Download presentation
Presentation is loading. Please wait.

1
Timothy E Byun, MD Hematology-Oncology Medical Group of Orange County, Inc. May 14, 2011

2
Objectives Review current treatment options for patients with advanced melanoma Discuss newly approved adjuvant therapy option in high risk melanoma Discuss newly approved therapeutic approach in advanced melanoma Discuss emerging therapeutic options in metastatic melanoma

4
Interferon α-2b as the only FDA approved adjuvant therapy for high-risk Melanoma High-dose Inteferon has shown to improve relapse-free survival compared to observation Its impact on overall survival has been less clear Meta-analysis of 14 randomized trials from 1990 to 2008 shows statistically significant improvement in both Disease Free Survival and Overall Survival S Mocellin, et al. JNCI 2010;102(7):493-501.
:")
5
IFN-α increases Disease Free Survival rate HR=0.82 [0.77-0.87; p<0.001] Mocellin S et al. JNCI J Natl Cancer Inst 2010;102:493-501 © The Author 2010. Published by Oxford University Press.
![IFN-α increases Disease Free Survival rate HR=0.82 [ ; p<0.001] Mocellin S et al.](http://images.slideplayer.com/18/5678015/slides/slide_5.jpg "JNCI J Natl Cancer Inst 2010;102: © The Author Published by Oxford University Press..")
6
IFN-α increases Overall Survival rate HR=0.89 [0.83-0.96; p=0.002] Mocellin S et al. JNCI J Natl Cancer Inst 2010;102:493-501 © The Author 2010. Published by Oxford University Press.
![IFN-α increases Overall Survival rate HR=0.89 [ ; p=0.002] Mocellin S et al.](http://images.slideplayer.com/18/5678015/slides/slide_6.jpg "JNCI J Natl Cancer Inst 2010;102: © The Author Published by Oxford University Press..")
7
Peginterferon α-2b (Sylantron) is approved for Stage III Melanoma Adjuvant Therapy Based on an open-label multi-center trial of 1256 patients Microscopic or Gross lymph nodal disease with complete resection Sylantron or placebo 1:1 randomization for 5 year treatment 33 % of patients discontinued treatment due to adverse reactions Most common adverse reactions were fatigue, depression, anorexia, elevated AST/ALT, myalgia, nausea, headache, and pyrexia
 is approved for Stage III Melanoma Adjuvant Therapy Based on an open-label multi-center trial of 1256 patients Microscopic or Gross lymph nodal disease with complete resection Sylantron or placebo 1:1 randomization for 5 year treatment 33 % of patients discontinued treatment due to adverse reactions Most common adverse reactions were fatigue, depression, anorexia, elevated AST/ALT, myalgia, nausea, headache, and pyrexia")
8
Peginterferon α-2b (Sylantron) is approved for Stage III Melanoma Adjuvant Therapy Increased Relapse-Free Survival Time compared to placebo: 34.8 months vs 25.5 months (HR 0.82 [0.71-0.96]; p = 0.011] No Difference in Overall Survival (HR 0.98 [0.82-1.16] Unknown efficacy compared to high-dose interferon therapy Probably better tolerated compared to high-dose interferon therapy
![Peginterferon α-2b (Sylantron) is approved for Stage III Melanoma Adjuvant Therapy Increased Relapse-Free Survival Time compared to placebo: 34.8 months vs 25.5 months (HR 0.82 [ ]; p = 0.011] No Difference in Overall Survival (HR 0.98 [ ] Unknown efficacy compared to high-dose interferon therapy Probably better tolerated compared to high-dose interferon therapy](http://images.slideplayer.com/18/5678015/slides/slide_8.jpg "Peginterferon α-2b (Sylantron) is approved for Stage III Melanoma Adjuvant Therapy Increased Relapse-Free Survival Time compared to placebo: 34.8 months vs 25.5 months (HR 0.82 [ ]; p = 0.011] No Difference in Overall Survival (HR 0.98 [ ] Unknown efficacy compared to high-dose interferon therapy Probably better tolerated compared to high-dose interferon therapy")
10
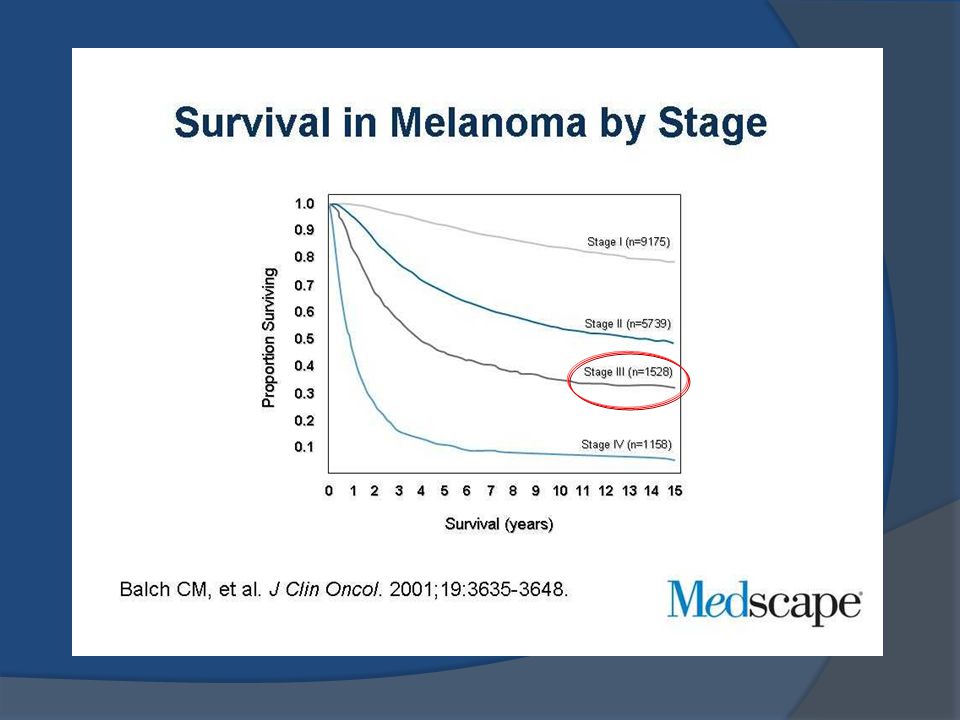
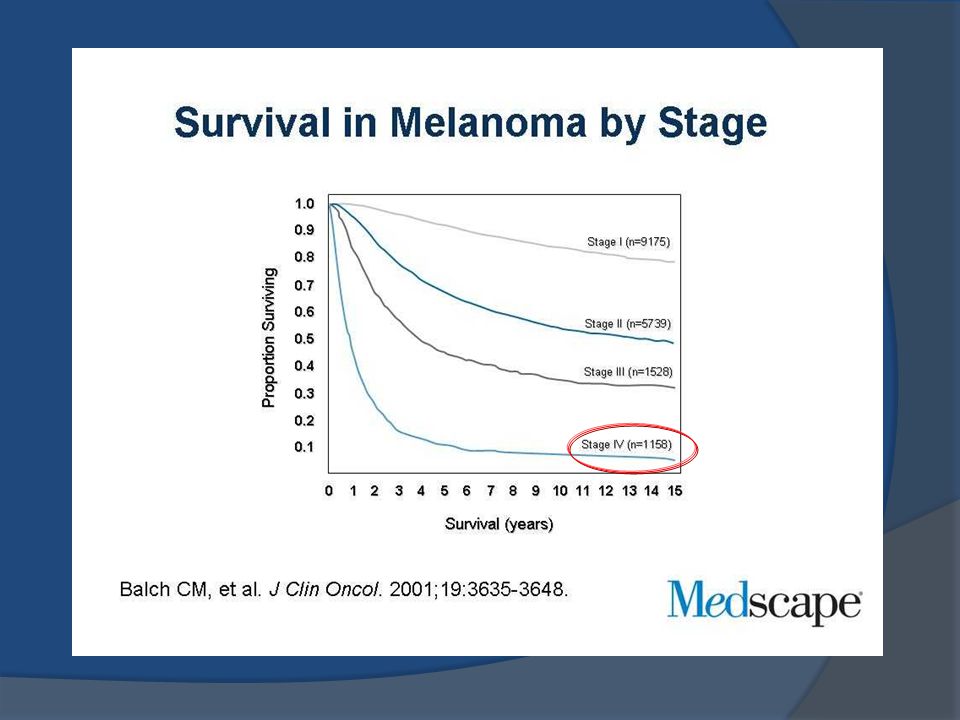
Prognosis is poor for metastatic melanoma patients Less than 10% survive 5 years Median survival of 6-9 months Very low response to current existing chemotherapy or immunotherapy Up until now, no randomized study has ever demonstrated survival benefit

11
Many studies failed to show survival benefit

12
Treatment Options for Metastatic Melanoma Surgical resection of metastases Chemotherapy: IV Dacarbazine (DTIC) FDA approval 1976 Response rate <10% and median time to progression of <2 months Immunotherapy: high-dose interleuken-2 (IL-2) FDA approval 1998 based on phase II data Response rate ~17%, durable response rate ~6% Requires hospitalization, manageable but severe side effects Avril MF, Aamdal S, Grob JJ, et al. JCO 2004;22:1118-1125. Atkins MB, Lotze MT, Dutcher JP, et al. JCO 1999;17:2105-2116.

13
Few patients experience durable response to high dose IL-2

16
Adapted from ASCO 2008 meeting. Suzanne Louise Topalian, MD

17
T Cell Activation by TCR and Co-stimulation Through CD28 Dendritic cell T cell MHC B7 TCR CD28 Antigen CTLA4

18
CTLA4 Receptors Are Up-Regulated Following T-Cell Activation Dendritic cell T cell MHC B7 TCR CD28 Antigen CTLA4

19
Dendritic cell T cell MHC B7 TCR CD28 Antigen CTLA4 CTLA4 Negatively Modulates T-Cell Activation

20
Dendritic cell T cell MHC B7 TCR CD28 Antigen CTLA4 Blocking Antibodies to CTLA4 Allow Positive Signaling from Costimulatory Molecules to T Cells Leach DR, Krummel MF, Allison JP. Enhancement of antitumor immunity by CTLA-4 blockade. Science 1996;271:1734-1736.

21
Ipilimumab(Yervoy) in Treatment of Cancer CTLA-4: Down-regulates T-cell activation Ipilimumab(Yervoy): Fully human monoclonal antibody Blocks CTLA-4 receptor Potentiates T cell activation Korman, Peggs and Allison: Adv. In Immunol. 2006;90:297-339

22
Ipilimumab: Mechanism of Action T cell TCR CTLA4 APC MHC B7 T-cell inhibition T cell TCR CTLA4 APC MHC B7 T-cell activation T cell TCR CTLA4 APC MHC B7 T-cell potentiation IPILIMUMAB blocks CTLA-4 CD28

23
MDX010-20: Study Design RANDOMIZERANDOMIZE Pre-treated Metastatic Melanoma (N=676) (N=137) (N=136) (N=403) gp100 + placebo Ipilimumab + placebo Ipilimumab + gp100
 (N=137) (N=136) (N=403) gp100 + placebo Ipilimumab + placebo Ipilimumab + gp100")
24
MDX010-20: Study Design Details Accrual: September 2004 – July, 2008 125 Centers in 13 Countries Randomized (3:1:1), Double-Blind Stratified for M-Stage and prior IL-2 Induction Ipilimumab: 3 mg/kg q 3 weeks X 4 doses gp100: 1mg q 3 weeks X 4 doses Re-induction (same regimen) in eligible patients
, Double-Blind Stratified for M-Stage and prior IL-2 Induction Ipilimumab: 3 mg/kg q 3 weeks X 4 doses gp100: 1mg q 3 weeks X 4 doses Re-induction (same regimen) in eligible patients")
25
= 1 st tumor assessment as per protocol Ipilimumab Improves Progression Free Survivial Compared to Control Ipi + gp100 (A) Ipi alone (B) gp100 alone (C) 1234 Years Comparison Hazard Ratio (C.I.) p-value Comparison Hazard Ratio (C.I.) p-value Arms A vs C 0.81 (0.66–1.00) 0.0464 Arms B vs C 0.64 (0.50–0.83) 0.0007 Arms A vs B 1.25 (1.01–1.53) 0.0371
 Ipi alone (B) gp100 alone (C) 1234 Years Comparison Hazard Ratio (C.I.) p-value Comparison Hazard Ratio (C.I.) p-value Arms A vs C 0.81 (0.66–1.00) Arms B vs C 0.64 (0.50–0.83) Arms A vs B 1.25 (1.01–1.53)")
26
Ipi + pbogp100 + pboP-value Secondary Comparison N 137136 0.0026 Number of deaths 100119 Hazard ratio (95% CI) 0.66 (0.51, 0.87) Median OS, Month (95% CI) 10.1 (8.0,13.8) 6.4 (5.5, 8.7) Ipilimumab Improves Overall Survival Compared to Control
 0.66 (0.51, 0.87) Median OS, Month (95% CI) 10.1 (8.0,13.8) 6.4 (5.5, 8.7) Ipilimumab Improves Overall Survival Compared to Control")
27
Survival RateIpi + gp100 N=403 Ipi + pbo N=137 gp100 + pbo N=136 1 year44%46%25% 2 year22%24%14% Ipilimumab Improves Overall Survival compared to control Ipi + gp100 (A) Ipi alone (B) gp100 alone (C) 1234 Years
 Ipi alone (B) gp100 alone (C) 1234 Years")
28
What mediates anti-CTLA4-induced durable tumor regressions? Brown: CD8+ T cells Blue: melanoma 2005 Durable response > 5 years Treatment with anti-CTLA4 antibodies The great majority of responses last years without relapses: - Longest responder: Ongoing since May 2001 - Response rate: ~10%

29
Ipilimumab improved Survival in all subgroups

30
Ipilimumab is associated with increased serious adverse effects % of Patients Ipi + gp100 N=380 Ipi + pbo N=131 gp100 + pbo N=132 Any adverse event (AE)98.496.997.0 Treatment - related Any AE 88.980.278.8 Treatment - related Grade 3/4 AE 17.422.911.4 Treatment - related Deaths 2.13.11.5
 Treatment - related Any AE Treatment - related Grade 3/4 AE Treatment - related Deaths")
31
Most Common Immune-Related Adverse Events* (Grades 3, 4 and 5) % of Patients irAE Ipi + gp100 N=380 Ipi + pbo N=131 gp100 + pbo N=132 Grade 3Grade 4Grade 3Grade 4Grade 3Grade 4 Any9.70.512.22.33.00 Dermatologic2.10.31.5000 GI5.30.57.600.80 Endocrine1.102.31.500 Hepatic 1.10002.30 Death due to irAE 1.31.50 *Across entire study duration
 % of Patients irAE Ipi + gp100 N=380 Ipi + pbo N=131 gp100 + pbo N=132 Grade 3Grade 4Grade 3Grade 4Grade 3Grade 4 Any Dermatologic GI Endocrine Hepatic Death due to irAE *Across entire study duration")
32
Summary First Randomized Phase III Study to Show Survival Benefit FDA approved for first-line or subsequent-line of therapy Suggests a long-term Survival Effect 2 year survival rate: 24% Some patients alive 10 years disease-free so far Immune mediated adverse effects require prompt medical attention and early administration of corticosteroids

33
Summary Ipilimumab represents a new class of T-cell potentiators and an important advance for the field of immuno-oncology Further development of ipilimumab is ongoing Diversification to a variety of cancer types and settings Alternative combination regimens Refinements in dose and schedule Next generation of anti-CTLA4 antibody?

34
Targeting BRAF kinase

36
Genetic mutations in melanomas: BRAF is frequently mutated NATURE|Vol 445|22 February 2007|doi:10.1038/nature05661 ~55%

37
BRAF is an attractive target Amena M. DeLuca, Archana Srinivas and Rhoda M. Alani (2008). Expert Rev. Mol. Med. Vol. 10, e6
. Expert Rev. Mol. Med. Vol. 10, e6.")
38
Inhibition of MAPK signaling in BRAF V600E melanoma of patients treated with PLX4032 Baseline pERK cyclin D Ki67 Day 15 Cyclin D B-Raf V600E MEK ERK P P Cell cycle (Ki67) PLX4032
 PLX4032")
39
RECIST Responses to PLX4032 (960 mg bid) in 32 Patients with BRAF V600E Mutant Melanoma (Response Rate Over 80%) -100 -75 -50 -25 0 25 50 75 100 %Change From Baseline (Sum of Lesion Size) Threshold for RECIST response Flaherty, Puzanov, Kim, Ribas, McArthur, Sosman, O’Dwyer, Lee, Grippo, Nolop, Chapman. New England Journal of Medicine 2010.

40
RECIST 30% Decrease *** RECIST Responses to PLX4032 (960 mg bid) in 132 Patients with BRAF V600E Mutant Melanoma Sosman, Kim, Schuchter, Gonzalez, Pavlick, Weber, McArthur, Hutson, Lawrence, Moschos, Flaherty, Hersey, Kefford, Chmielowski, Amaravadi, Puzanov, Li, Bhattacharya, Nolop, Lee, Joe, Ribas. Society for Melanoma Research, Sydney, Australia, 2010

41
McDermott U et al. N Engl J Med 2011;364:340-350. Dramatic Response to PLX 4032

42
Duration of responses with PLX4032: Median PFS ~ 7 months Legend M1a M1b M1c Threshold reached for PR PD Patient remaining in study

43
PLX 4032 Increases Survival in a Phase III Trial Data to be presented at ASCO 2011 Meeting in Chicago 675 patients randomized to PLX 4032 vs Dacarbazine In phase I study, response rate was over 80% and median time to progression was over 7 months Adverse effects are relatively well-tolearted and include keratoacanthoma, rash, photosensitivity, joint pain, fatigue, hair loss Skin squamous cell carcinoma are seen, but managed with local therapy without needing drug discontinuation

44
Main Problems with PLX4032: Acquired resistance On target toxicity: Squamous cell carcinomas/Keratoachantomas Jan 10 (64 d) Dec 09 (42 d) Spontaneous regression on continued therapy Progressive KA/SCC
 Dec 09 (42 d) Spontaneous regression on continued therapy Progressive KA/SCC")
45
Conclusion Adjuvant therapy options for stage III resected melanoma: High-dose Interferon alpha-2b or Peginteferon(Sylantron) Ipilimumab is the first phase III study to show a survival benefit in metastatic melanoma Immune mediated adverse reactions need to be managed aggressively with steroids
 Ipilimumab is the first phase III study to show a survival benefit in metastatic melanoma Immune mediated adverse reactions need to be managed aggressively with steroids")
46
Conclusion PLX 4032 produces high response rate and prolongs survival in BRAF mutant metastatic melanoma patients Overcoming PLX 4032 Resistance poses a challenge Unclear sequencing of new drugs and old drugs: Sequencing based on BRAF mutation status and Tumor burden/Performance Status?

47
The goal: increase the number of long-term survivors Adapted from ASCO2008 meeting Patrick Hwu, MD

48
Thank You!

Similar presentations



:>")

 in combination with chemotherapy: pivotal metastatic breast cancer survival data 1.>")






 Comparing BRAF Inhibitor.>")





: investigational agents TTP = median time to disease progression OS = median overall survival.>")
 in Metastatic Castration-Resistant Prostate Cancer (mCRPC): Results from a Phase II Randomized Discontinuation Trial Hussain M et.>")