Download presentation
Presentation is loading. Please wait.

1
Principles of Cardiac Arrest Management
Richard Lake 10/2003

2
Background Information
40% of deaths under the age of 75yrs in Europe are due to cardiovascular disease One third of people who suffer a myocardial infarction die before reaching hospital Most die within an hour of the onset of acute symptoms The majority of these deaths the presenting rhythm is Ventricular Fibrillation or pulseless Ventricular Tachycardia, (VF/ pulseless VT)
")
3
The only treatment for VF/ pulseless VT is attempted defibrillation
With each minute’s delay the chance of a successful outcome fall by 7-10% Once in hospital the incidence of VF after Myocardial Infraction is approximately 5% Most likely presentation of in hospital cardiac arrest is asystole or pulseless electrical activity (PEA).
.")
4
The Chain of Survival

5
Early Access to emergency services or cardiac arrest team
Out of hospital summon EMS by dialling 999/112 In hospital call cardiac arrest team ring 2222 (check number when on placement)
")
6
External chest compressions and
ventilation will slow down the rate of deterioration of the brain and heart Basic Life Support should be performed immediately

7
Basic Life Support Danger Response Shout for Help Airway Breathing
If no help arrived leave victim, go for help Circulation

8
Danger Check for danger to: Yourself Bystanders Victim
Even clinical areas can have dangers, so ALWAYS CHECK

9
Response Check the victim for response
Ask a question, ‘hello are you alright?’ Give a command, ‘open your eyes!’ Give a painful stimulus; pinch the shoulder If no response shout for help

10
Checking for response

11
Airway Check the airway
Open the airway, place one hand on the victims forehead and gently tilt head back Remove any visible obstruction from the victims mouth, including dislodged dentures. Leave well fitting dentures in place DO NOT ATTEMPT ANY FINGER SWEEPS

12
Opening the airway

13
Jaw thrust technique may be needed if C-spine injury

15
If available use airway adjuncts

16
Nasopharyngeal airway insertion

19
Oropharyngeal airway insertion

20
Breathing Keeping the airway open: Look – for chest movements
Listen – at the victims mouth for breath sounds Feel – for air on your cheek Look, listen and feel for no more than 10 seconds to determine if the victim is not breathing.

21
If not breathing and no help has arrived
Leave the victim and go to summon help

22
Turn the victim onto his back if he is not already in that position
Give 2 effective rescue breaths, each of which should make the chest rise and fall If you have difficulty achieving an effective breath: Recheck the victims mouth and remove any obstruction Recheck there is head tilt and chin lift Make up to 5 attempts to achieve 2 effective breaths Even if unsuccessful move onto check circulation

24
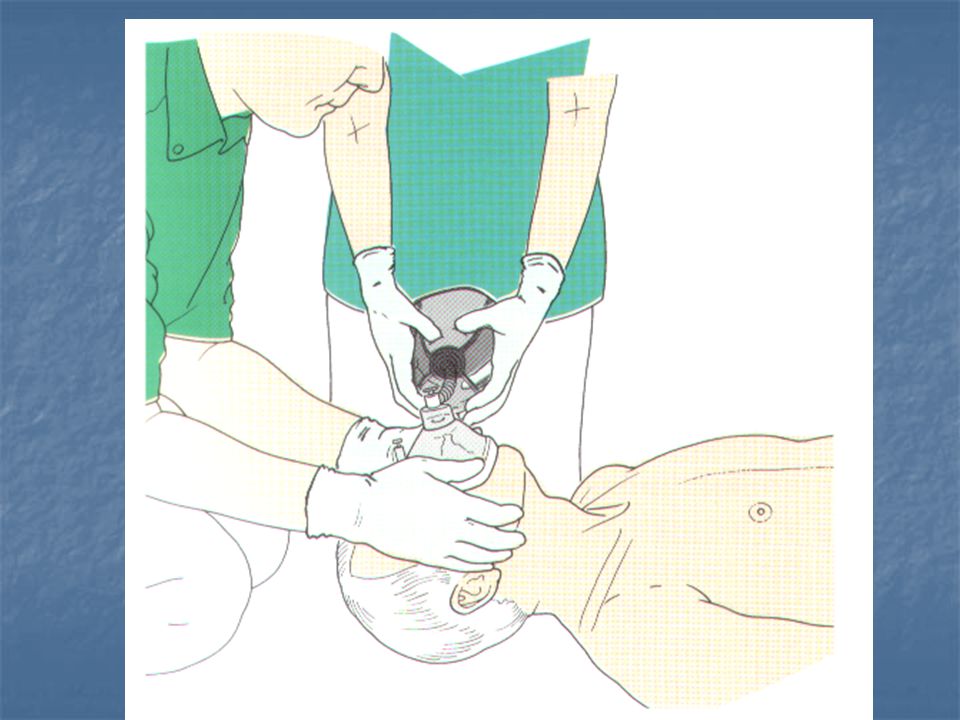
If available use a pocket mask

26
Bag valve mask device may be used

28
Circulation Look, listen and feel for normal breathing, coughing, swallowing, eye flickering, or any movement by the victim If you feel confident check for a carotid pulse You should take no more than 10 seconds to do this

29
Always check pulse same side as you

30
If no breathing but signs of circulation
Continue rescue breaths at a rate of 10 breaths per minute After every 10 breaths (every 1 minute) recheck for signs of circulation This should take no longer than 10 seconds to check
 recheck for signs of circulation. This should take no longer than 10 seconds to check.")
31
If no breathing and no signs of circulation
Commence CPR at a ratio of 15 Compressions to 2 ventilations

32
Ensure correct hand position

34
The Chain of Survival

35
Out of hospital the aim is to
deliver a shock within 5 minutes of the EMS receiving a call In hospital the first healthcare responder should be trained and authorised to use a defibrillator immediately

36
Automated External Defibrillator

37
AED hands off pads

38
Automated External Defibrillators may be used

40
Manual Defibrillator

41
Manual Defibrillator Paddles

42
Defibrillation

43
Defibrillation should be performed promptly

44
Often defibrillation restores a
perfusing heart rhythm, this is often inadequate to sustain circulation and further advanced life support is required to improve the chances of long term survival

45
Remember the chain of survival

46
The Universal Treatment Algorithm
An important part of Advanced Cardiac Life Support

47
Objectives Recognise the four cardiac arrest rhythms
Identify correctly the appropriate algorithm for each of the rhythms Discuss the potential reversible causes of cardiac arrest

48
Re-assess one minute after defibrillation
BLS Algorithm if appropriate Precordial Thump Attach Monitor/Defib Assess rhythm +/- Pulse Check VF / VT NON VF/VT DEFIB X 3 as necessary During CPR Correct reversible causes CPR 3 min Re-assess one minute after defibrillation CPR 1 MIN Check electrode / paddle positions Attempt/verify airway/02/IV access Give adrenaline every 3 mins ? buffers/atropine/ pacing/antiarrhythmics

49
? VF / VT Non VF / VT BLS Algorithm Precordial Thump
if appropriate Precordial Thump if appropriate Attach Monitor/Defib Assess rhythm +/- Pulse Check ? VF / VT Non VF / VT

50
During CPR Correct reversible causes
BLS Algorithm if appropriate Precordial Thump Attach Monitor/Defib Assess rhythm +/- Pulse Check VF / VT During CPR Correct reversible causes DEFIB X 3 as necessary Check electrode / paddle positions Attempt/verify airway/02/IV access Give adrenaline every 3 mins ? buffers/atropine/ pacing/antiarrhythmics CPR 1 MIN

51
During CPR Correct reversible causes
BLS Algorithm if appropriate Precordial Thump Attach Monitor/Defib Assess rhythm +/- Pulse Check NON VF/VT During CPR Correct reversible causes CPR 3 min Re-assess one minute after defibrillation Check electrode / paddle positions Attempt/verify airway/02/IV access Give adrenaline every 3 mins ? buffers/atropine/ pacing/antiarrhythmics

52
Potentially Reversible Causes
Hypoxia Hypovolemia Hyper/ Hypokalemia and metabolic disturbances Hypothermia Tension pneumothorax Tamponade Toxic/ therapeutic disturbances Thrombo-embolic/ mechanical obstruction

53
Re-assess one minute after defibrillation
BLS Algorithm if appropriate Precordial Thump Attach Monitor/Defib Assess rhythm +/- Pulse Check VF / VT NON VF/VT DEFIB X 3 as necessary During CPR Correct reversible causes CPR 3 min Re-assess one minute after defibrillation CPR 1 MIN Check electrode / paddle positions Attempt/verify airway/02/IV access Give adrenaline every 3 mins ? buffers/atropine/ pacing/antiarrhythmics

58
Drugs used commonly during resuscitation
Epinephrine (Adrenaline) Atropine Amiodarone Magnesium Sulphate Lidocaine (Lignocaine) Sodium Bicarbonate Calcium
 Atropine. Amiodarone. Magnesium Sulphate. Lidocaine (Lignocaine) Sodium Bicarbonate. Calcium.")
59
Epinephrine (Adrenaline)
First line cardiac arrest drug, given after every 3 minutes of CPR Dose 1mg (10ml of 1 in 10,000) IV Causes vasoconstriction, increased systemic vascular resistance increasing cerebral and coronary perfusion Increases myocardial excitability, when the myocardium is hypoxic or ischaemic
 IV. Causes vasoconstriction, increased systemic vascular resistance increasing cerebral and coronary perfusion. Increases myocardial excitability, when the myocardium is hypoxic or ischaemic.")
60
Atropine Given for asystole or pulseless electrical activity with a rate less than 60 beats per minute 3mg is given as a single intravenous dose It blocks the activity of the vagus nerve on the SA and AV nodes, increasing sinus automaticity and facilitating AV node conduction

61
Amiodarone For Refractory VF/VT; haemodynamically stable VT and other resistant tachyarrhythmias If VF or pulseless VT persists after the first 3 shocks then Amiodarone 300mg is considered. If not pre-diluted, must be diluted in 5% dextrose to 20ml. (Will crystallise is mixed with saline) Should be given centrally but in an emergency can be given peripherally Increases the duration of the action potential in the atrial and ventricular myocardium
 Should be given centrally but in an emergency can be given peripherally. Increases the duration of the action potential in the atrial and ventricular myocardium.")
62
Magnesium Sulphate For refractory VF when hypomagnesaemia is possible; ventricular tachyarrhythmias when hypomagnesaemia is possible In refractory VF – 1 to 2g (2-4ml of 50% magnesium sulphate) peripherally over 1 to 2 minutes. Other circumstances 2.5g (5ml of 50% magnesium sulphate) over 30 minutes
 peripherally over 1 to 2 minutes. Other circumstances 2.5g (5ml of 50% magnesium sulphate) over 30 minutes.")
63
Lidocaine (Lignocaine)
For Refractory VF/ pulseless VT (when Amiodarone is unavailable 100mg for VF/ pulseless VT that persists after three shocks. Another 50mg can be given if necessary

64
Sodium Bicarbonate Given for severe metabolic acidosis and Hyperkalaemia 50mmol (50ml of 8.4% solution), where there is an acidosis or cardiac arrest associated with Hyperkalaemia
, where there is an acidosis or cardiac arrest associated with Hyperkalaemia.")
65
Calcium Administered when pulseless electrical activity caused by:
Hyperkalaemia Hypocalcaemia Overdose of Calcium channel blocking drugs Dose 10ml of 10% calcium chloride repeated according to blood results

66
Summary Cardiac arrest can have a variety of causes
The chain of survival is essential to improve outcome from cardiac arrest

67
Awareness of the universal treatment algorithm is important
A knowledge of the drugs used in cardiac arrest, their routes and dilution is also essential

68
Questions

69
References Resuscitation Council (UK). (2000) Advanced Life Support Provider Course Manual . 4th Edition. Resuscitation Council (UK).:London Resuscitation Council (UK). (2002) Immediate Life Support Course Manual . 1st Edition. Resuscitation Council (UK).:London
. (2002) Immediate Life Support Course Manual . 1st Edition. Resuscitation Council (UK).:London.")
Similar presentations























.>")


>")


