Download presentation
Presentation is loading. Please wait.

1
The role of radiation in the management of acromegaly
Current concepts and controversies

2
Axial and Coronal MRI

3
Radiological Anatomy Coronal section showing optic chiasm

4
MRI Anatomy

5
Functional imaging withGallium Dotatate

6
Coronal section demonstrating proximity to optic chiasm

7
Stem Cell regions

8
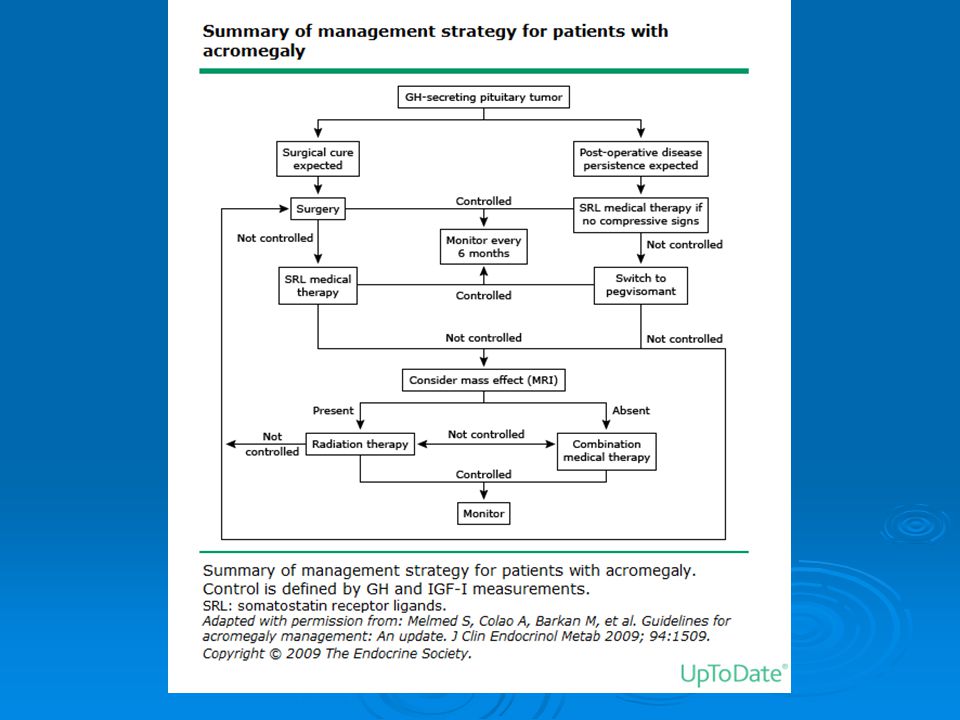
Management of Acromegaly
Surgery Radiation therapy Medical Therapy

10
Surgery Generally first line therapy
Indicated for active acromegaly, visual loss, pituitary tumour apoplexy, mass effect and treatment of progressive or refractory disease Transsphenoidal Endoscopic transsphenoidal Craniotomy

11
Surgical Results Goal of management is restoration of a normal GH secretion profile and normalisation of IGF-1 70-88% long term control in microadenomas 50-61% long term control in macroadenomas Recurrence more likely with invasive tumours

12
Surgical complications
Low mortality <0.5% CSF leak and meningitis Vascular injury <1% Sinusitis Diabetes insipidus ; transient 3% pemanent <2% Visual loss in 5% New hypopituitarism in 10-20%

13
Multimodality therapy
Indicated in residual or recurrent adenomas 75% are macroadenomas at diagnosis and often invade surrounding structures such as bone or dura rendering complete safe resection unfeasible Between 10-50% will have persistent elevations of IGF-1 and GH Up to 20% can recur in spite of normalisation of hormone levels

14
Multimodality Therapy
Following incomplete resection or recurrence radiation therapy and medical therapy either in a combined or sequential fashion can be used The aim is to achieve normalisation of GH and IGF-1 levels Therapy is best considered in a multi-disciplinary team evluating the most effective and least risky therapy for each patient on an individual basis

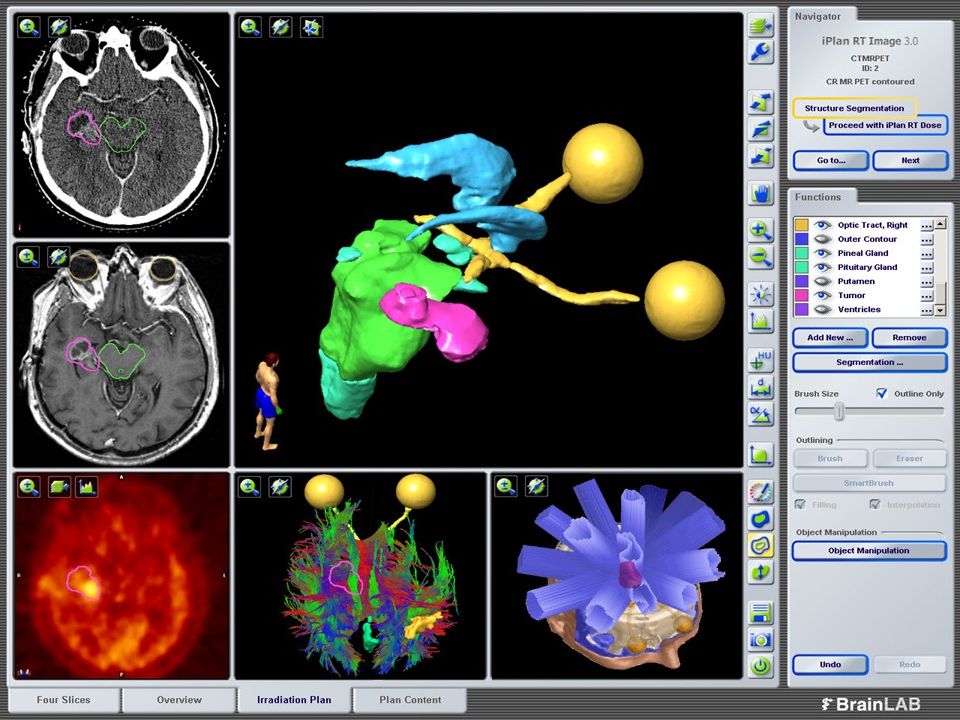
15
Stereotactic Radiation
From the Greek stereos solid, taxis form or order 3 dimensional localisation of objects with Cartesian coordinates Two major divisions, Radiosurgery ; the delivery of a single large dose and Radiotherapy ; the delivery of multiple smaller doses Benefits must always be balanced against inherent risks of new hypopituitarism, visual loss and cranial nerve deficits

16
Conventional External beam Radiotherapy(EBRT)
Old technology Has been used since the 1920’s, not much planning involved and large volumes of normal tissues irradiated

17
EBRT

18
EBRT Widely varying reported rates of effectiveness 5-74% hormonal remission, variation probably due to levels defining remission Functional response can take 5-15 years to manifest 50-80% risk of new hypopituitarism Increased stroke risk EBRT use has thus significantly dropped in the last decade

19
Complications of EBRT Low risk of radiation cerebral damage at doses<50 Gy at 2Gy/#, radionecrosis <1% Optic neuropathy at this dose schedule occurs at approximately 1-5% New hypopituitarism in up to 60% Increased incidence of stroke has been demonstrated with a 1.6 fold excess Radiation induced second tumours in 2% at 10 years and 2.4% at 20 years Possible mild cognitive impairment with older techniques

20
Stereotactic Radiosurgery
Gamma Knife Cyber Knife Linac Based Can be frame based Recent use of Image guided Radiotherapy IGRT with on-line cone beam CT scan in a linear accelerator(Linac)
")
21
Frame for Gamma Knife

22
Gamma Knife

23
Cyber Knife

24
Radiosurgery Single dose to a mean marginal dose of 14-34 Gy
Can only be used if the adenoma is at least 3-5mm away from the optic chiasm or optic nerves Tolerance dose of optic chiasm is 8Gy after which there is a significant risk of blindness in both eyes

25
Coronal section on Gamma Plan

26
Gamma Plan

27
Radiosurgery Stable or reduced tumour volume is achieved in 97% of patients Normalisation of IGF-1 and GH levels is achieved in17-96%, this variation is probably due to varying doses, length of follow up and thresholds for defining remission A large meta-analysis demonstrated remission in approximately 50% , overall control +/- medical therapy was 73% Median time to remission was 29.8 months

28
Radiosurgery The smaller the adenoma and the lower the IGF-1 and GH levels the more likely remission is to be attained Prior or concurrent use of Octreotide may decrease the effectiveness of radiosurgery People treated with radiosurgery require close follow up due to the long latency of remission, risks of late relapse and potential late side effects

29
Complications of Radiosurgery
New hypopituiarism, 2-47% Visual disturbances, 1-11% Cranial nerve damage, rare Temporal lobe epilepsy Radiation Necrosis Carotid artery stenosis The larger the volume of tumour and the closer it is to the optic nerves the greater the risk of complications

30
Fractionated Stereotactic Radiotherapy (f-SRT)
In recent years the advent of frameless, high precision reproducibly accurate systems with <1mm variation using image guidance(IGRT) has allowed far more localised radiation delivery This reduces the volume of normal tissue irradiated A recent study delivering 54Gy in treatments demonstrated stable or reduced volume in 91% 50% achieved biochemical control within 30 months of those 30%had complete remission and came off all medical therapy, none of this group showed late relapse
 has allowed far more localised radiation delivery. This reduces the volume of normal tissue irradiated. A recent study delivering 54Gy in treatments demonstrated stable or reduced volume in 91% 50% achieved biochemical control within 30 months of those 30%had complete remission and came off all medical therapy, none of this group showed late relapse.")
32
Comparison of frame based with Image guided Radiotherapy

33
Immobilisation using a bite block and a thermoplastic mask

34
Bite block

35
Thermoplastic Mask alone

36
Schematic Dose distribution

37
f-SRT In those who had one or more functional pituitary axes prior to f-SRT 29% developed further hypopituitarism at 48 months In people who had hypopituitarism prior to therapy 21% developed a defficiency in a new axis Overall 50% demonstrated biochemical control 91% demonstrated tumour control at a median of 34 months 55% showed tumour regression

38
f-SRT Low rates of toxicity have been demonstrated with high rates of durable control Recent studies have shown 5 year tumour control rates of 100% and hormonal control rates of 80% Optic neuropathy occurs in 1-5% of cases Overall hypopituitarism rates vary from 15-37% No cases of CVA have been recorded although this may be due to the fact that f-SRT has not been used for long and stroke is a late effect Possibly less cognitive impairment than EBRT , requires validation

40
Advanced techniques in f-SRT
IMRT( Intensity modulated radiation therapy) shapes and modulates the beam to allow far higher target conformity whilst minimising radiation dose to adjacent normal tissue especially sensitive structures. This may take10-12 minutes to deliver VMAT(volumetric Modulated Arc Therapy) is a more refined form of IMRT capable of greater conformality and sparing of critical structures in certain settings. Treatment takes 70 seconds
 shapes and modulates the beam to allow far higher target conformity whilst minimising radiation dose to adjacent normal tissue especially sensitive structures. This may take10-12 minutes to deliver. VMAT(volumetric Modulated Arc Therapy) is a more refined form of IMRT capable of greater conformality and sparing of critical structures in certain settings. Treatment takes 70 seconds.")
41
Advanced f-SRT Image guided radiation therapy(IGRT)
This may be combined with IMRT or VMAT Micro Multileaf Collimators (mMLC) available from a number of vendors; Elekta particularly the Agility or the Apex collimator, Brain Lab including Novalis , Varian particularly True Beam May also be delivered by cone collimation available from a number of vendors including the aforementioned and Radionics. These are not capable of beam modulation as are the mMLC devices and may not be able to spare adjacent structures as well particularly if they are close by
 available from a number of vendors; Elekta particularly the Agility or the Apex collimator, Brain Lab including Novalis , Varian particularly True Beam. May also be delivered by cone collimation available from a number of vendors including the aforementioned and Radionics. These are not capable of beam modulation as are the mMLC devices and may not be able to spare adjacent structures as well particularly if they are close by.")
42
Micro Multi Leaf Collimator m-MLC

43
Conclusion Radiotherapy is very effective in the management of recurrent or persistent active acromegaly following surgery Conventional EBRT achieves biochemical remission in 50-60% with a reasonable risk of complications Stereotactic Therapy SRS or f-SRT provide comparable high rates of tumour control and hormonal remission with low morbidity risks. Possibly reduce late toxicities to normal tissue

44
Conclusion Tumour characteristics particularly size, proximity to optic chiasm or cavernous sinus and dural involvement are particularly important in deciding between SRS and f-SRT. For small tumours >3mm away from the chiasm SRS is a convenient option For larger tumours close to critical structures f-SRT is an option with equivalent control rates but lower morbidity Research into other fractionation schedules involving a smaller number of higher dose fractions (HIGRT) is ongoing
 is ongoing.")
Similar presentations















: The optimal indication for operable tumors in inoperable patients D.Katsochi 1, S.Kosmidis 1, A.Fotopoulou.>")




