Download presentation
Presentation is loading. Please wait.

1
Dr. Mahmoud Abdel-Khalek
Airway Management Prepared by Dr. Mahmoud Abdel-Khalek

2
Introduction In order to ensure adequate oxygenation and ventilation throughout the insults of anesthesia and surgery, the anesthesiologist must take active measures to maintain the patency of the airway as well as ensuring its protection from aspiration

3
Airway Anatomy The airways can be divided into 2 parts namely:
The upper airway. The lower airway.

4
Anatomy of the Upper Airway
Airway structures above the vocal chords Larynx Divides upper and lower airways Pharynx Extends from the nose and mouth to the esophagus and trachea Nasopharynx Oropharynx Laryngopharynx

5
Upper and Lower Airway

6
Upper Airway

7
Anatomy of the Upper Airway

8
Oral Cavity Adenoids and tonsils may become swollen and infected may cause upper airway obstruction

9
Larynx Marks where the upper airway ends and lower airway begins
Thyroid cartilage Formed by two plates that form the laryngeal prominence (Adam’s apple) Cricoid cartilage is the first ring of the trachea Cricothyroid membrane: ligament between the thyroid and cricoid cartilage site for emergency surgical and nonsurgical access to the airway (cricothyrotomy)
 Cricoid cartilage is the first ring of the trachea. Cricothyroid membrane: ligament between the thyroid and cricoid cartilage site for emergency surgical and nonsurgical access to the airway (cricothyrotomy)")
10
Larynx Glottis: Space between the vocal cords Vallecula
Pocket between base of tongue and epiglottis Important landmark for ET intubation Arytenoid cartilages Posterior attachment of the vocal cords Valuable guides for ET intubation Laryngospasm: spasmodic closure of the vocal cords seals off the airway

11
Trachea Begins below the cricoid cartilage About 12cm length in adults
1st tracheal ring anterior to C6 Supported by C-shaped cartilages (open posteriorly; membranous aspect overlies esophagus Trachea ends at level of carina at T5 Divides into right and left mainstem bronchi Right mainstem bronchus larger in diameter and deviates at less acute angle than left (therefore aspiration or endobronchial intubation usu. to right side)
")
12
Routine airway management
Routine airway management associated with general anesthesia consists of: Airway assessment Preparation and equipment check Patient positioning Preoxygenation Bag and mask ventilation (BMV) Intubation (if indicated) Confirmation of endotracheal tube placement Intraoperative management and troubleshooting Extubation
 Intubation (if indicated) Confirmation of endotracheal tube placement. Intraoperative management and troubleshooting. Extubation.")
13
Airway Assessment: Mouth opening
An incisor distance of 3 cm or greater is desirable in an adult

14
Thyromental Distance: Thyromental distance
Thyromental distance: the distance between the mentum and the superior thyroid notch A distance greater than 3 fingerbreadths is desirable

15
Airway Assessment: Mallampati Classification
Examines the size of the tongue in relation to the oral cavity Large sized tongue obstructs the view of the pharyngeal structures and may add difficulty to intubation

16
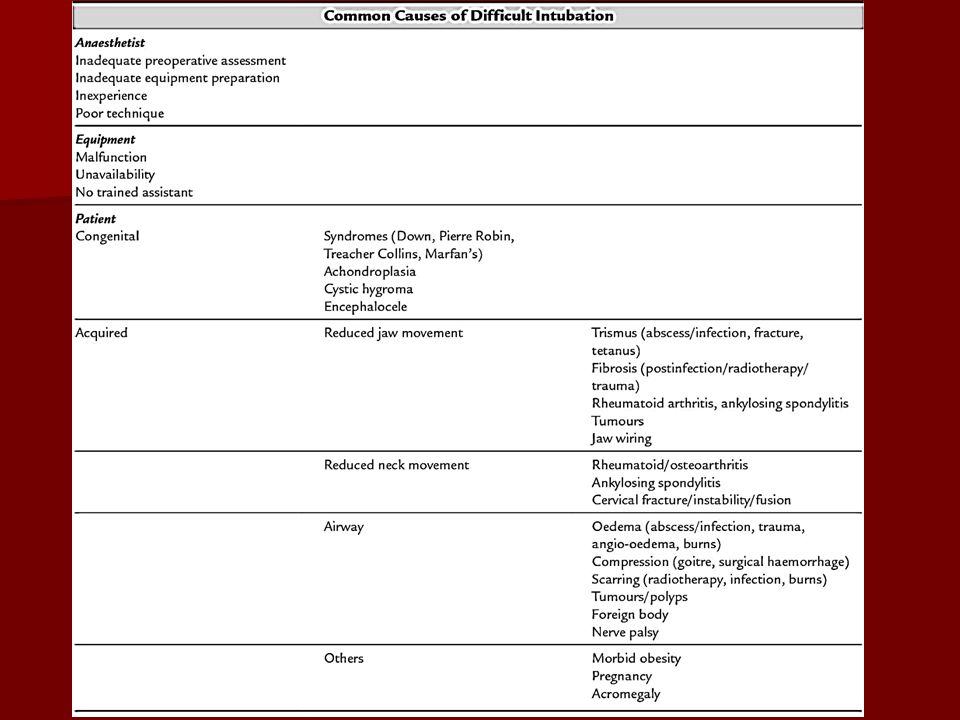
Conditions Associated with Difficult Intubation

17
Preparation and equipment check
Preparation is mandatory for all airway management scenarios The following equipment is routinely needed in airway management situations An oxygen source BMV capability Laryngoscopes (direct and video) Several endotracheal tubes of different sizes Other (not endotracheal tube) airway devices (e.g., oral, nasal airways) Suction Oximetry and CO2 detection Stethoscope Tape Blood pressure and ECG monitors Intravenous access
 Several endotracheal tubes of different sizes. Other (not endotracheal tube) airway devices (e.g., oral, nasal airways) Suction. Oximetry and CO2 detection. Stethoscope. Tape. Blood pressure and ECG monitors. Intravenous access.")
18
Preparation

19
Laryngoscopes

20
Oral artificial airway sizes
Correct size by measuring from corner of mouth to bottom of earlobe Adult oral airways typically come in small (80 mm [Guedel No. 3]), medium (90 mm [Guedel No. 4]), and large (100 mm [Guedel No. 5]) sizes.
, medium (90 mm [Guedel No. 4]), and large (100 mm [Guedel No. 5]) sizes.")
21
Endotracheal tubes

22
The face mask

23
Patient Positioning Relative alignment of the oral and
pharyngeal axes is achieved by having the patient in the “sniffing” position

24
Preoxygenation When possible, preoxygenation with face mask oxygen should precede all airway management interventions Oxygen is delivered by mask for several minutes prior to anesthetic induction. The FRC, the patient’s oxygen reserve, is purged of nitrogen. Up to 90% of the normal FRC of 2 L following preoxygenation is filled with O2 Considering the normal oxygen demand of 200–250 mL/min, the preoxygenated patient may have a 5–8 min oxygen reserve. Thus improving safety by allowing more time before desaturation in if ventilation following anesthetic induction is delayed. Conditions that increase oxygen demand (e.g., sepsis, pregnancy) and decrease FRC (e.g. morbid obesity, pregnancy) reduce the apneic period before desaturation ensues.
 and decrease FRC (e.g. morbid obesity, pregnancy) reduce the apneic period before desaturation ensues.")
25
The use of face mask In current practice the face mask is only used
In preoxygenation before tracheal intubation or insertion of the laryngeal mask During short non-invasive procedures, e.g. Orthopedic manipulations and dental anaesthesia

26
Technique of face mask selection of the correct fit is important to provide a gas-tight seal For children, a mask with excessive dead space should be avoided (Rebreathing) The mandible is held ‘into’ the mask by the anesthetist and forward to prevent obstruction of the airway by the tongue The importance of observation of the airway during mask anesthesia cannot be overemphasized Maintenance of the airway may be assisted further by the use of an oropharyngeal (Guedel) airway in anesthetized patients
 The mandible is held ‘into’ the mask by the anesthetist and forward to prevent obstruction of the airway by the tongue. The importance of observation of the airway during mask anesthesia cannot be overemphasized. Maintenance of the airway may be assisted further by the use of an oropharyngeal (Guedel) airway in anesthetized patients.")
27
Technique….

28
Disadvantages It “ties up” the anesthesiologist’s hands
It does not protect against aspiration or laryngospasm (closure of the cords in response to noxious stimuli at light planes of anesthesia) Upper airway obstruction may occur, particularly in obese patients or patients with very large tongues
 Upper airway obstruction may occur, particularly in obese patients or patients with very large tongues.")
29
Laryngeal Mask Airway (LMA)
LMA consists of a wide bore tube whose proximal end connects to a breathing circuit with a standard 15-mm connector, and whose distal end is attached to an elliptical cuff that can be inflated through a pilot tube. The deflated cuff is lubricated and inserted blindly into the hypopharynx so that, once inflated, the cuff forms a low-pressure seal around the entrance to the larynx. This requires anesthetic depth and muscle relaxation slightly greater than that required for the insertion of an oral airway.

30
Advantages and disadvantages

31
Indications Contraindications
To provide a clear airway without the need for the anesthetist’s hands to support a face mask. To avoid the use of tracheal intubation during spontaneous ventilation. In a case of unanticipated difficult intubation Contraindications ‘Full stomach’ A patient in whom the risk of regurgitation of gastric contents into the esophagus is increased (e.g. hiatus hernia). Oral operations as it may prevent surgical access
. Oral operations as it may prevent surgical access.")
32
Size selection& Technique

33
Technique of LMA insertion

34
Tracheal Intubation

35
ET tube Most commonly made of PVC
The shape and rigidity of TT’s can be altered by inserting a stylet The patient end of the tube is beveled to aid visualization and insertion through the vocal cords (the Murphy eye) to decrease the risk of occlusion Most adult TT’s have a cuff inflation system consisting of a valve, pilot balloon, inflating tube, and cuff
 to decrease the risk of occlusion. Most adult TT’s have a cuff inflation system consisting of a valve, pilot balloon, inflating tube, and cuff.")
36
Indications Provision of a clear airway, e.g. anticipated difficulty in using mask anesthesia in the edentulous patient An ‘unusual’ and prolonged position, e.g. prone or sitting. A reinforced non-kinking tube may be necessary. Operations on the head and neck, e.g. ENT, dental A nasotracheal tube may be required. Protection of the respiratory tract against aspiration e.g. from blood during upper respiratory tract or oral surgery and from inhalation of gastric contents in emergency surgery or patients with oesophageal obstruction. During anesthesia using IPPV and muscle relaxants To facilitate suction of the respiratory tract During thoracic operations

37
Contraindications for Intubation
Patients with an intact gag reflex Patients likely to react with laryngospasm to an intubation attempt. e.g. Children with epiglottitis Basilar skull fracture – avoid naso-tracheal intubation and nasogastric/pharyngeal tube.

39
Technique Position the patient supine, open the airway with a head-tilt chin-lift maneuver.(Suspected spinal injury, attempt naso-tracheal intubation, spine in neutral position.). Open mouth by separating the lips and pulling on upper jaw with the index finger. Hold laryngoscope in left hand, insert scope into mouth with blade directed to right tonsil.
. Open mouth by separating the lips and pulling on upper jaw with the index finger. Hold laryngoscope in left hand, insert scope into mouth with blade directed to right tonsil.")
40
Technique Once right tonsil is reached, sweep the blade to the midline keeping the tongue on the left. This brings the epiglottis into view.” DO NOT LOOSE SIGHT OF IT!” Advance the blade until it reaches the angle between the base of the tongue and epiglottis.( vallecular space) Lift the laryngoscope upwards and away from the nose – towards the chest. This should bring the vocal cords into view. It may be necessary for a colleague to press on the trachea to improve the view of the larynx.
 Lift the laryngoscope upwards and away from the nose – towards the chest. This should bring the vocal cords into view. It may be necessary for a colleague to press on the trachea to improve the view of the larynx.")
41
Technique Place the ETT in the right hand. Keep the concavity of the tube facing the right side of the mouth. Insert the tube watching it enter through the cords Insert the tube just so the cuff has passed the cords and then inflate the cuff. Listed for air entry at both apices and both axillae to ensure correct placement using a stethoscope.

42
Technique

43
Confirmation of Tube Placement
End Tidal Carbon Dioxide Monitor Stethoscope

44
Complications

45
Nasotracheal Intubation

46
Nasotracheal intubation
Advantages: Comfortable for prolong intubation in postoperative period Suitable for oral surgery : tonsillectomy , mandible surgery For blind nasal intubation Can take oral feeding Resist for kinking and difficult to accidental extubation Disadvantages Trauma to nasal mucosa Risk for sinusitis following prolonged intubation Risk of bacteremia Smaller diameter than oral route

47
Contraindication for nasoendotracheal intubation
Fracture base of skull Large adenoids Coagulopathy Nasal cavity obstruction Retropharyngeal abscess

49
Thank You

Similar presentations

















 ภาควิชาวิสัญญีวิทยา วิทยาลัยแพทยศาสตร์ กรุงเทพมหานครและวชิรพยาบาล.>")

