive Medicine 2005; 28(4):")
17
Why do trials and observational studies often contradict each other (Berkman, SER 2008 abstract 373)? Confounders Dose of exposure Group heterogeneity Period of exposure

18
Trials, observational studies and confounding
randomisation and blinding permit like-for-like comparison selection biases result-may preclude causal inference to the target population fraction of epidemiological questions are answerable using trials confounding is inevitable in other studies sin is failing to make efforts to demonstrate comparisons are not like-for-like

19
Comparing like-with-like
Sin 3, Commandment V: Start with detailed comparisons of subgroups, and don’t rely solely on one approach to control of confounding The paradox-commandment is nearly always applied in trials (not really needed)
")
20
Sin 4: Either overstatement or understatement of the case for causality based on associations
Overstatement of the case for causality is usual Counter-factual reasoning - theoretical underpinnings In practice, critical appraisal and conceptual frameworks are needed These deserve to be improved through critical research

21
Causality and design: understatement
new problem Typical statement ‘finding is not causal because the data come from a study of design x’ lazy and sloppy sin Every association places one somewhere on the pathway of causal analysis Where?-toughest question in epidemiology

22
Sin 4: Causes-examples Herbst et al 1971 case-control study on adenocarcinoma of the vagina in young woman 8 cases in girls born in N. England hospitals 1946 – 1951 (treated 1966 – 1969) and 4 controls per case Estrogen given to mothers in this pregnancy Cases 7/8 Controls 0/32 P = < (chi square) Discussion integrates epidemiology, biology and clinical medicine “… the results of this study suggest it is unwise to administer stilbestrol to women early in pregnancy.” N Engl J Med 1971; 284(15):
 and 4 controls per case. Estrogen given to mothers in this pregnancy. Cases 7/8. Controls 0/32. P = < (chi square) Discussion integrates epidemiology, biology and clinical medicine. … the results of this study suggest it is unwise to administer stilbestrol to women early in pregnancy. N Engl J Med 1971; 284(15):")
23
Causality examples (continued)
Ismail et al’s C-C study on RFs for MI 8 RFs picked out in abstract 6 had ORs ≥ 3 1 had an OR = 0.04 (0.01, 0.35) Concludes: “…While this study does not establish a cause-effect relation … it raises the possibility that several of the associated factors may be modifiable risk factors …” “Based on our findings, we suggest that stringent …” They list 6 public health actions based on their risk factors Heart 2004; 90(3):
 Concludes: …While this study does not establish a cause-effect relation … it raises the possibility that several of the associated factors may be modifiable risk factors … Based on our findings, we suggest that stringent … They list 6 public health actions based on their risk factors Heart 2004; 90(3):")
24
Causality: examples from The Society for Epidemiological Research 2008
Abstract 077 (Hughes et al) “Although causality cannot be determined from a cross-sectional study, the results suggest that increasing physical activity may be beneficial in reducing ED. (ED is erectile dysfunction) this implies causality can be determined from other designs i.e. that this design is different the inference is, in fact a causal one, albeit guarded American Journal of Epidemiology 2008; 167(suppl_11):S1-147.
 Although causality cannot be determined from a cross-sectional study, the results suggest that increasing physical activity may be beneficial in reducing ED. (ED is erectile dysfunction) this implies causality can be determined from other designs i.e. that this design is different. the inference is, in fact a causal one, albeit guarded American Journal of Epidemiology 2008; 167(suppl_11):S")
25
Causality-examples Abstract 179 (Scott et al)
Cross-sectional data from 27 countries “… I will demonstrate how to estimate the causal effects that improved water supply etc” Technical solution being sought – marginal structural models Abstract 378 (de Leon et al) Examined associations between CRP and several factors by race “Although causal inferences are not possible due to the cross-sectional nature of these data, our findings suggest the possibility that pro-inflammatory processes play a role in racial differences in health …” American Journal of Epidemiology 2008; 167(suppl_11):S1-147.
 Examined associations between CRP and several factors by race Although causal inferences are not possible due to the cross-sectional nature of these data, our findings suggest the possibility that pro-inflammatory processes play a role in racial differences in health … American Journal of Epidemiology 2008; 167(suppl_11):S")
26
Sin 4: Commandments VI and VII
VI Never say this design cannot contribute to causality or imply causality is ensured by your design VII Offer a judgement using a theoretical perspective on causality and the scientific literature

27
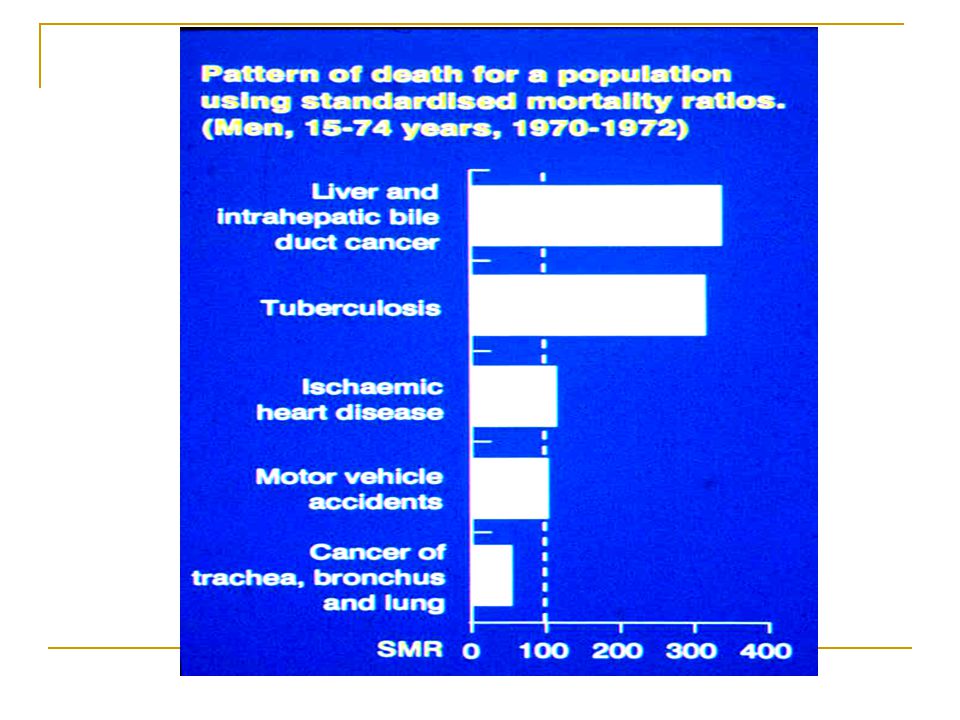
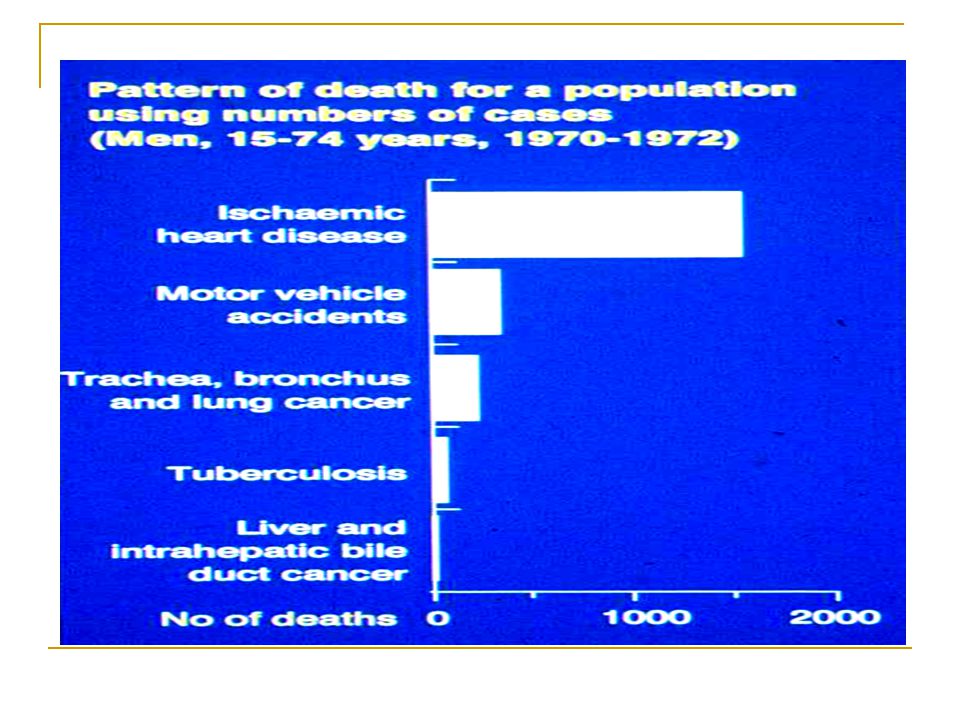
Sin 5: Not providing both absolute and relative summary measures
age and sex specific rates permit virtually everything we value highly in epidemiology summary data are distortions of this base reality do we spend time looking at such data? do we reflect on the distortions of other forms of data presentation?

30
Distortion in data presentation
Ness et al. Variants in cytokine genes among African Americans and White Americans Summary: The proinflammatory cytokine interleukin-6 (etc) genotype (IL6-IM4) was 36.5 times (8.8, 151.9) more common among African Americans Actual data Prevalence of G/G variant White women 36.3% Black women 82.5% Prevalence rate ratio = 2.27 Odds ratio = American Journal of Epidemiology 2004; 160(11):
 genotype (IL6-IM4) was 36.5 times (8.8, 151.9) more common among African Americans. Actual data. Prevalence of G/G variant White women 36.3% Black women 82.5% Prevalence rate ratio = Odds ratio = American Journal of Epidemiology 2004; 160(11):")
31
Sin 5 Commandment VIII VIII Give numbers, rates and comparative measures – rates hold primacy – and adjust ORs appropriately and utilise them carefully

32
Sin 6: In intervention studies, making recommendations without demonstrating general health benefits
Specialist’s world cardiologists and cardiovascular epidemiologists want interventions to control cardiovascular disorders no point if no net benefit specific strategies should be contributing to a common and general endeavour- longer, healthier, better life research on specific outcomes needs testing against the overall goal

33
Sin 6: examples-specific and general benefits
HRT ‘benefits’ and ‘costs’ in relation to menopausal symptoms, osteoporosis, CVD and cancer Reducing glycated haemoglobin to 6% in the elderly will improve control of diabetes, but increase mortality (N Engl J Med 2008; 358(24): ) Vit A at birth reduces mortality But not in Guinea – Bissau in Africa And, it will not be beneficial in India and Pakistan for ever, and even contested now (Benn et al, BMJ 2008; Sachder Lancet 2008; Tielsch BMJ 2008)
: ) Vit A at birth reduces mortality. But not in Guinea – Bissau in Africa. And, it will not be beneficial in India and Pakistan for ever, and even contested now (Benn et al, BMJ 2008; Sachder Lancet 2008; Tielsch BMJ 2008)")
34
Sin 6: Commandment IX IX Ensure general benefits (mortality/morbidity) exceed the general costs before recommending a public health or clinical application. Don't substitute one disease for another.
 exceed the general costs before recommending a public health or clinical application. Don t substitute one disease for another.")
35
Sin 7: Failure to interpret and utilise study data correctly to benefit health
Interpretation-intellectual endeavour in science on a par with generating worthwhile hypotheses Needs combining with practical recommendations Problems: misapplication non-application

36
Example: A Frank Statement to Cigarette Smokers
1954 advertisement in US newspapers by 14 tobacco companies and trade associations. “… experiments on mice have given wide publicity to a theory …” “… eminent doctors and research scientists have publicly questioned the claimed significance of these experiments.” “Distinguished authorities point out: That there is no agreement among the authorities regarding what the cause is “ (and 5 more points) Reprinted in The Lancet 2008;371:1645.
 Reprinted in The Lancet 2008;371:1645.")
37
Sin 7: Commandment X: World Council of Epidemiology
X Epidemiology needs connections to those who apply work e.g. politicians, doctors, public health specialists Such partners need to hear a unified voice World Council on Epidemiology needed

38
Conclusions The seven sins and 9 of the 10 Commandments-all basic in epidemiology so why do they occur? human frailties limitations of our science pressures of time and resources Strengthen human side of epidemiology Recognise innate limitations Reorganise our scientific endeavour

39
Conclusions 10th Commandment is of a different order World Council on Epidemiology unifying voice hastening advances or stultifying monster Data mining, data linkage, genetic epidemiology and large-scale epidemiology: millions of associations to come The proposal presents a dilemma, if not a conundrum

Similar presentations






. What is a cohort?>")












