Download presentation
Presentation is loading. Please wait.

1
SON Breast Cancer Update: Current Controversies Oct 18, 2014 Who should we radiate and why? Lorna Weir Radiation Oncologist BC Cancer Agency, Vancouver Centre

2
Faculty/Presenter disclosure –Dr. Lorna Weir –Relationships with commercial interests: –none

3
Disclosure of Commercial Support –Dr. Lorna Weir –Commercial support for this meeting is listed in the program –I have no personal commercial support

4
Mitigating Potential Bias –Dr. Lorna Weir –n/a

5
Outline Post – lumpectomy breast radiation - why Management of nodal regions in sentinel node era Who should we not radiate Management of axilla after neo-adjuvant chemo (radiation perspective) Summary/conclusions
 Summary/conclusions")
6
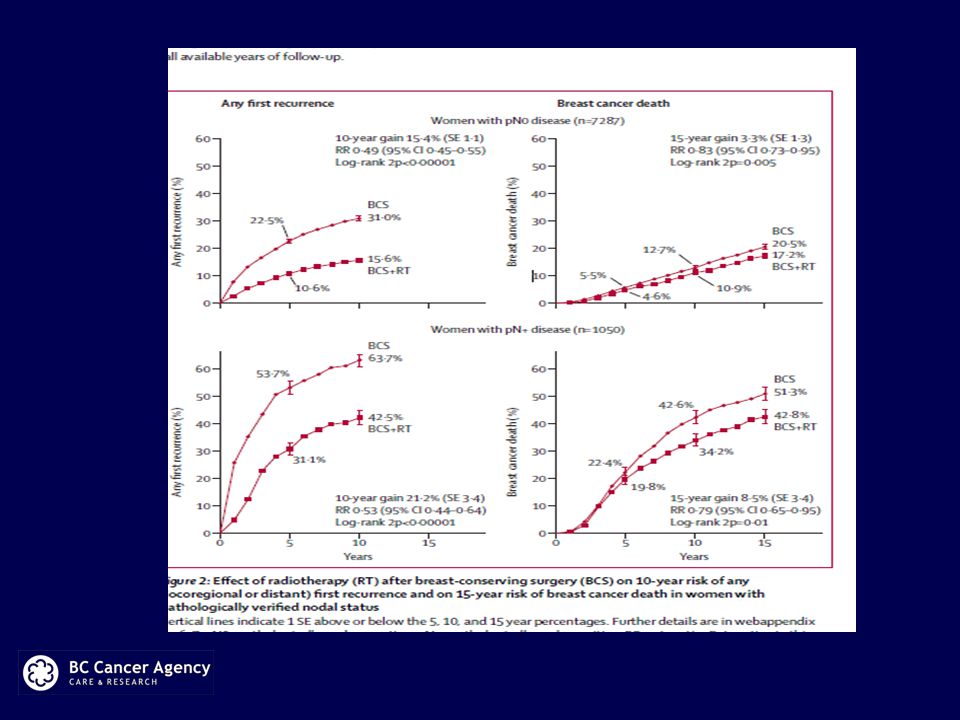
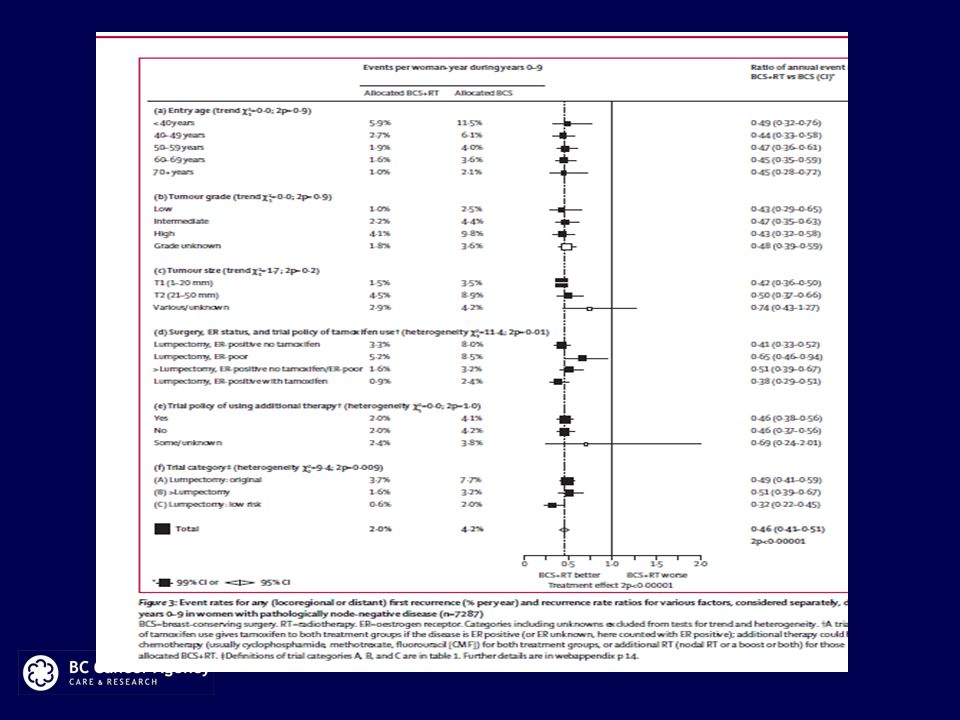
Post Lumpectomy Breast Radiation Early stage invasive breast cancer Effect of radiotherapy after BCS, meta-analysis (Lancet 2011, 378:1707-16) 10,801 women, 17 randomized trials Lumpectomy +/- radiation (most trials only breast radiation) Overall RT reduced 10 year risk of any first recurrence from 35% to 19% ** one breast cancer death was avoided for every 4 recurrences avoided for both node – and + disease
 10,801 women, 17 randomized trials Lumpectomy +/- radiation (most trials only breast radiation) Overall RT reduced 10 year risk of any first recurrence from 35% to 19% ** one breast cancer death was avoided for every 4 recurrences avoided for both node – and + disease")
9
Management of the nodal regions in the sentinel node era - background –McGill metaanalysis looked at loco-regional recurrence rates from 1990-2011 –53 randomized studies of adjuvant therapy for early breast cancer, 86,598 patients –Proportion of local recurrences decreased from 30% to 15% of all recurrences in the time period –distant recurrences also declined but magnitude was less –In this era, specialized breast surgical oncology increased, surgical treatment of the axilla became less, and systemic therapy use increased Bouganim, Br Cancer Res Treat (2013) 139:603
 139:603")
10
Management of the nodal regions in the sentinel node era – newer studies ACSOG Z0011 published 2011 (Giuliano, JAMA) –Closed early, 901 pts –Lumpectomy and breast RT, SNB, 1-2 positive nodes –Randomized to ALND vs “ no further axillary treatment ” –Med FU 6.3 years –27% had additional pos+ nodes after ALND –5 yr OS and DFS was not inferior for SNB alone. –No difference in LR recurrences

11
Management of the nodal regions in the sentinel node era – newer studies ACSOG Z0011 – radiation details from abstract at SABCS 2013 Subgroup of pts with details of RT available: –81 % of pts had breast tangents only –~50 % of these had “high tangents” –19 % also had nodal radiation (≥ 3 fields) and these tended to have greater nodal involvement –“No conclusions can be drawn from the analysis as to whether the treatment was necessary or beneficial”
 and these tended to have greater nodal involvement – No conclusions can be drawn from the analysis as to whether the treatment was necessary or beneficial")
14
Management of the nodal regions MA 20 (NCIC) Women with node-positive breast cancer (or high risk node negative) treated with BCS and adjuvant chemotherapy and/or endocrine therapy Randomized to : –Whole breast radiation alone or –Whole breast radiation plus nodal radiation to the internal mammary, supraclavicular, and high axillary lymph nodes. Whelan, ASCO 2011

15
Management of the nodal regions – MA 20 Interim analysis 2011 RESULTS : 1,832 women. Median follow-up was 62 months. mean age 53.3 years node negative 10% 1-3 positive nodes 85% > 4 positive nodes 5% 91% had chemo 71% had endocrine Rx Whelan, ASCO 2011

16
Management of the nodal regions – MA 20 DFS was 84 % vs 89.7 % HR 0.68 OS was 90.7 % vs 92.3 % (n.s.) Locoreg failure was 5.5 % vs 3.2 % DM rate was 13 % vs 7.6 % Whelan, ASCO 2011
 Locoreg failure was 5.5 % vs 3.2 % DM rate was 13 % vs 7.6 % Whelan, ASCO 2011")
17
Management of the nodal regions - MA 20 Pneumonitis 0.2 % vs 1.3 % Lymphedema was 4% vs 7% Whelan, ASCO 2011

18
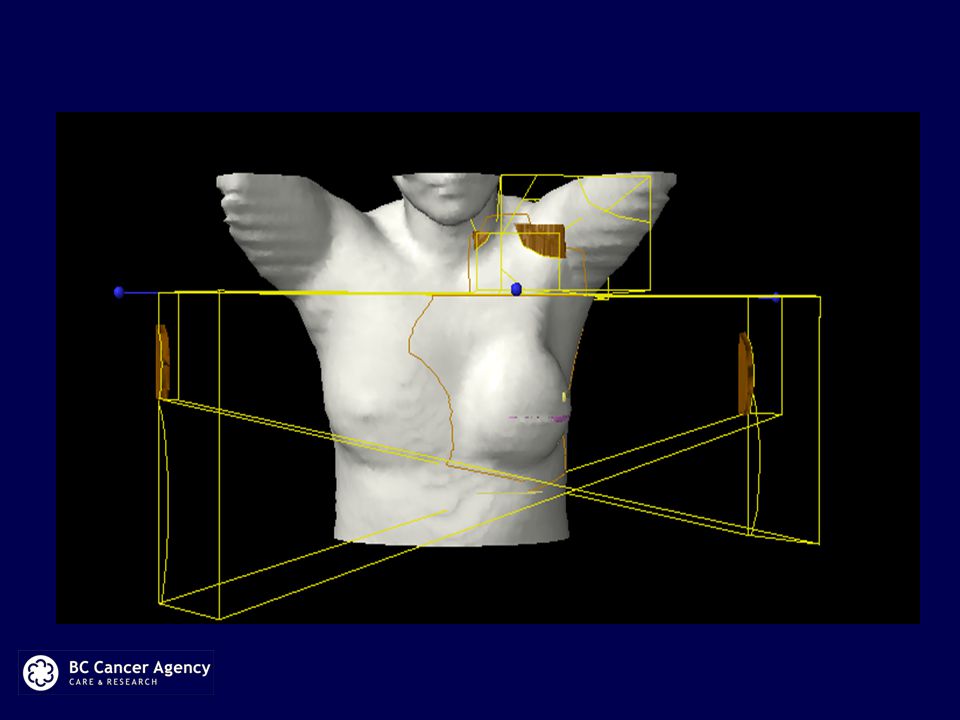
NCIC MA 20

19
EORTC phase III trial 22922/10925 BCS or Mastectomy Positive nodes or medial/central located tumours RT to breast/CW only RT to breast/CW and SCV+IM 4004 Patients with med FU 10.9 yrs BCS 76% Post menop 59% 85% systemic treatment Most pts pT1 and pT2 Node neg- 44% ( must be medial or central primary tumour)
")
20
EORTC 22922 At 10 yrs - in favour of the nodal RT arm: Overall survival : 80.7 % vs 82.3 % (HR 0.87; P 0.049) Disease-free survival: 69 % vs 72 % ( HR 0.89; P 0.044) Metastases-free survival: 75 % vs 78 % (HR 0.86 P= 0.02) Node neg subgroup also benefitted from RT
 Disease-free survival: 69 % vs 72 % ( HR 0.89; P 0.044) Metastases-free survival: 75 % vs 78 % (HR 0.86 P= 0.02) Node neg subgroup also benefitted from RT")
21
EORTC 22922 Lung toxicity (pneumonitis, fibrosis, dyspnea) 4.3% vs. 1.3% Cardiac disease : 1.4% vs. 1.6% (NS)
.")
22
AMAROS= After Mapping of the Axilla RT or Surgery (EORTC phase III RCT) Non-inferiority Eligible -Invasive Ca -Clinical node N0 - BCS or Mastectomy -No age limit
 Non-inferiority Eligible -Invasive Ca -Clinical node N0 - BCS or Mastectomy -No age limit")
23
Management of the nodal regions in patients with positive sentinel nodes – newer studies AMAROS 1425 pts with positive sentinel node Randomized to completion ALND (n = 744) vs nodal radiation (n = 681) 90% had systemic Rx 82 % had breast conservation Lymphedema rate ~ double in surgery arm
 vs nodal radiation (n = 681) 90% had systemic Rx 82 % had breast conservation Lymphedema rate ~ double in surgery arm")
24
AMAROS trial results: 5 years follow-up ARRDFSOS ART1.03% (7pts)82.7%92.5% AND0.54% (4pts)86.9% HR 1.17, P = 0.18 93.3% HR 1.17, p= 0.34 ( The LRR was so low in both groups that the study turned out to be underpowered for assessing non-inferiority between the two treatments, which was one of its original goals, according to the abstract) The ARR after a negative sentinel node biopsy was 0.8%
82.7%92.5% AND0.54% (4pts)86.9% HR 1.17, P = % HR 1.17, p= 0.34 ( The LRR was so low in both groups that the study turned out to be underpowered for assessing non-inferiority between the two treatments, which was one of its original goals, according to the abstract) The ARR after a negative sentinel node biopsy was 0.8%")
25
Personalized Medicine Breast Radiation Available prognostic and predictive factors for IBTR are useful but not definitive –Age, tumour size, grade, receptors, margins and LVI, nodal status are prognostic for breast recurrence –Limited in their predictive ability for benefit from RT Some women will receive no benefit from breast RT - experience side effects and inconvenience

26
Personalized Medicine – Who not to Radiate Molecular profiling can define risk in sufficient detail to allow selection for systemic treatment avoidance –IHC 4 –Oncotype and Mammaprint Can expression profiling identify patients at low risk for local recurrence? –Avoidance of breast RT

27
Voduc K D et al. JCO 2010;28:1684-1691 Breast Cancer Subtypes and Risk of Local and Regional Relapse Six Biomarker Panel for Defining Subtypes (Voduc et al JCO 2010, 28 1684-91) SubtypeERPRHER2CK5/6EGFRKi67 Lum AEither positiveNegativeAny Neg Lum BEither positiveNegativeAny Pos Lum HER2 Either positivePositiveAny HER2Negative PositiveAny BasalNegative Either positiveAny TN non- basal Negative Any
 SubtypeERPRHER2CK5/6EGFRKi67 Lum AEither positiveNegativeAny Neg Lum BEither positiveNegativeAny Pos Lum HER2 Either positivePositiveAny HER2Negative PositiveAny BasalNegative Either positiveAny TN non- basal Negative Any.")
28
Randomized Trial, 769 pts IBTR 13.8% for Tam vs 5.3% for Tam/RT at 10 years, P<0.0001

29
IBTR for Luminal A by Treatment Group Tam 7.1% Tam/RT 4.3% P = 0.3

30
IBTR for Luminal B by Treatment Group Tam 19.5% Tam/RT 3.5% P = 0.018

31
LUMINA trial Prospective cohort study Ontario and BC, funded Women –60 or older – tumours 2 cm or less –Margins 2mm or more –Grade 1 and 2 –Node neg –Not multifocal –If consent Ki-67 done –Low no breast RT –High breast RT

32
SNB after neo-adjuvant chemo For patients with initial positive nodes, there are 2 multicenter prospective trials looking at SNB alone (Boughey and Kuehn) FN rates are ~30% if only 1 SN removed, but go down to 10% if 3 SN’s are removed For these patients the current standard of care is still to give loco-regional radiation (treat as node positive)
 FN rates are ~30% if only 1 SN removed, but go down to 10% if 3 SN’s are removed For these patients the current standard of care is still to give loco-regional radiation (treat as node positive)")
33
Open trials which address these questions NSABP B51/RTOG 1304 –Phase III –Patients who present with N1 disease before neo-adjuvant chemo, who become path node neg at surgery (either SNB +/- ALND) –Mastectomy patients randomized to no RT vs RT to chest wall and nodes –Lumpectomy patients randomized to breast RT vs breast and nodal RT
 –Mastectomy patients randomized to no RT vs RT to chest wall and nodes –Lumpectomy patients randomized to breast RT vs breast and nodal RT")
34
Open trials which address these questions ALLIANCE (A011202) –Phase III –FNA or core + nodes, then neoadjuvant chemo –Patients who remain path node positive after neo- adjuvant chemo (but negative by physical exam) –Randomized to completion ALND vs SNB alone –All patients have nodal radiation
 –Phase III –FNA or core + nodes, then neoadjuvant chemo –Patients who remain path node positive after neo- adjuvant chemo (but negative by physical exam) –Randomized to completion ALND vs SNB alone –All patients have nodal radiation")
35
Future Await final analysis of MA 20 and more mature results of AMAROS Proposed randomized trial for Canada: Patients having BCS with 1-2 positive SN’s (including itc’s, micro and macro mets) randomized to: WBI alone WBI plus RNI 1650 patients, followed for DFS
 randomized to: WBI alone WBI plus RNI 1650 patients, followed for DFS")
36
Conclusions/Summary Breast radiation after lumpectomy significantly reduces first recurrences (both local and distant) Should still be standard of care Exception may be Luminal A patients followed on a protocol Roughly 30% of patients with 1-2 positive sentinel nodes have additional positive nodes at completion ALND Despite this, regional recurrence rates are very low even when completion ALND omitted in the current era of systemic and radiation therapy
 Should still be standard of care Exception may be Luminal A patients followed on a protocol Roughly 30% of patients with 1-2 positive sentinel nodes have additional positive nodes at completion ALND Despite this, regional recurrence rates are very low even when completion ALND omitted in the current era of systemic and radiation therapy")
37
Conclusions/Summary Adding nodal radiation to breast/CW radiation results in fewer distant recurrences, improved DFS, with a small positive effect on OS The added toxicity from nodal radiation is small but needs to be discussed in the context of the benefits Future trials will inform us as to the best loco-regional treatment after neo-adjuvant chemotherapy

Similar presentations







>")






>")





