Download presentation
Presentation is loading. Please wait.

1
Am J Gastroenterol 2012; 107:46–52

2
Drmohammad Sadrkabir

3
Hepatitis B and hepatitis C are well-known etiological factors that lead to hepatocellular carcinoma (HCC) in Taiwan. Cirrhosis, obesity, diabetes mellitus (DM), fatty liver disease, hereditary hemochromatosis, alcohol, smoking, and other dietary and environmental exposures are also factors that contribute to the development of HCC. A recent case–control study that consists of 2,061 patients with HCC and 6,183 noncancer controls has shown a significant association between DM and the risk of HCC with an odds ratio of 2.87. A study of site-specific cancer mortality in Asian populations has also reported that DM is associated with higher risk of mortality from liver and pancreatic cancer (1.51 and 1.78, respectively).
, fatty liver disease, hereditary hemochromatosis, alcohol, smoking, and other dietary and environmental exposures are also factors that contribute to the development of HCC. A recent case–control study that consists of 2,061 patients with HCC and 6,183 noncancer controls has shown a significant association between DM and the risk of HCC with an odds ratio of A study of site-specific cancer mortality in Asian populations has also reported that DM is associated with higher risk of mortality from liver and pancreatic cancer (1.51 and 1.78, respectively)..")
4
Metformin, a widely used anti-diabetic drug, has recently attracted great attention for lowering cancer risk. It has been found to inhibit cancer cell growth in vitro and in vivo. Epidemiological studies have also shown that metformin therapy is associated with reduced risks of breast cancer and HCC.

5
Another case–control study conducted in the United States also showed that treatment with metformin or thiazolidinediones is associated with a 70% reduction in HCC risk among diabetic patients. Both the case–control studies are limited, with small clinical samples of HCC. To the best of our knowledge, only one cohort study, also from Taiwan, has observed the effect of DM medication in reducing the risk of HCC among Asian populations, but only metformin was studied.

6
To clarify the role of diabetes in the risk of developing HCC, a population-based cohort study, taking advantage of a large-size data set available from the National Health Insurance program in Taiwan, was conducted. The present study investigates further whether the risk of HCC increases with the presence of hepatitis B and/or hepatitis C. Furthermore, it examines whether the HCC risk is reduced with DM therapies, including metformin and thiazolidinediones.

7
METHODS The National Health Insurance program in Taiwan is a universal health insurance system covering more than 99% of the country's population of 23 million. Data used in this analysis came from the Longitudinal Health Insurance Database, which contains the claims’ history of 1 million subjects randomly selected from the entire population. This database contains registration of insurance, inpatient and outpatient claims, prescribed drugs, and basic sociodemographic information, including sex and birth date. The retrospective cohort study was composed of two study groups: a diabetic patients group and a matched non-diabetic comparison group.

8
The diabetic group included patients with an initial diagnosis of DM who had been prescribed anti-diabetic drugs (e.g., metformin, sulfonylureas, thiazolidinediones, α-glucosidase inhibitors, D-phenylalanine derivatives, dipeptidyl peptidase 4 inhibitors, and incretin mimetic agents or insulins) in 2000–2005. All subjects younger than 20 years old on the day of diagnosis were excluded. For each diabetic patient, four subjects without medical claims for diabetes who were frequency matched with sex and age (per 5 years) in the same period were randomly selected. Subjects diagnosed with cancer before the index date were excluded from the present study. Other comorbidities presented before the index date were defined as follows: obesity, cirrhosis, alcoholic liver damage, nonalcoholic fatty liver disease, hereditary hemochromatosis ; hepatitis B, and hepatitis C.
 in the same period were randomly selected. Subjects diagnosed with cancer before the index date were excluded from the present study. Other comorbidities presented before the index date were defined as follows: obesity, cirrhosis, alcoholic liver damage, nonalcoholic fatty liver disease, hereditary hemochromatosis ; hepatitis B, and hepatitis C..")
9
Both diabetic and non-diabetic groups were followed up to determine the incidence of HCC until the end of 2008 or censored because of death, withdrawal from the insurance program, or loss to follow-up consultations. All types of personal identification on files connected with the present study were scrambled using surrogate identification numbers to secure patient privacy. The present study was exempted from ethical review.

10
Statistical analysis χ 2 -Tests and Student's t-tests were used to compare the differences between the DM group and the non-diabetic group regarding sociodemographic characteristics and comorbidities. Cox proportional hazard models were used to estimate the HR with 95% CI, which determined the association between diabetes and the risk of developing HCC. The risk of developing HCC associated with comorbidities such as DM, cirrhosis, hepatitis B, and hepatitis C were also estimated. Further analysis investigated medications available for the DM treatment. The Cox proportional hazard analysis was also used to estimate whether there were reduced HCC risks associated with DM medications. All analyses were performed using the SAS software version 9.1 (SAS Institute, Cary, NC), and the statistical significance level was set at two-sided P<0.05.
, and the statistical significance level was set at two-sided P<")
11
RESULTS

14
The multivariate Cox proportional hazard regression analysis with sex, age, and comorbidities:

17
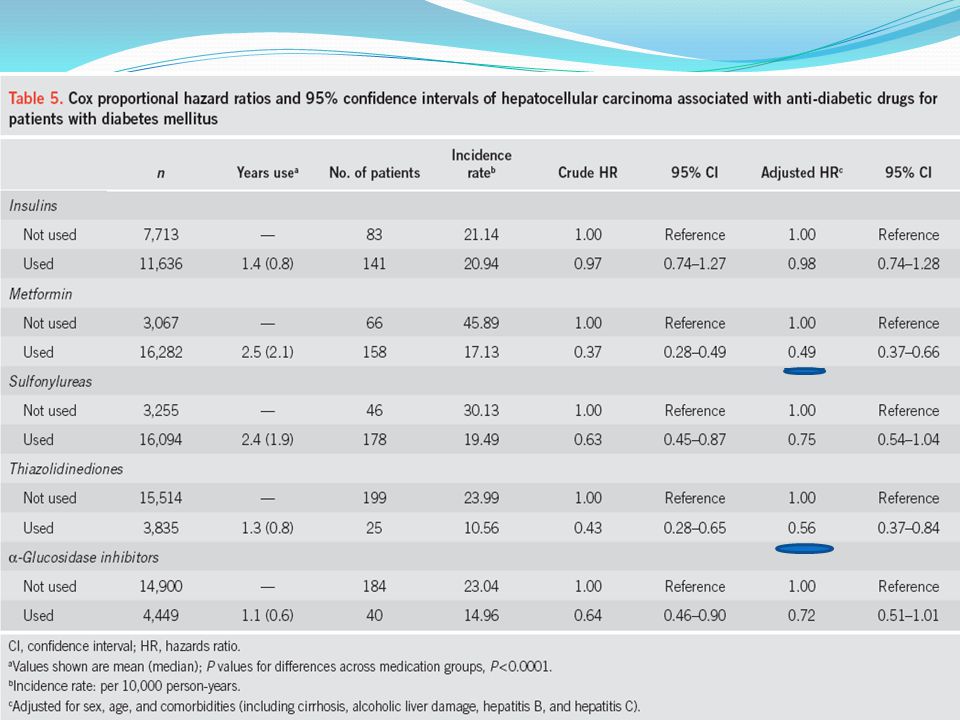
As shown in Table5, the association between anti-diabetic drugs and the risk of HCC was further analyzed. The median duration of taking metformin was 2.1 years (mean, 2.5 years), similar to that of sulfonylureas (mean, 2.4 years), but more than 1 year longer than that of other anti-diabetic drugs (P<0.001). After adjusting for sex, age, and comorbidities, the patients taking metformin had the lowest HCC HR at 0.49 (95% CI=0.37–0.66), followed by patients taking thiazolidinediones (HR=0.56, 95% CI=0.37–0.84). Taking insulin, sulfonylurea, and α-glucosidase inhibitors also reduced the HCC risk; however, the reductions were not statistically significant.Table5
, similar to that of sulfonylureas (mean, 2.4 years), but more than 1 year longer than that of other anti-diabetic drugs (P<0.001). After adjusting for sex, age, and comorbidities, the patients taking metformin had the lowest HCC HR at 0.49 (95% CI=0.37–0.66), followed by patients taking thiazolidinediones (HR=0.56, 95% CI=0.37–0.84). Taking insulin, sulfonylurea, and α-glucosidase inhibitors also reduced the HCC risk; however, the reductions were not statistically significant.Table5.")
18
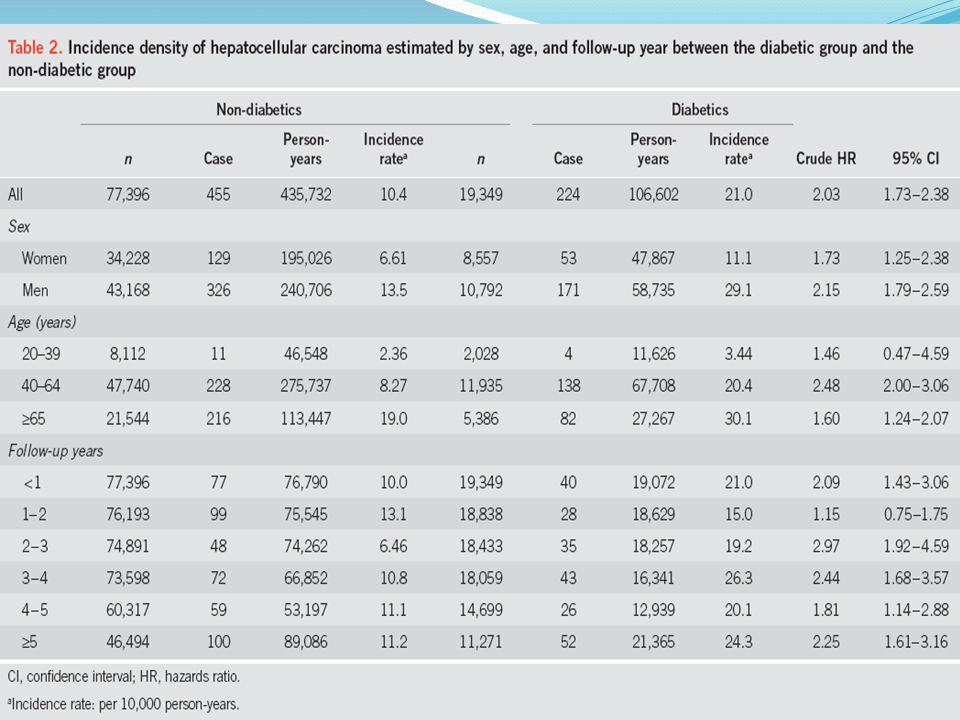
DISCUSSION Diabetic patients have an incidence of HCC twice higher than non-diabetics, indicating that approximately 11 additional cases of HCC develop annually per 10,000 diabetic patients. The incidence of HCC is higher in patients with DM regardless of sex, age, or follow-up period. The adjusted HR for developing HCC in diabetics in the current study is 1.73, which is lower than the risk found in other studies. In the systematic review by El-Serag et al., DM was associated with an increased risk of developing HCC (risk ratio=2.5, 95% CI=1.9–3.2) independent of alcohol use or viral hepatitis. Another systematic review showed that patients with DM are 3.64 times (95% CI=2.61–5.07) more likely to develop HCC compared with non-diabetics.
 independent of alcohol use or viral hepatitis. Another systematic review showed that patients with DM are 3.64 times (95% CI=2.61–5.07) more likely to develop HCC compared with non-diabetics..")
19
In line with previous findings, the present study observed a synergistic effect between DM and liver comorbidities regarding the development of HCC. The HCC risk was strongly associated with these three comorbidities, particularly cirrhosis (HR=8.65). Patients with hepatitis C are at twice higher HCC risk than those with hepatitis B (HR=5.61 vs. HR=2.52). A new and significant finding is that HCC increased markedly to an HR of 72.4 for diabetics with cirrhosis and hepatitis C compared with patients without those disorders.
. Patients with hepatitis C are at twice higher HCC risk than those with hepatitis B (HR=5.61 vs. HR=2.52). A new and significant finding is that HCC increased markedly to an HR of 72.4 for diabetics with cirrhosis and hepatitis C compared with patients without those disorders..")
20
Several studies have assessed the association between anti- diabetic drugs and the risk of developing HCC; all found reduced risk associated with metformin treatment. The results of the present study confirm the effect of metformin. Furthermore, we found that thiazolidinedione treatment is also significantly associated with a reduced incidence of HCC. To our knowledge, only one hospital-based case– control study in the United States has shown that thiazolidinediones may reduce the risk of HCC, which is consistent with our observation. Evidence from in vivo studies has shown that thiazolidinediones inhibited tumor formation in the liver.

21
Previous case–control studies have shown that sulfonylurea users have an increased risk of developing HCC compared with non-users. In contrast, the present study shows a 25% risk reduction in patients using sulfonylureas, but the association was not statistically significant. We found that 92.5% of sulfonylurea users have switched to other anti- diabetic drugs, which might, to some extent, offset the unfavorable effect of sulfonylurea on risk of HCC. Further prospective studies may be helpful for clarifying the association of sulfonylureas with HCC.

22
A hospital-based case–control study in the United States found that patients that have had diabetes for >10 years have a 2.2-fold increased risk of developing HCC (95% CI=1.2–4.8) compared with those that have had diabetes for 2 to 5 years. Thus, the risk may increase with the increasing duration of DM. We assessed the risk of developing HCC in terms of the duration of taking anti-diabetic drugs. The risk of developing HCC decreased as the duration of taking the medications increased. The trend is most obvious for patients who have been taking metformin for at least 1 year. The HR was 0.49 (95% CI=0.31– 0.78) after taking metformin for 12–23 months, which decreased to 0.26 (95% CI=0.18–0.39) after taking it for ≥24 months compared with non-users of metformin (data not shown). This trend was less pronounced among patients taking α-glucosidase inhibitors.
 after taking metformin for 12–23 months, which decreased to 0.26 (95% CI=0.18–0.39) after taking it for ≥24 months compared with non-users of metformin (data not shown). This trend was less pronounced among patients taking α-glucosidase inhibitors..")
23
The strength of the present study is its large sample size. Although the concept is not novel, the population-based data set with a large sample size allows the demonstration of risk factors for HCC with a minimal tendency for selection bias in Taiwan. However, the present study has a number of limitations. First, a number of suspected risk factors for HCC were not available, such as cigarette smoking, aflatoxin exposure, and body mass index. Second, the claims’ data do not contain laboratory test results. Thus, the extent of DM control among the study subjects was not accounted for because hemoglobin A1c values are not available. Third, this observational study does not explore the mechanism by which DM is related to HCC. Finally, misclassification and measurement errors in drug exposure might have occurred if the patients failed to take the prescribed drugs. Non-compliance is likely to cause underestimation of the drug effect.

24
CONCLUSION The current study suggests that patients with DM have a higher risk of developing HCC. Comorbidities such as cirrhosis, hepatitis B, and hepatitis C significantly aggravate the risk of developing HCC. The markedly elevated risk of developing HCC associated with hepatitis C and its synergism with cirrhosis provides new insights into HCC prevention. This observation may prompt the screening of high-risk patients. On the other hand, patients taking metformin or thiazolidinediones have reduced risks of developing HCC.

25
Thank you for your attention

Similar presentations



. What is a cohort?>")

















