Download presentation
Presentation is loading. Please wait.

1
Alcohol Interventions: What the research tells us Professor Colin Drummond

3
Alcohol use disorders: prevalence Drummond et al., 2005 26% of the adult population have an alcohol use disorder (AUD) Includes 38% of men & 16% of women aged 16-64 23% of the adult population are hazardous or harmful alcohol users (7.1 million people in England) 21% of men and 9% of women engage in binge drinking Prevalence of alcohol dependence is 3.6% overall, 6% among men, and 2% among women (1.1 million people in England) Alcohol Needs Assessment Research Project, 2005 Alcohol dependence is considerably more prevalent than drug abuse
 Includes 38% of men & 16% of women aged % of the adult population are hazardous or harmful alcohol users (7.1 million people in England) 21% of men and 9% of women engage in binge drinking Prevalence of alcohol dependence is 3.6% overall, 6% among men, and 2% among women (1.1 million people in England) Alcohol Needs Assessment Research Project, 2005 Alcohol dependence is considerably more prevalent than drug abuse")
4
“The habit of drunkenness is a disease of the mind”

8
NICE Guidance 2010-11 Alcohol use disorders – Preventing harmful drinking (PH24) – Diagnosis and clinical management of alcohol related physical complications (CG100) – Diagnosis, assessment and management of harmful drinking and alcohol dependence (CG) Related guidance – Psychiatric comorbidity (CG) – Complex pregnancies (CG)
 – Diagnosis and clinical management of alcohol related physical complications (CG100) – Diagnosis, assessment and management of harmful drinking and alcohol dependence (CG) Related guidance – Psychiatric comorbidity (CG) – Complex pregnancies (CG)")
9
NICE Guidance 2010-11 Alcohol use disorders – Preventing harmful drinking (PH24) – Diagnosis and clinical management of alcohol related physical complications (CG100) – Diagnosis, assessment and management of harmful drinking and alcohol dependence (CG) Related guidance – Psychiatric comorbidity (CG) – Complex pregnancies (CG)
 – Diagnosis and clinical management of alcohol related physical complications (CG100) – Diagnosis, assessment and management of harmful drinking and alcohol dependence (CG) Related guidance – Psychiatric comorbidity (CG) – Complex pregnancies (CG)")
10
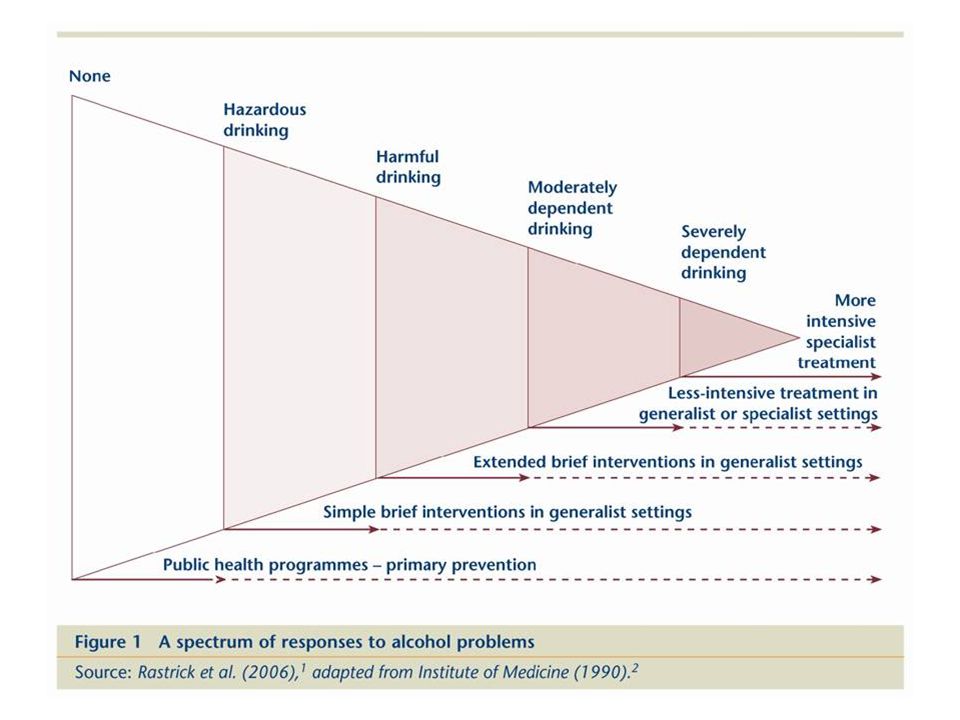
Preventing harmful drinking – evidence relevant to interventions AUDIT high sensitivity and specificity Laboratory markers poor screening tools Brief interventions effective (27 systematic reviews) Brief advice as effective as extended brief intervention ~ brief more cost effective Brief interventions less effective in alcohol dependence than hazardous/harmful drinkers Most evidence in primary care, limited for acute care & CJS settings
 Brief advice as effective as extended brief intervention ~ brief more cost effective Brief interventions less effective in alcohol dependence than hazardous/harmful drinkers Most evidence in primary care, limited for acute care & CJS settings")
11
Preventing harmful drinking (PH24) All NHS professionals and non-NHS Routine alcohol screening – Universal – Targeted “if not feasible” Validated screening tool (AUDIT, FAST etc) Don’t use biological markers Structured brief advice- all hazardous/harmful Extended brief- non-responders Referral of moderate/severe alcohol dependence/non-responders to brief interventions
 All NHS professionals and non-NHS Routine alcohol screening – Universal – Targeted if not feasible Validated screening tool (AUDIT, FAST etc) Don’t use biological markers Structured brief advice- all hazardous/harmful Extended brief- non-responders Referral of moderate/severe alcohol dependence/non-responders to brief interventions")
12
Clinical management Unplanned withdrawal: – Admit high risk, vulnerable and under 16s – Symptom triggered regime more cost effective – Benzodiazepine or carbamazepine – CIWA monitoring Wernicke’s encephalopathy – Oral thiamine for most – Parenteral for malnourished, liver disease and in AED or admitted for acute illness or injury

13
Management of harmful drinking and alcohol dependence Identification and assessment Care coordination Settings Assisted withdrawal Psychosocial interventions Pharmacological interventions Comorbidity Children and young people

14
Identification and assessment Competence Motivational interviewing Alcohol misuse, dependence, problems, risk, need for assisted withdrawal Formal assessment tools (AUDIT, SADQ, LDQ, APQ, CIWA, MMSE) Treatment goals Children and young people
 Treatment goals Children and young people")
15
Care pathway – case identification and possible diagnosis for adults Screen (PAT, FAST, SASQ etc.) indicates possible alcohol use disorder Administer: AUDIT AUDIT < 8 AUDIT 16–19 Harmful drinking AUDIT 8–15 Hazardous drinking AUDIT 20+ Probable alcohol dependence Referral to specialist assessment/withdraw al assessment Referral to specialist assessment where no improve maintained Extended brief intervention(s) Review of progress Consider Tier 2 interventions Consider Tier 2 or 3 interventions/ immediate withdrawal assessment for acute inpatients settings and prisons Brief intervention
 indicates possible alcohol use disorder Administer: AUDIT AUDIT < 8 AUDIT 16–19 Harmful drinking AUDIT 8–15 Hazardous drinking AUDIT 20+ Probable alcohol dependence Referral to specialist assessment/withdraw al assessment Referral to specialist assessment where no improve maintained Extended brief intervention(s) Review of progress Consider Tier 2 interventions Consider Tier 2 or 3 interventions/ immediate withdrawal assessment for acute inpatients settings and prisons Brief intervention")
16
Interventions: delivery and setting Competence, manuals, supervision Care coordination Case management – alcohol dependence Stepped care and ACT Inpatient withdrawal management Structured intensive community programme – Moderate severe dependence, social support, complex needs Residential rehabilitation – Moderate severe dependence AND homeless – 3 months

17
Interventions Harmful/mild dependence – CBT, BT, Social Network therapy – BCT – Non-responders: offer acamprosate, naltrexone plus psychosocial Moderate/severe dependence – Assisted withdrawal – Intensive community programme – Acamprosate or naltrexone plus – CBT, BT, SNT, BCT – Disulfiram (second line, suitability/preference) Children and young people under 18 – Inpatient for withdrawal – CBT, multi-component programmes – Acamprosate or naltrexone (second line 16-18 only) Families and carers – Assessment and intervention in their own right
 Children and young people under 18 – Inpatient for withdrawal – CBT, multi-component programmes – Acamprosate or naltrexone (second line only) Families and carers – Assessment and intervention in their own right")
18
Association between baseline severity and effect size in naltrexone versus placebo trials (logRR)
")
19
Assisted withdrawal Threshold for assessment: >20 AUDIT >15 units/day Community based withdrawal programme - most Inpatient assisted withdrawal – >30 SADQ, fits or DTs – OR 15-30 plus benzodiazepine, mental or physical comorbidity, learning disability, cognitive impairment – Lower threshold for homeless, older, younger, pregnancy, homeless Regimes – Community: fixed dose – Inpatient: fixed dose or symptom triggered

20
AUDIT > 20 Consider need for alcohol withdrawal Outcome of assessment SADQ < 15 Typical drinks per day < 15 SADQ 15–30 Typical drinks per day < 30 units Absence of comorbid features SADQ ≥ 30 Typical drinks per day ≥ 30 units Comorbid features present Consider Tier 2 or 3 interventions: Psychological and pharmacological interventions Comprehensive assessment where comorbid features present Outpatient (Tier 3 interventions): Assisted alcohol withdrawal Inpatient (Tier 4 interventions): Assisted alcohol withdrawal AUDIT < 20 AUDIT
: Assisted alcohol withdrawal Inpatient (Tier 4 interventions): Assisted alcohol withdrawal AUDIT < 20 AUDIT")
22
Gap between need and access (PSUR) by region
 by region")
Similar presentations






 Public Health Alcohol: Its Impact & Address.>")




 in Berkshire Community Partnership Forum February 2014 Sally Murray Head of Children’s Commissioning.>")








