Download presentation
Presentation is loading. Please wait.

1
LECTURE 5 PHARMACOLOGY DRUG ELIMINATION

2
Drug Elimination Excretion Sites of Action Absorption PLASMA
Unbound Drug PLASMA Metabolism Tissue Depots Bound Drug Excretion

3
elimination through kidneys
Drug Elimination Direct filtration & elimination through kidneys Drug Elimination Metabolism by liver to inactive product Drug Metabolism by liver to active product Active secretion by kidneys

4
elimination through kidneys
Drug Elimination Direct filtration & elimination through kidneys Drug Elimination Drug Active secretion by kidneys

5
Drug Elimination MAJOR ROUTES Minor routes of elimination Liver
Kidneys Minor routes of elimination Lungs (Volatile general anesthetics) Sweat Saliva Mother’s milk
 Sweat. Saliva. Mother’s milk.")
6
NEED FOR METABOLISM

7
KIDNEY Is Major Site of Drug Elimination
Water Soluble Filtration in Glomerulus Lipid Soluble LIVER KIDNEY Lipid soluble drugs are reabsorbed!!! Back diffusion is dependent on pH of tubular fluid & lipid solubility of drug Secretion of organic acids and bases Excretion in Urine

8
The Kidney Arterial supply Glomerulus Collecting tubule Proximal
(1.3 L/min) Glomerulus Collecting tubule Proximal tubule Distal tubule Venous return Active secretion Reabsorption Urine (1.5 L/day) e.g., gentamicin, cephalexin Loop of Henle
 Glomerulus. Collecting. tubule. Proximal. tubule. Distal. tubule. Venous. return. Active secretion. Reabsorption. Urine. (1.5 L/day) e.g., gentamicin, cephalexin. Loop of Henle.")
9
Blood Flow in the Kidney Is Important
Renal blood flow is ~25% of cardiac output 1.3 L/min Renal plasma flow is 50% of renal blood flow 650 ml/min Glomerular filtration rate (GFR) is 20% of plasma flow 130 ml/min In 24 hr, Liters are filtered by the glomerulus 24 hr urine output is Liters More than 99% of glomerular filtrate volume must be reabsorbed BUT water reabsorption does NOT equal solute reabsorption
 is 20% of plasma flow. 130 ml/min. In 24 hr, Liters are filtered by the glomerulus. 24 hr urine output is Liters. More than 99% of glomerular filtrate volume must be reabsorbed. BUT water reabsorption does NOT equal solute reabsorption.")
10
Drug Excretion in the Kidney
Two Components Glomerular filtration Passive (no energy) Clears free drug only 130 ml/min Tubular secretion Active (requires energy) Can clear % of drug flowing through kidney 650 ml/min (5X glomerular filtration)
 Clears free drug only. 130 ml/min. Tubular secretion. Active (requires energy) Can clear % of drug flowing through kidney. 650 ml/min (5X glomerular filtration)")
11
Glomerular Filtration
The Glomerulus Filters 100% of blood supply Filters everything <40 kDa Plasma & small proteins Glomerular Filtration Rate ~130 ml/min Measured by inulin or creatinine Creatinine clearance is a measure of kidney health Used to adjust drug dosage if needed Arterial supply (130 ml/min)
")
12
Tubular Secretion Energy-dependent transport (secretion)
Occurs from blood into Proximal tubule Distal tubule Loop of Henle Can clear blood of 100 of drug passing through kidney Separate transport systems for Weak organic bases (WOBs) Weak organic acids (WOAs) Most drugs and metabolites are WOAs Probenecid is a substrate for WOA transporters Its administration inhibits secretion of many drugs
 Weak organic acids (WOAs) Most drugs and metabolites are WOAs. Probenecid is a substrate for WOA transporters. Its administration inhibits secretion of many drugs.")
13
Tubular Secretion Drugs are NOT normal substrates
Drugs compete with other drugs BUT Drugs compete with endogenous metabolites In particular metabolic acids Sulfate Phosphate Glucuronate (sugar acids) Can cause electrolyte disturbances
 Can cause electrolyte disturbances.")
14
Tubular Reabsorption Mostly by passive non-ionic diffusion
Non-ionized forms of drug reabsorbed 60% in proximal tubule Uric acid (urate) is the exception (active) Acid & base forms of drugs are secreted Lipophilic (non-ionic) forms of drugs are reabsorbed Blood and urine pH affect drug elimination THEREFORE CONSEQUENTLY
 is the exception (active) Acid & base forms of drugs are secreted. Lipophilic (non-ionic) forms of drugs are reabsorbed. Blood and urine pH affect drug elimination. THEREFORE. CONSEQUENTLY.")
15
CLEARANCE A very important concept for drug use
Clearance (Cl) is the VOLUME of fluid (plasma) “cleared” (freed) of drug per unit time Clearance of most drugs is a first order process A constant fraction of drug is cleared per unit time A fraction is NOT a concentration Therefore, first order clearance is independent of drug concentration
 is the VOLUME of fluid (plasma) cleared (freed) of drug per unit time. Clearance of most drugs is a first order process. A constant fraction of drug is cleared per unit time. A fraction is NOT a concentration. Therefore, first order clearance is independent of drug concentration.")
16
CLEARANCE Clearance is independent of the method and route of clearance Hepatic clearance Renal clearance Lung (inhalational) clearance Saliva Mother’s milk
 clearance. Saliva. Mother’s milk.")
17
Therapeutic Implications of Clearance
Highly ionized drugs tend to be rapidly cleared Minimal tubular reabsorption since only non-ionized drug is reabsorbed Alkalinizing urinary pH with Na bicarbonate can accelerate clearance of WOAs Salicylate and barbiturates Acidifying urinary pH with arginine hydrochloride can accelerate clearance of WOBs Amphetamines

18
Therapeutic Implications of Clearance
Drug forms that are quite lipid soluble at the pH of the urine (5.5) are readily reabsorbed Maximal tubular reabsorption since non-ionized drug is reabsorbed Increasing osmolarity of urine (mannitol) may increase elimination of a lipophilic drug
 are readily reabsorbed. Maximal tubular reabsorption since non-ionized drug is reabsorbed. Increasing osmolarity of urine (mannitol) may increase elimination of a lipophilic drug.")
19
Therapeutic Implications of Clearance
Tubular secretion of a drug may be inhibited by another drug by competition for the transporter Probenecid competes with penicillins Thus prolongs action of antibiotic Probenecid competes with some diuretics (furosemide) and thus may prevent diuretic access to the tubule which is where they act Decreases effect of diuretic
 and thus may prevent diuretic access to the tubule which is where they act. Decreases effect of diuretic.")
20
Therapeutic Implications of Clearance
Drug clearance is decreased by renal disease Measured by creatinine clearance Caused by Decreased renal blood flow Glomerular tubular damage Tubular nephropathy Drug clearance is greater in an adult than in Children (immaturity of kidney function) Elderly (decreased renal function Alcoholics
 Elderly (decreased renal function. Alcoholics.")
21
Drug Metabolism Most metabolic products are less pharmacologically active Important exceptions: Where the metabolite is more active (Prodrugs, e.g. Erythromycin-succinate (less irritation of GI) --> Erythromycin) Where the metabolite is toxic (acetaminophen) Where the metabolite is carcinogenic Close relationship between the biotransformation of drugs and normal biochemical processes occurring in the body: Metabolism of drugs involves many pathways associated with the synthesis of endogenous substrates such as steroid hormones, cholesterol and bile acids Many of the enzymes involved in drug metabolism are principally designed for the metabolism of endogenous compounds These enzymes metabolize drugs only because the drugs resemble the natural compound
 --> Erythromycin) Where the metabolite is toxic (acetaminophen) Where the metabolite is carcinogenic. Close relationship between the biotransformation of drugs and normal biochemical processes occurring in the body: Metabolism of drugs involves many pathways associated with the synthesis of endogenous substrates such as steroid hormones, cholesterol and bile acids. Many of the enzymes involved in drug metabolism are principally designed for the metabolism of endogenous compounds. These enzymes metabolize drugs only because the drugs resemble the natural compound.")
22
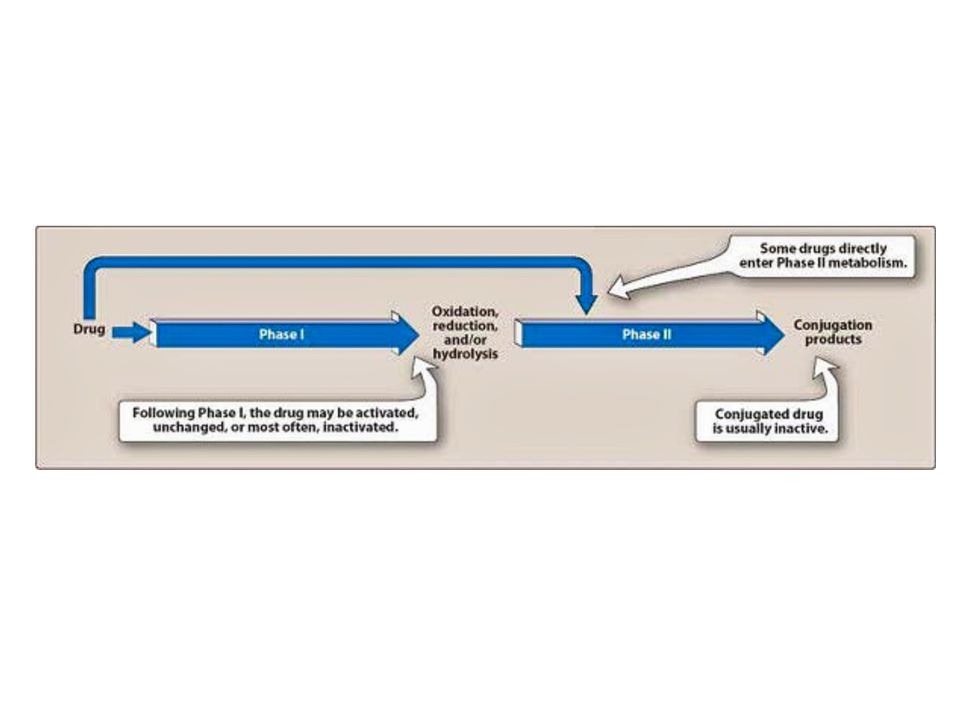
Phases of Drug Metabolism
Phase I Reactions Convert parent compound into a more polar (=hydrophilic) metabolite by adding or unmasking functional groups (-OH, -SH, -NH2, -COOH, etc.) Often these metabolites are inactive May be sufficiently polar to be excreted readily Phase II Reactions Conjugation with endogenous substrate to further increase aqueous solubility Conjugation with glucoronide, sulfate, acetate, amino acid Phase I usually precede phase II reactions Liver is principal site of drug metabolism: Other sites include the gut, lungs, skin and kidneys For orally administered compounds, there is the “First Pass Effect” Intestinal metabolism Liver metabolism Enterohepatic recycling Gut microorganisms - glucuronidases
 metabolite by adding or unmasking functional groups (-OH, -SH, -NH2, -COOH, etc.) Often these metabolites are inactive. May be sufficiently polar to be excreted readily. Phase II Reactions. Conjugation with endogenous substrate to further increase aqueous solubility. Conjugation with glucoronide, sulfate, acetate, amino acid. Phase I usually precede phase II reactions. Liver is principal site of drug metabolism: Other sites include the gut, lungs, skin and kidneys. For orally administered compounds, there is the. First Pass Effect Intestinal metabolism. Liver metabolism. Enterohepatic recycling. Gut microorganisms - glucuronidases.")
23
Drug Metabolism - Phase I
Phase I Reactions Oxidation Reduction Hydrolytic cleavage Alkylation (Methylation) Dealkylation Ring cyclization N-carboxylation Dimerization Transamidation Isomerization Decarboxylation
 Dealkylation. Ring cyclization. N-carboxylation. Dimerization. Transamidation. Isomerization. Decarboxylation.")
24
Drug Metabolism - Oxidation
Two types of oxidation reactions: Oxygen is incorporated into the drug molecule (e.g. hydroxylation) Oxidation causes the loss of part of the drug molecule (e.g. oxidative deimination, dealkylation) Microsomal Mixed Function Oxidases (MFOs) “Microsomes” form in vitro after cell homogenization and fractionation of ER Rough microsomes are primarily associated with protein synthesis Smooth microsomes contain a class of oxidative enzymes called “Mixed Function Oxidases” or “Monooxygenases” These enzymes require a reducing agent (NADPH) and molecular oxygen (one oxygen atom appearing in the product and the other in the form of water)
 Oxidation causes the loss of part of the drug molecule. (e.g. oxidative deimination, dealkylation) Microsomal Mixed Function Oxidases (MFOs) Microsomes form in vitro after cell homogenization and fractionation of ER. Rough microsomes are primarily associated with protein synthesis. Smooth microsomes contain a class of oxidative enzymes called. Mixed Function Oxidases or Monooxygenases These enzymes require a reducing agent (NADPH) and molecular oxygen. (one oxygen atom appearing in the product and the other in the form of water)")
25
Drug Metabolism - Oxidation
MFO consists of two enzymes: Flavoprotein, NADPH-cytochrome c reductase One mole of this enzyme contains one mole each of flavin mononucleotide (FMN) and flavin adenine dinucleotide (FAD) Enzyme is also called NADPH-cytochrome P450 reductase Cytochrome P450 named based on its light absorption at 450 nm when complexed with carbon monoxide is a hemoprotein containing an iron atom which can alternate between the ferrous (Fe++) and ferric (Fe+++) states Electron acceptor Serves as terminal oxidase its relative abundance compared to NADPH-cytochrome P450 reductase makes it the rate-limiting step in the oxidation reactions
 and flavin adenine dinucleotide (FAD) Enzyme is also called NADPH-cytochrome P450 reductase. Cytochrome P450. named based on its light absorption at 450 nm when complexed with carbon monoxide. is a hemoprotein containing an iron atom which can alternate between the ferrous (Fe++) and ferric (Fe+++) states. Electron acceptor. Serves as terminal oxidase. its relative abundance compared to NADPH-cytochrome P450 reductase makes it the rate-limiting step in the oxidation reactions.")
26
Cytochrome P450 At least 57 different isozymes in humans, over 7700 forms in Nature isozyme-catalytically and structurally similar but genetically distinct enzymes-different genes and amino acid sequences Different isozymes have different substrate specificities Individuals have several alleles for P450’s and differ in which isozymes they have Since individuals have different combinations of P450’s, they differ in their response to specific drugs A subset of cytochrome P450’s can be induced, so that more is expressed upon exposure to a compound. Because of the number of different isozymes and their different substrates and inhibitors, the metabolism of a drug can be altered if an individual takes a second drug.

27
Some substrates of cytochrome P450 isozymes

28
Drug Metabolism - Phase II
Conjugation reactions Glucuronidation by UDP-Glucuronosyltransferase: (on -OH, -COOH, -NH2, -SH groups) Sulfation by Sulfotransferase: (on -NH2, -SO2NH2, -OH groups) Acetylation by acetyltransferase: Amino acid conjugation (on -COOH groups) Glutathione conjugation by Glutathione-S-transferase: (to epoxides or organic halides) Fatty acid conjugation (on -OH groups) Condensation reactions
 Sulfation by Sulfotransferase: (on -NH2, -SO2NH2, -OH groups) Acetylation by acetyltransferase: Amino acid conjugation. (on -COOH groups) Glutathione conjugation by Glutathione-S-transferase: (to epoxides or organic halides) Fatty acid conjugation. (on -OH groups) Condensation reactions.")
29
Drug Metabolism - Glucuronidation
Glucuronidation ( = conjugation to a-d-glucuronic acid) Quantitatively the most important phase II pathway for drugs and endogenous compounds Products are often excreted in the bile. Enterohepatic recycling may occur due to gut glucuronidases Requires enzyme UDP-glucuronosyltransferase (UGT): Genetic family of enzymes Metabolizes a broad range of structurally diverse endogenous and exogenous compounds Structurally related family with approximately 16 isoforms in man
 Quantitatively the most important phase II pathway for drugs and endogenous compounds. Products are often excreted in the bile. Enterohepatic recycling may occur due to gut glucuronidases. Requires enzyme UDP-glucuronosyltransferase (UGT): Genetic family of enzymes. Metabolizes a broad range of structurally diverse endogenous and exogenous compounds. Structurally related family with approximately 16 isoforms in man.")
30
Drug Metabolism - Glucuronidation
Glucuronidation – requires creation of high energy intermediate: UDP-Glucuronic Acid:

32
NEXT LECTURE AUTONOMIC NERVOUS SYSTEM APPLIED PHARMACOLOGY

33
THANK YOU

Similar presentations





 Absorption Distribution Metabolism Excretion Toxicology.>")
 that alter the pharmacological activity of both endogenous and exogenous compounds.>")

 - but the body is not homogeneous. Factors.>")
 : metabolism of a drug.>")









