Download presentation
Presentation is loading. Please wait.

1
Arrhythmias Danny Haywood FY1

2
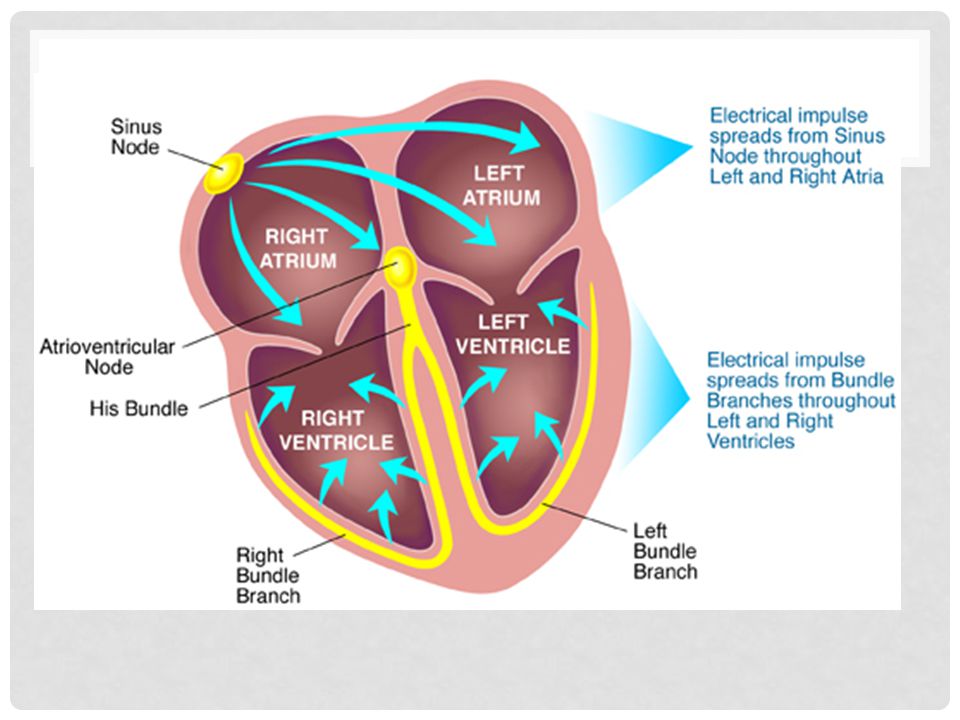
Intro Conduction system of heart Symptoms/signs Investigations
Tachy vs Brady Bradyarrhythmias Different types Management Tachyarrhythmias Broad vs narrow Types of each Management of each Summary Some example ECGs

4
Symptoms/signs Syncope Dizziness Palpitations Heart Failure Chest pain
Sudden death No symptoms

5
Investigations Bedside Bloods Imaging Special tests ECG
TFTs, U+E, FBC, Troponins Imaging Echo, CXR Special tests Holter monitor

6
ARRhYTHMIAS Bradyarrhythmias vs Tachyarrhythmias Brady Tachy
HR < 60bpm Tachy HR > 100bpm

7
Bradyarrhythmias Type I heart block Type II heart block
1st degree heart block Prolonged PR interval > 0.2 seconds Type II heart block Mobitz type 1 – Wenckebach Gradually increased PR intervals until missed QRS Mobitz type 2 Intermittently P wave not followed by QRS May be pattern eg 2:1, 3:1 ratio of P waves to QRS complexes – no increase in PR interval Type III heart block Complete heart block No correlation between P waves and QRS complexes

8
Management Acute (eg. Secondary to MI) Chronic
If symptomatic/clinical deterioration IV atropine External (transcutaneous) pacing Chronic Mobitz type II or complete AV block Permanent pacemaker
 pacing. Chronic. Mobitz type II or complete AV block. Permanent pacemaker.")
9
Tachyarrhythmias Narrow complex (Supraventricular) vs Broad complex (Ventricular) Narrow QRS <0.12 seconds Broad QRS >0.12 seconds

10
Narrow complex Sinus tachycardia Atrial Fibrillation (AF)
Atrial Flutter Atrioventricular nodal re-entry tachycardia (AVNRT) Atrioventricular reciprocating tachycardia (AVRT)
 Atrioventricular reciprocating tachycardia (AVRT)")
11
AF Continuous, rapid activation of atria – due to rapidly depolarising foci within the atria Often located by pulmonary veins No coordinated mechanical action

12
AF – Causes ATRIAL PhIB A – Alcohol T – Thyroid disease
R – Rheumatic heart disease I – Ischaemic heart disease A – Atrial myxoma L – Lung pathology (pneumonia, PE) Ph – Pheochromocytoma I – Idiopathic B – Blood pressure (hypertension)
 Ph – Pheochromocytoma. I – Idiopathic. B – Blood pressure (hypertension)")
13
AF - management Conservative Medical Interventional Alcohol cessation
Lifestyle factors (diet/exercise/smoking) Medical Treat underlying cause Rate control vs rhythm control Interventional Catheter ablation
 Medical. Treat underlying cause. Rate control vs rhythm control. Interventional. Catheter ablation.")
14
Rate control Older age, permanent AF
Bisoprolol/verapamil and Warfarin (CHADSVASc)
")
15
Anticoagulation Therapy
Congestive heart failure (or Left ventricular systolic dysfunction) 1 H Hypertension: blood pressure consistently above 140/90 mmHg (or treated hypertension on medication) A2 Age ≥75 years 2 D Diabetes Mellitus S2 Prior Stroke or TIA or thromboembolism V Vascular disease (e.g. peripheral artery disease, myocardial infarction, aortic plaque) A Age 65–74 years Sc Sex category (i.e. female gender) Chadsvasc Score Risk Anticoagulation Therapy Low No antithrombotic therapy (or Aspirin) 1 Moderate Oral anticoagulant (or Aspirin) 2 or greater High Oral anticoagulant
 1. H. Hypertension: blood pressure consistently above 140/90 mmHg (or treated hypertension on medication) A2. Age ≥75 years. 2. D. Diabetes Mellitus. S2. Prior Stroke or TIA or thromboembolism. V. Vascular disease (e.g. peripheral artery disease, myocardial infarction, aortic plaque) A. Age 65–74 years. Sc. Sex category (i.e. female gender) Chadsvasc. Score. Risk. Anticoagulation Therapy. Low. No antithrombotic therapy (or Aspirin) 1. Moderate. Oral anticoagulant (or Aspirin) 2 or greater. High. Oral anticoagulant.")
16
Rhythm control Cardioversion < 48 hours
Pharmacological vs DC younger, symptomatic, physically active patients Congestive heart failure Paroxysmal AF failure of rate control < 48 hours Cardioversion + heparin > 48hrs – TOE/anti-coagulation (3 weeks) risk of failure? High – 4 weeks sotalol/amiodarone then electrical. Low - electrical
 risk of failure High – 4 weeks sotalol/amiodarone then electrical. Low - electrical.")
17
Rhythm control Pharmacological Interventional
No structural heart disease 1st - Flecainide 2nd – Sotalol 3rd – Amiodarone Structural heart disease Amiodarone Interventional Pulmonary vein isolation - catheter ablation

18
Atrial Flutter Organised atrial rhythm, coming from ectopic focus in atria (usually left) Usually 300bpm Ventricular rate depends on degree of AV block eg 2:1 = 150bpm Saw tooth pattern

19
Atrial Flutter Management Conservative Medical – similar to AF
Vagal manoeuvres Medical – similar to AF Acute DC cardioversion or IV adenosine (<48 hours) > 48 hours - 3 weeks anticoag then cardiovert Chronic Pill in pocket Regular anti-arrhythmics Interventional Radiofrequency catheter ablation
 > 48 hours - 3 weeks anticoag then cardiovert. Chronic. Pill in pocket. Regular anti-arrhythmics. Interventional. Radiofrequency catheter ablation.")
20
AVNRT 2 pathways within the AV node
1) short refractory period + slow conduction 2) long refractory period + fast conduction Normally conducts through fast pathway If premature atrial beat, fast pathway still refractory (long refractory period) therefore travels down slow pathway and back up the fast pathway.
 short refractory period + slow conduction. 2) long refractory period + fast conduction. Normally conducts through fast pathway. If premature atrial beat, fast pathway still refractory (long refractory period) therefore travels down slow pathway and back up the fast pathway.")
21
avnrt

22
AVRT Accessory pathway (Bundle of Kent most common)
Pre-excitation (delta wave) on ECG Wolff-Parkinson-White syndrome
 on ECG. Wolff-Parkinson-White syndrome.")
23
Management of SVTs Haemodynaically unstable Conservative Medical
Electrical cardioversion Conservative Vagal manoeuvres Valsalva, carotid massage, cold water Medical Adenosine (acute) Anti-arrhythmics (regular and pill-in-pocket) Interventional Catheter ablation
 Anti-arrhythmics (regular and pill-in-pocket) Interventional. Catheter ablation.")
24
Broad complex tachys VT vs VF
Unstable electrical cardioversion Stable 1st – Class I Anti-arrhythmics (lidocaine) 2nd – Amiodarone 3rd – DC cardioversion
 2nd – Amiodarone. 3rd – DC cardioversion.")
25
Broad complex tachys VT vs VF
Cardiac arrest Rapid, irregular activity – no cardiac output Usually provoked by ventricular ectopic beat Management Electrical defibrillation

26
Broad complex tachys Something to be aware of
SVT with concomitant bundle branch block = broad complex tachy

27
Summary Brady vs tachy Remember causes of AF Brady Tachy Sinus Brady
1st degree heart block Mobitz I & II Complete Tachy Narrow Sinus tachy, AF, Flutter, AVNRT, AVRT Broad VT, VF, Remember causes of AF

28
ECGs – test yourself

29
A

30
B

31
C

32
D

33
E

34
F

35
G

36
H

37
I

38
J

39
K

40
L

41
Answers Sinus rhythm AF Atrial Flutter VT VF 1st degree heart block
Complete heart block Mobitz type II AVRT Mobitz type I AVNRT Right bundle branch block

42
References All images and ECGs borrowed gratefully from google images
Kumar & Clarke: Clinical Medicine 7th Ed NICE guidelines: AF (CG36)
")
Similar presentations


















 Autonomic Nervous System.>")
