Download presentation
Presentation is loading. Please wait.

1
Cirrosi Epatica Definizione Meccanismi della fibrogenesi epatica
Fisiopatologia dell’ipertensione portale Complicanze maggiori della cirrosi Cenni di terapia delle complicanze Management della cirrosi compensata/scompensata

2
CIRROSI Alterazione dell’architettura del fegato caratterizzata da noduli e formazione di tessuto collagene CAUSE: Tutte le cause di danno epatico cronico

3
Progressione del danno epatico cronico
Causa iniziale Stadio finale Complicanze ● anni Fibrosi Distorsione dell’architettura epatica Cirrosi

4
Hepatic Artery Portal Vein Sinusoids Bile Duct Central Veins

5
Changes of hepatic microcirculation in cirrhosis
Normal Cirrhosis Changes of hepatic microcirculation in cirrhosis

6
Activation of HSC

7
LIVER CIRRHOSIS : from activation of HSC to cirrhotic nodules

8
– Necrosi a ponte porto-centrale
Fibrosi virale Spazio portale – Necrosi a ponte porto-centrale 2. – Epatite da interfaccia e sviluppo di setti che circondano il parechima 3. – Perdita di connessioni vascolari con il sistema portale

9
Formazione di setti porto-portali La vena centrolobulare è conservata
fibrosi biliare Spazio portale Modello BDL CBP CB secondaria CSP Formazione di setti porto-portali La vena centrolobulare è conservata

10
– Secondary to venous outflow problems (e.g. chronic heart failure)
Centrolobular fibrosis portal tract – Secondary to venous outflow problems (e.g. chronic heart failure) 2. - Chronic ETOH consumption 3. – Development of central to central septa and “reversed lobulation”
 2. - Chronic ETOH consumption. 3. – Development of central to central septa and reversed lobulation")
11
CONSEQUENCES OF DEVELOPING PROGRESSIVE HEPATIC FIBROSIS
structural & functional intrahepatic resistance splanchnic blood flow (cirrhosis) HCC systemic hyperdynamic circulation portal hypertension decrease central volume portosystemic collaterals variceal bleeding HRS ascites hepatic encephalopathy cardiac output cardiomyopathy spontaneous bacterial peritonitis hepatopulmonary syndrome
 HCC. systemic. hyperdynamic circulation. portal hypertension. decrease central. volume. portosystemic collaterals. variceal bleeding. HRS. ascites. hepatic encephalopathy. cardiac output. cardiomyopathy. spontaneous. bacterial peritonitis. hepatopulmonary syndrome.")
12
Ipertensione portale Condizione fisiopatologica causata dall’aumento della pressione venosa nel distretto portale Principale conseguenza della cirrosi epatica e principale meccanismo delle sue principali complicanze cliniche Riconosce anche cause extraepatiche, in cui le manifestazioni cliniche dominanti dipendono dalla sede di origine della ipertensione portale

13
Anatomia e Fisiologia della circolazione portale
Sistema venoso ad alta portata e bassa resistenza che drena il sangue dagli organi addominali per convogliarlo al fegato; da questo, attraverso i sinusoidi e le vene sovrepatiche, raggiunge la vena cava inferiore e la circolazione sistemica Flusso epatico: 1.5 l/min (80% venoso, portale) Pressione portale: 7 mmHg (diretta o wedge) Pressione sovra-epatiche/atrio dx: 3-5 mmHg Gradiente porto-epatico (HVPG): ≤5
 Pressione portale: 7 mmHg (diretta o wedge) Pressione sovra-epatiche/atrio dx: 3-5 mmHg. Gradiente porto-epatico (HVPG): ≤5.")
14
Classificazione e cause
Cause Pre-epatiche Trombosi portale Trombosi splenica Cause Intraepatiche Presinusoidali Sinusoidali Postsinusoidali Cause post-epatiche Membrana cavale Pericardite costrittiva Insufficienza tricuspidale Grave scompenso cardiaco destro

15
Cause di ipertensione portale intraepatica
Pre-sinusoidali Schistosomiasi, sarcoidosi, tossici, fibrosi epatica congenita, malattie mielo proliferative Sinusoidali o miste Cirrosi, epatite alcolica, iperplasia nodulare rigenerativa Post-sinusoidali Malattia veno-occlusiva Sindrome di Budd-Chiari

16
PORTAL HYPERTENSION: pathophysiological sequelae
structural & functional intrahepatic resistance splanchnic blood flow (cirrhosis) HCC systemic hyperdynamic circulation portal hypertension decrease central volume portosystemic collaterals variceal bleeding HRS ascites hepatic encephalopathy cardiac output cardiomyopathy spontaneous bacterial peritonitis hepatopulmonary syndrome
 HCC. systemic. hyperdynamic circulation. portal hypertension. decrease central. volume. portosystemic collaterals. variceal bleeding. HRS. ascites. hepatic encephalopathy. cardiac output. cardiomyopathy. spontaneous. bacterial peritonitis. hepatopulmonary syndrome.")
17
Conseguenze dell’ ipertensione portale
Splenomegalia ed ipersplenismo Circoli collaterali ed emorragie digestive Shunt porto-sistemici ed encefalopatia porto-sistemica Vasodilatazione splancnica ed alterazioni della emodinamica sistemica

18
Circoli collaterali Ligamento falciforme Gastro-esofagei
Parete addome e retro peritoneo Gastro-esofagei Vene emorroidarie

19
Conseguenze degli shunts portosistemici
Riducono il flusso portale Aumentano insufficienza epatica NON riducono significativamente la pressione portale Favoriscono la circolazione iperdinamica Favoriscono iperammoniemia Endotossinemia Encefalopatia porto sistemica

20
Complicanze maggiori della cirrosi

22
Complicanze maggiori della cirrosi

23
Natural History of Chronic Liver Disease Development of cirrhosis
Compensated cirrhosis Decompensated cirrhosis Death Orthotopic liver transplant (OLT) Development of complications: NATURAL HISTORY OF CHRONIC LIVER DISEASE – SUMMARY Variceal hemorrhage Ascites Encephalopathy HRS
 Development of complications: NATURAL HISTORY OF CHRONIC LIVER DISEASE – SUMMARY. Variceal hemorrhage. Ascites. Encephalopathy. HRS.")
24
Mortalità per complicanze di cirrosi epatica - 384 Pts
follow-up: 5 anni Fattovich G et al, Gastroenterology 1997;112:463

25
Child-Turcotte-Pugh (CTP) Score
Points 1 2 3 Encephalopathy None Grade 1-2 Grade 3-4 (precipitant) (chronic) Ascites None Mild Moderate Bilirubin (mg/dl) < >3 Albumin (g/dl) > <2.8 PT (seconds prolonged) < >6 or INR < >2.3 CHILD-TURCOTTE-PUGH (CTP) SCORE The CTP (or Child) score is based on five parameters: encephalopathy, ascites, bilirubin, albumin and prothrombin time. Each parameter is graded from 1 to 3, therefore the minimal score is 5 and the maximal score is 15. Patients can be listed for liver transplantation if they meet minimal listing criteria, that is, a Child-Pugh-Turcotte score of 7. Child A: 5-6 pts Child B: 7-9 pts Child C: pts MINIMAL LISTING CRITERIA: CTP SCORE 7 POINTS
 (chronic) Ascites None Mild Moderate. Bilirubin (mg/dl) <2 2-3 >3. Albumin (g/dl) > <2.8. PT (seconds prolonged) <4 4-6 >6. or INR < >2.3. CHILD-TURCOTTE-PUGH (CTP) SCORE. The CTP (or Child) score is based on five parameters: encephalopathy, ascites, bilirubin, albumin and prothrombin time. Each parameter is graded from 1 to 3, therefore the minimal score is 5 and the maximal score is 15. Patients can be listed for liver transplantation if they meet minimal listing criteria, that is, a Child-Pugh-Turcotte score of 7. Child A: 5-6 pts Child B: 7-9 pts Child C: pts. MINIMAL LISTING CRITERIA: CTP SCORE 7 POINTS.")
26
MELD (Model for End-Stage Liver Disease)
Predicts 3-month mortality among patients with chronic liver disease on the liver waiting list MELD = (0.957 x LN (creatinine) x LN (bilirubin) x LN (INR) ) x 10 Minimum score = 6 (risk of death on WL 20%) Maximum score = 40 (risk of death on WL 100%)
 x LN (bilirubin) x LN (INR) ) x 10. Minimum score = 6 (risk of death on WL 20%) Maximum score = 40 (risk of death on WL 100%)")
27
Diagnostica della cirrosi con ipertensione portale
Clinico-semeiologica Misurazione invasiva emodinamica portale Eco-doppler Endoscopia digestiva

28
Diagnosi clinico-semeiologica
Splenomegalia Circoli collaterali superficiali Gavoccioli emorroidari Spider Naevi Edema perimalleolare Ascite Asterixis

29
Semeiotica dell’ipertensione portale

33
Definition of ascites Uncomplicated
Grade 1 (mild) detectable only by US Grade 2 (moderate) moderate symmetrical abdominal distension Grade 3 (large) marked abdominal distension Refractory Ascites that cannot be mobilized or early recurrence of ascites not prevented by medical therapy Diuretic-resistant Diuretic-intractable
 detectable only by US. Grade 2 (moderate) moderate symmetrical abdominal distension. Grade 3 (large) marked abdominal distension. Refractory. Ascites that cannot be mobilized or early recurrence of ascites not prevented by medical therapy. Diuretic-resistant. Diuretic-intractable.")
35
Treatment of Ascites Bed rest unproven benefit
Dietary sodium restriction to 5.2 g/d (90 mmol) Diuretics Anti-Mineralocorticoids Spironolactone, Canrenoate, Canrenone Loop diuretics Furosemide, Torasemide, Ethacrynic Acid Other potassium-sparing diuretics Amiloride, Triamterene
 Diuretics. Anti-Mineralocorticoids Spironolactone, Canrenoate, Canrenone. Loop diuretics Furosemide, Torasemide, Ethacrynic Acid. Other potassium-sparing diuretics Amiloride, Triamterene.")
36
Diagnostic Criteria of Refractory Ascites
Treatment duration Intensive diuretic therapy (spironolactone 400 mg/d + furosemide 160 mg/d) for at least 1 wk Salt-restricted diet (< 90 mmol or 5.2 g of salt/d) Lack of response Weight loss < 0.8 kg over 4 days Urinary sodium output < sodium intake Early ascites recurrence Grade 2 or 3 ascites within 4 wks of initial mobilization Diuretic-induced complications Hepatic Encephalopathy, Renal Impairment, Hyponatremia, Hypo/Hyperkalemia
 for at least 1 wk. Salt-restricted diet (< 90 mmol or 5.2 g of salt/d) Lack of response. Weight loss < 0.8 kg over 4 days. Urinary sodium output < sodium intake. Early ascites recurrence. Grade 2 or 3 ascites within 4 wks of initial mobilization. Diuretic-induced complications. Hepatic Encephalopathy, Renal Impairment, Hyponatremia, Hypo/Hyperkalemia.")
37
PERITONITE BATTERICA SPONTANEA: definizione ed epidemiologia
Infezione del liquido ascitico PMN > 250/mm3 e colturale + su liquido ascitico Microbiologia: G-: E. Coli, K. Pneumoniae (60%) G+: Strepto (25%) Anaerobi: rari Non evidente sorgente di infezione addominale trattabile chirurgicamente 10-25% dei cirrotici ospedalizzati con ascite Mortalità elevata (17-50%) Alto rischio di recurrence: 43-70% (6-12 mesi)
 G+: Strepto (25%) Anaerobi: rari. Non evidente sorgente di infezione addominale trattabile chirurgicamente % dei cirrotici ospedalizzati con ascite. Mortalità elevata (17-50%) Alto rischio di recurrence: 43-70% (6-12 mesi)")
38
PERITONITE BATTERICA SPONTANEA: forme cliniche
Classic CNNA (culture negative neutrocytic ascites) MNB (monomicrobial non-neutrocytic bacterascites) carcinosi peritoneale, pancreatite, peritonite TBC Classica CNNA MNB PMN > 250 < 250 Colturale + -
 MNB (monomicrobial non-neutrocytic bacterascites) carcinosi peritoneale, pancreatite, peritonite TBC. Classica. CNNA. MNB. PMN. > 250. < 250. Colturale. + -")
39
PERITONITE BATTERICA SPONTANEA: terapia e profilassi
Cefotaxime: 2g/12 hrs per 5-10 gg Ciprofloxacina: 400 mg/12 hrs per 5 gg, poi orale Se non risposta: Stafilo? + Albumina: 1.5 g/kg alla diagnosi, 1 g/kg dopo 48 hrs (prevenire HRS!) Chinolonico long-term (Norfloxacina 400 mg/die) soprattutto se proteine < 1 g/dl nel liquido ascitico
 Chinolonico long-term (Norfloxacina 400 mg/die) soprattutto se proteine < 1 g/dl nel liquido ascitico.")
41
Definition of Hepatorenal Syndrome (HRS)
Type I HRS Rapid and progressive renal failure with a doubling of serum creatinine to a level greater than 2.5 mg/dl or a halving of the creatinine clearance to less than 20 ml/min in less than 2 wks Type II HRS More chronic form with a slowly progressive increase in serum creatinine level to greater than 1.5 mg/dl or a creatinine clearance of less than 40 ml/min

42
DIFFERENCES BETWEEN TYPE-1 AND TYPE-2 HRS
Renal failure Type-2 Type-1 Consequence Survival Moderate and steady Refractory ascites Months Severe and progressive Terminal hepatorenal failure Days Spontaneous Precipitated Onset

43
Definition of Hepatorenal Syndrome: Major Criteria
Chronic or acute liver disease with liver failure and portal hypertension Low glomerular filtration rate (serum creatinine > 1.5 mg/dl or creatinine clearance < 40 ml/min) Absence of shock, excessive fluid loss, ongoing bacterial infection and recent treatment with nephrotoxic drugs No sustained improvement in renal function following expansion with 1.5 l of isotonic saline Proteinuria < 0.5 g/dl No US evidence of renal tract disease
 Absence of shock, excessive fluid loss, ongoing bacterial infection and recent treatment with nephrotoxic drugs. No sustained improvement in renal function following expansion with 1.5 l of isotonic saline. Proteinuria < 0.5 g/dl. No US evidence of renal tract disease.")
44
Definition of Hepatorenal Syndrome: Minor Criteria
Urine volume < 500 ml/d Urine sodium < 10 mmol/d Urine osmolality < plasma osmolality Urine red cell count < 50/high power field Serum sodium < 130 mmol/l

45
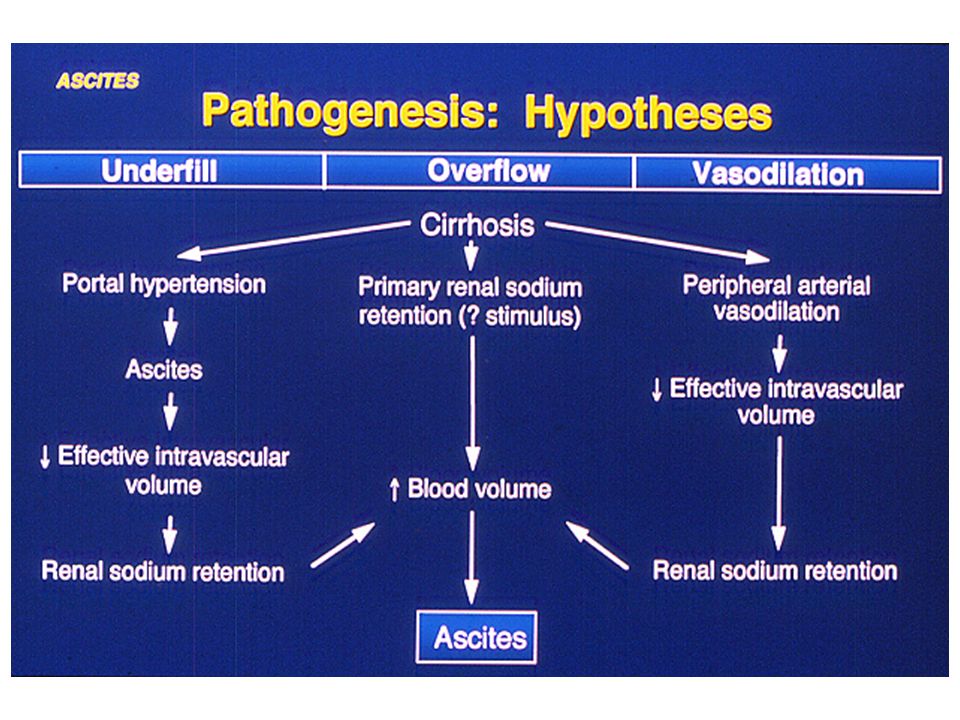
The Pathophysiology of HRS

47
Diagnosi e classificazione endoscopica
Varici esofagee Varici fondo

48
Diagnosi e classificazione endoscopica
Gastropatia ipertensiva GAVE

49
Dilation and Rupture of Varices
Varix P Flow Recently, we and others have suggested that changes in portal pressure associated with daily activities may contribute to the proggesive dilatation that precedes the rupture of the varices. This is because meals and alcoholic beverages cause brisk increases in portal pressure and blood flow, due to the postprandial hyperemia. Similarly, portal pressure increases markedly by even mild exercise and by activities increasing the intra-abdominal pressure. These repeat bumps in portal pressure cause acute incremets of variceal size, contributing to its proggresive dilatation, coming closer to the lighting point for the explosion of the varices. Risk increases in portal pressure and collateral blood flow caused by: Meals Alcohol Exercise Increased intra-abdominal pressure

50
Acute variceal bleeding Sclerotherapy + Drugs vs Sclerotherapy alone Mortality

51
PREVENZIONE RISANGUINAMENTO (profilassi secondaria)
BB + nitrati fallimento LEV(+ BB) successo fallimento successo continuare Malattia epatica avanzata Malattia epatica stabile Continuare + follow up TIPS OLT TIPS (DSSR) D´Amico, 2004
 successo. fallimento. successo. continuare. Malattia epatica. avanzata. Malattia epatica. stabile. Continuare. + follow up. TIPS. OLT. TIPS (DSSR) D´Amico,")
52
HEPATIC ENCEPHALOPATHY – NOMENCLATURE
Type A Associated with Acute liver failure Type B Associated with porto-systemic Bypass without intrinsic hepatocellular disease Type C Associated with Cirrhosis and porto-systemic shunting Slide 346 HEPATIC ENCEPHALOPATHY – NOMENCLATURE Hepatic encephalopathy is subdivided into type A associated with acute liver failure, type B associated with portosystemic bypass without intrinsic hepatocellular disease (portosystemic shunts), and type C when associated with cirrhosis and portosystemic shunting. Ferenci et al., Hepatology 2002; 35:716 Ferenci et al., Hepatology 2002; 35:716
, and type C when associated with cirrhosis and portosystemic shunting. Ferenci et al., Hepatology 2002; 35:716. Ferenci et al., Hepatology 2002; 35:716.")
53
Encephalopathy of acute liver failure (Type A)
Rapid deterioration in the level of consciousness Increased intracranial pressure (ICP) Reduced cerebral perfusion pressure Neuropathologically, there is brain edema Pathogenesis is multifactorial with ammonia playing a major role
 Reduced cerebral perfusion pressure. Neuropathologically, there is brain edema. Pathogenesis is multifactorial with ammonia playing a major role.")
54
TYPE C HEPATIC ENCEPHALOPATHY IS THE ENCEPHALOPATHY OF CIRRHOSIS
Neuropsychiatric complication of cirrhosis Results from spontaneous or surgical / radiological portal-systemic shunt + chronic liver failure Failure to metabolize neurotoxic substances Alterations of astrocyte morphology and function (Alzheimer type II astrocytosis) Slide 348 TYPE C HEPATIC ENCEPHALOPATHY IS THE ENCEPHALOPATHY OF CIRRHOSIS In cirrhosis, hepatic encephalopathy results from a combination of portosystemic shunting and failure to metabolize neurotoxic substances. Astrocytes are the only cells in the brain that can metabolize ammonia and, in hepatic encephalopathy, changes in the astrocytes are seen (Alzheimer’s type II astrocytosis).
 Slide 348. TYPE C HEPATIC ENCEPHALOPATHY IS THE ENCEPHALOPATHY OF CIRRHOSIS. In cirrhosis, hepatic encephalopathy results from a combination of portosystemic shunting and failure to metabolize neurotoxic substances. Astrocytes are the only cells in the brain that can metabolize ammonia and, in hepatic encephalopathy, changes in the astrocytes are seen (Alzheimer’s type II astrocytosis).")
55
CHARACTERISTICS OF TYPE A VS. TYPE C ENCEPHALOPATHY
Characteristics of Type A vs. Type C Hepatic Encephalopathy Type A Type C Rapid onset Frequently fatal Main cause: cerebral edema Gradual onset Rarely fatal Main cause: shunting / toxin Precipitant Treatment: usually effective Slide 347 CHARACTERISTICS OF TYPE A VS. TYPE C ENCEPHALOPATHY Type A hepatic encephalopathy is of rapid onset, frequently fatal, and related to cerebral edema. Liver transplantation is the most effective treatment. Type C is of gradual onset, rarely fatal, and is caused by porto-systemic shunting. A precipitating cause can often be found and treatment is usually effective. Treatment: rarely effective short of liver transplant

56
PATHOPHYSIOLOGY OF HEPATIC ENCEPHALOPATHY
Ammonia Upregulation of astrocytic peripheral benzodiazepine receptors (PBR) Neurosteroid production Modulation of GABAA receptor Hepatic encephalopathy Slide 349 PATHOPHYSIOLOGY OF HEPATIC ENCEPHALOPATHY Ammonia, which crosses the blood-brain barrier, results in up-regulation of astrocytic peripheral-type benzodiazepine receptors which are the most potent stimulants of neurosteroid production. Neurosteroids are the major modulators of GABA, which results in cortical depression and hepatic encephalopathy.
 Neurosteroid production. Modulation of GABAA receptor. Hepatic encephalopathy. Slide 349. PATHOPHYSIOLOGY OF HEPATIC ENCEPHALOPATHY. Ammonia, which crosses the blood-brain barrier, results in up-regulation of astrocytic peripheral-type benzodiazepine receptors which are the most potent stimulants of neurosteroid production. Neurosteroids are the major modulators of GABA, which results in cortical depression and hepatic encephalopathy.")
57
PATHOPHYSIOLOGY OF HEPATIC ENCEPHALOPATHY
Hepatic Encephalopathy Pathogenesis Toxins NH3 Shunting Failure to metabolize NH3 GABA-BD receptors Slide 350 PATHOPHYSIOLOGY OF HEPATIC ENCEPHALOPATHY This slide demonstrates how ammonia bypasses the liver, either through porto-systemic collaterals or through a created shunt (transjugular intrahepatic porto-systemic shunt) and ultimately reaches the brain. Bacterial action Protein load
 and ultimately reaches the brain. Bacterial action. Protein load.")
58
Pathogenesis of Hepatic Encephalopathy: role of GABA-BD receptors

59
HEPATIC ENCEPHALOPATHY IS A CLINICAL DIAGNOSIS
Clinical findings and history important Ammonia levels are unreliable Ammonia has poor correlation with diagnosis Measurement of ammonia not necessary Number connection test Slow dominant rhythm on EEG Slide 351 HEPATIC ENCEPHALOPATHY IS A CLINICAL DIAGNOSIS. The diagnosis of hepatic encephalopathy is based on history and physical exam findings. Ammonia levels are unreliable, and there is a poor correlation between the stage of encephalopathy and blood level of ammonia. Therefore, measurements of ammonia are not necessary. Psychometric tests such as the number connection test and the EEG are typically used in research studies and not for clinical diagnosis.

60
STAGES OF HEPATIC ENCEPHALOPATHY
Stage Mental state Neurologic signs 1 Mild confusion: limited attention Incoordination, tremor, span, irritability, inverted sleep impaired handwriting pattern 2 Drowsiness, personality changes, Asterixis, ataxia, intermittent disorientation dysarthria 3 Somnolent, gross disorientation, Hyperreflexia, muscle marked confusion, slurred speech rigidity, Babinski sign 4 Coma No response to pain, decerebrate posture Slide 352 STAGES OF HEPATIC ENCEPHALOPATHY These clinical stages of hepatic encephalopathy depend on the mental state and neurological signs.

61
Severity of Hepatic Encephalopathy
Poor Correlation of Ammonia Levels With Presence or Severity of Encephalopathy 400 350 300 250 Venous total ammonia mmol/L 200 150 POOR CORRELATION OF AMMONIA LEVELS WITH PRESENCE OR SEVERITY OF HEPATIC ENCEPHALOPATHY This slide demonstrates the poor correlation between the severity of hepatic encephalopathy and venous ammonia levels. Patients with grade 0 encephalopathy (i.e. no encephalopathy) have ammonia levels that overlap with those with overt encephalopathy stages 1-3. It would be reasonable to obtain ammonia levels in patients admitted with coma (stage 4) of unknown etiology. 100 50 Grade 0 Grade 1 Grade 2 Grade 3 Grade 4 Severity of Hepatic Encephalopathy Ong et al., Am J Med 2003; 114:188
 have ammonia levels that overlap with those with overt encephalopathy stages 1-3. It would be reasonable to obtain ammonia levels in patients admitted with coma (stage 4) of unknown etiology Grade 0. Grade 1. Grade 2. Grade 3. Grade 4. Severity of Hepatic Encephalopathy. Ong et al., Am J Med 2003; 114:188.")
62
BLOOD AMMONIA LEVELS ONLY LEAD TO CONFUSION
“Blood ammonia levels cause as much confusion in those requesting the measurement as in the patients in whom they are being measured” Slide 356 BLOOD AMMONIA LEVELS ONLY LEAD TO CONFUSION Adrian Reuben Hepatology 2002;35:983

63
MINIMAL HEPATIC ENCEPHALOPATHY
Occurs in 30-70% of cirrhotic patients without overt hepatic encephalopathy Detected by psychometric and neuro- psychological testing May improve with lactulose or synbiotics (probiotics and fermentable fiber) Predicts overt encephalopathy Slide 359 MINIMAL HEPATIC ENCEPHALOPATHY Minimal hepatic encephalopathy (formerly called “sub-clinical” hepatic encephalopathy) occurs in about 30-70% of patients with cirrhosis without overt hepatic encephalopathy. Minimal hepatic encephalopathy is detected by psychometric and neuropsychological testing alone. Minimal HE may improve with lactulose or synbiotics.
 Predicts overt encephalopathy. Slide 359. MINIMAL HEPATIC ENCEPHALOPATHY. Minimal hepatic encephalopathy (formerly called sub-clinical hepatic encephalopathy) occurs in about 30-70% of patients with cirrhosis without overt hepatic encephalopathy. Minimal hepatic encephalopathy is detected by psychometric and neuropsychological testing alone. Minimal HE may improve with lactulose or synbiotics.")
64
TREATMENT OF HEPATIC ENCEPHALOPATHY
Identify and treat precipitating factor Infection GI hemorrhage Prerenal azotemia Sedatives Constipation Lactulose (adjust to 2-3 bowel movements/day) Protein restriction, short-term (if at all) Slide 361 TREATMENT OF HEPATIC ENCEPHALOPATHY Treatment of hepatic encephalopathy involves 1) identifying and treating the precipitating factor, and 2) using lactulose adjusted to produce 2-3 bowel movements per day. Protein restriction is carried out typically when patients have stage 4 hepatic encephalopathy, but may not be necessary. Long-term protein restriction is not required. A vegetable protein diet is better tolerated than an animal protein diet.
 Protein restriction, short-term (if at all) Slide 361. TREATMENT OF HEPATIC ENCEPHALOPATHY. Treatment of hepatic encephalopathy involves 1) identifying and treating the precipitating factor, and 2) using lactulose adjusted to produce 2-3 bowel movements per day. Protein restriction is carried out typically when patients have stage 4 hepatic encephalopathy, but may not be necessary. Long-term protein restriction is not required. A vegetable protein diet is better tolerated than an animal protein diet.")
65
Actions of Lactulose NH3 Decreased pH NH4+ Lactic acid NH3 Lactulose
Slide 363 ACTIONS OF LACTULOSE Lactulose acts by several mechanisms. The acidic pH decreases urease-producing bacteria which produce ammonia. The proton H+ produced combines with NH3 to give NH4, which is non-absorbable, and results in ammonia excretion in stool. The cathartic effect of lactulose is also helpful. It is important to note that data supporting the benefit of lactulose in hepatic encephalopathy are lacking. Urease-producing bacteria Increase cathartic effect

66
PROTEIN RESTRICTION IS NOT NECESSARY IN HEPATIC ENCEPHALOPATHY
4 Hypoproteic diet Normoproteic diet 3 2 Hepatic encephalopathy stage 1 Slide 364 PROTEIN RESTRICTION IS NOT NECESSARY IN HEPATIC ENCEPHALOPATHY In a double-blind, placebo-controlled study performed in 30 patients with acute hepatic encephalopathy, patients were randomized to a normoproteic diet (yellow line) or a hypoproteic diet (blue line). Otherwise, treatment of encephalopathy was routine in both groups. As shown in the slide, there were no differences in the course of hepatic encephalopathy between study groups. Therefore, the study concludes that protein restriction is not necessary in the management of hepatic encephalopathy. Córdoba et al. J Hepatol 2004; 91:38 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Day Córdoba, J Hepatology 2004; 91:38
 or a hypoproteic diet (blue line). Otherwise, treatment of encephalopathy was routine in both groups. As shown in the slide, there were no differences in the course of hepatic encephalopathy between study groups. Therefore, the study concludes that protein restriction is not necessary in the management of hepatic encephalopathy. Córdoba et al. J Hepatol 2004; 91: Day. Córdoba, J Hepatology 2004; 91:38.")
67
Treatment Recommendations - Cirrhosis
Compensated Decompensated Hepatoma Surveillance U/S, AFP q 6 months Varices Surveillance Monitor Liver Function PT, Alb, Bili q 3-6 months Variceal Bleed SBP Ascites HRS Encephalopathy (Garcia-Tsao G, 2003)
")
68
Management of cirrhosis
Maintain nutrition/reduce salt intake Prevent bone loss Prevent bleeding Prevent encephalopathy High index suspicion for sepsis Close control diabetes Management of complications Early diagnosis and therapy of HCC (Selected antiviral therapy) Appropriate referral to transplant centres
 Appropriate referral to transplant centres.")
69
Natural History of Cirrhosis in 2008: Altered by What We Do
More aggressive screening HCC identified earlier Ablative therapies for HCC (down-staging) Obliteration of varices/beta-blockade TIPSS Liver Transplantation
 Obliteration of varices/beta-blockade. TIPSS. Liver Transplantation.")
71
HEPATIC ENCEPHALOPATHY – TREATMENT SUMMARY
Increase ammonia fixation in liver: Ornithine aspartate Benzoate Shunt occlusion or reduction Slide 365 HEPATIC ENCEPHALOPATHY – TREATMENT SUMMARY Hepatic encephalopathy can be treated with agents aimed at decreasing ammonia production in the gut. This strategy includes lactulose or non-absorbable antibiotics such as neomycin, metronidazole, or rifaximin. Change in dietary protein from an animal source to a vegetable source may also be beneficial. L-ornithine L-aspartate and benzoate may increase ammonia fixation in the liver. In patients who have a large portosystemic shunt in the absence of liver disease, occlusion of the shunt may be carried out. Decrease ammonia production in gut: Lactulose Antibiotics Adjustment in dietary protein

72
Liver Transplant Indications Contraindications
Decompensated cirrhosis - all causes (hepatitis C most common indication) Intrahepatic malignancy Acute liver failure Metabolic disease Extrahepatic malignancy Active infection Active substance abuse Advanced cardiopulmon-ary disease Extensive portal venous thrombosis LIVER TRANSPLANT – INDICATIONS AND CONTRAINDICATIONS Indications for liver transplantation include cirrhosis of the liver of all causes, intrahepatic malignancy (such as hepatocellular carcinoma), acute liver failure, and metabolic disease such as Wilson’s disease and oxalosis. Extrahepatic malignancy, active infection, substance abuse, cholangiocarcinoma, and non-hepatic comorbidity may be contraindications to transplantation.
 Intrahepatic malignancy. Acute liver failure. Metabolic disease. Extrahepatic malignancy. Active infection. Active substance abuse. Advanced cardiopulmon-ary disease. Extensive portal venous thrombosis. LIVER TRANSPLANT – INDICATIONS AND CONTRAINDICATIONS. Indications for liver transplantation include cirrhosis of the liver of all causes, intrahepatic malignancy (such as hepatocellular carcinoma), acute liver failure, and metabolic disease such as Wilson’s disease and oxalosis. Extrahepatic malignancy, active infection, substance abuse, cholangiocarcinoma, and non-hepatic comorbidity may be contraindications to transplantation.")
74
Child score and survival in 424 patients
1.0 CPT - A .8 .6 CPT - B .4 CPT - C .2 Cum Survival 0.0 200 400 600 800 1000 1200 1400 1600 OLT 1-yr survival OLT 2-yr survival Days Heumann et al

75
MELD and Survival on Transplant Waiting List Probability of survival
100 92.3% 90.7% <15 80 60 66.0% Probability of survival (%) 40 33.8% 30+ MELD AND SURVIVAL ON TRANSPLANT WAITING LIST This slide demonstrates the relationship between MELD score and risk for 3-month mortality while on the transplant waiting list. The higher the MELD score, the higher the mortality. 20 2 4 6 8 10 12 Months from listing
 % 30+ MELD AND SURVIVAL ON TRANSPLANT WAITING LIST. This slide demonstrates the relationship between MELD score and risk for 3-month mortality while on the transplant waiting list. The higher the MELD score, the higher the mortality Months from listing.")
76
Organ Allocation for Liver Transplant
Fulminant hepatic failure has highest priority MELD score determines priority in cirrhosis Amongst patients with same blood type, highest MELD score determines priority Waiting time used only to break ties with identical MELD scores MELD scores are updated at regular intervals ORGAN ALLOCATION FOR LIVER TRANSPLANT Within each UNOS region, patients with fulminant hepatic failure have the highest priority. In patients with cirrhosis, the MELD score determines the priority. Among patients with the same blood type, the patient with the highest MELD score gets the priority. Waiting times are used only to break ties when patients have identical MELD scores. MELD scores are updated at regular intervals.

77
United Network for Organ Sharing (UNOS) Regions
1 6 7 9 2 10 8 11 5 UNOS REGIONS There are 11 regions within the United States for organ allocation under the United Network of Organ Sharing (UNOS). 3 4
")
78
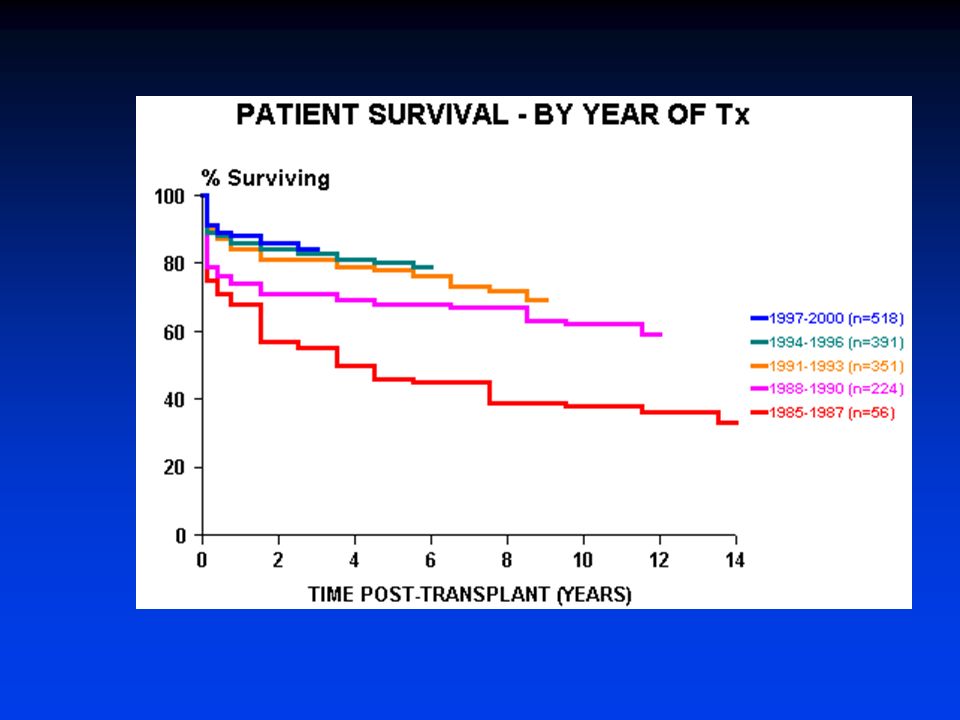
Liver Transplantation in the U.S.
Current 1- and 3-year survival rates are 90% and 80%, respectively During 2005, ~6,000 liver transplantations were performed During 2005, ~17,000 patients were on the waiting list and ~2,000 died on it or were removed from it because they became too sick for transplant Main problem is the shortage of donors Expansion of donor pool: marginal livers, split-livers, live donors

79
NATURAL HISTORY OF CHRONIC LIVER DISEASE – SUMMARY
Development of cirrhosis Chronic liver disease Compensated cirrhosis Decompensated cirrhosis Death Median survival ~ 9 years Median survival ~ 1.6 years Development of complications: Slide 410 NATURAL HISTORY OF CHRONIC LIVER DISEASE – SUMMARY Orthotopic liver transplant (OLT) Variceal hemorrhage Ascites Encephalopathy Jaundice
 Variceal hemorrhage. Ascites. Encephalopathy. Jaundice.")
80
MANAGEMENT OF COMPENSATED CIRRHOSIS – SUMMARY
Chronic liver disease Compensated cirrhosis Decompensated cirrhosis Death Diagnosis: Liver biopsy Clinical/LSS Screen for varices (EGD): Orthotopic liver transplant (OLT) Large varices beta-blockers Small varices EGD in 1-2 yrs No varices EGD in 2-3 yrs Slide 411 MANAGEMENT OF COMPENSATED CIRRHOSIS – SUMMARY Screen for HCC: Ultrasound and AFP q 6 mos Measures to stop alcohol use Hep A and B vaccination
: Orthotopic liver. transplant (OLT) Large varices beta-blockers. Small varices EGD in 1-2 yrs. No varices EGD in 2-3 yrs. Slide 411. MANAGEMENT OF COMPENSATED CIRRHOSIS – SUMMARY. Screen for HCC: Ultrasound and AFP q 6 mos. Measures to stop alcohol use. Hep A and B vaccination.")
81
MANAGEMENT OF ASCITES – SUMMARY
Chronic liver disease Compensated cirrhosis Decompensated cirrhosis Death Ascites Diagnosis: Clinical US or CAT scan Orthotopic liver transplant (OLT) Treatment: Slide 412 MANAGEMENT OF ASCITES – SUMMARY Spironolactone-based No NSAIDs Early diagnosis of SBP: Paracentesis q admission or with symptoms No aminoglycosides in SBP
 Treatment: Slide 412. MANAGEMENT OF ASCITES – SUMMARY. Spironolactone-based. No NSAIDs. Early diagnosis of SBP: Paracentesis q admission. or with symptoms. No aminoglycosides in SBP.")
82
MANAGEMENT OF VARICEAL BLEEDING – SUMMARY
Chronic liver disease Compensated cirrhosis Decompensated cirrhosis Death Variceal Bleed Diagnosis / Treatment: Endoscopy within 12 hrs Orthotopic liver transplant (OLT) Other Treatment: Slide 413 MANAGEMENT OF VARICEAL BLEEDING – SUMMARY Prophylactic antibiotics Prophylaxis of rebleed: Beta-blockers prior to d/c or Serial ligation post d/c
 Other Treatment: Slide 413. MANAGEMENT OF VARICEAL BLEEDING – SUMMARY. Prophylactic antibiotics. Prophylaxis of rebleed: Beta-blockers prior to d/c or. Serial ligation post d/c.")
83
MANAGEMENT OF HEPATIC ENCEPHALOPATHY - SUMMARY
Management of Encephalopathy Chronic liver disease Compensated cirrhosis Decompensated cirrhosis Death Encephalopathy Diagnosis Clinical Orthotopic liver transplant (OLT) Treatment: D/C diuretics D/C sedatives Dx paracentesis Slide 414 MANAGEMENT OF HEPATIC ENCEPHALOPATHY - SUMMARY No long-term protein restriction
 Treatment: D/C diuretics. D/C sedatives. Dx paracentesis. Slide 414. MANAGEMENT OF HEPATIC ENCEPHALOPATHY - SUMMARY. No long-term protein restriction.")
85
Cenni di terapia dell’ipertensione portale
Farmaci antifibrotici: una promessa ancora non mantenuta L’unica terapia in grado di modificare la progressione è, al momento, il trattamento del fattore etiologico di base (es no Et-OH) Il target della terapia è quello di ridurre, farmacologicamente o “chirurgicamente” il gradiente venoso porto-epatico L’end-point clinico è la prevenzione primaria o secondaria del sanguinamento da varici
 Il target della terapia è quello di ridurre, farmacologicamente o chirurgicamente il gradiente venoso porto-epatico. L’end-point clinico è la prevenzione primaria o secondaria del sanguinamento da varici.")
86
Terapia dell’ipertensione portale
Vasocostrittori arteriolari splancnici Beta bloccanti non selettivi Vasopressina ed analoghi Somatostatina ed analoghi Terapia Endoscopica Scleroterapia Legatura Terapia Chirurgica H shunt (mesocavale) Splenorenale distale TIPS
 Splenorenale distale. TIPS.")
87
Mediatori vasoattivi nella ipertensione portale
VASODILATATORI Glucagone Prostaciclina Adenosina Fattore Natriuretico Atriale VIP Endotossine TNF NO VASOCOSTRITTORI Norepinefrina Serotonina Endotelina Angiotensina II Vasopressina

88
Treatment of ascites: Grade 1 Ascites
No specific treatment, only reduction of dietary sodium intake

89
Treatment of ascites: Grade 2 Ascites
Bed rest unproven benefit Dietary sodium restriction to 5.2 g/d (90 mmol) Diuretics Anti-Mineralocorticoids Spironolactone, Canrenoate, Canrenone Loop diuretics Furosemide, Torasemide, Ethacrynic Acid Other potassium-sparing diuretics Amiloride, Triamterene
 Diuretics. Anti-Mineralocorticoids Spironolactone, Canrenoate, Canrenone. Loop diuretics Furosemide, Torasemide, Ethacrynic Acid. Other potassium-sparing diuretics Amiloride, Triamterene.")
90
Treatment of ascites: use of Diuretics in Grade 2 Ascites
Spironolactone: alone at first, mg/d once Adequate response: weight loss = kg/d (1 kg/d if peripheral edema) If not adequate response: stepwise increase If failure to spironolactone 200 mg/d after 2-3 wks: + Furosemide (20-40 mg/d) If failure: maximal doses of spironolactone 400 mg/d + furosemide 160 mg/d Canrenoate, Amiloride (5-30 mg/d), or Torasemide may be used alternatively
 If not adequate response: stepwise increase. If failure to spironolactone 200 mg/d after 2-3 wks: + Furosemide (20-40 mg/d) If failure: maximal doses of spironolactone 400 mg/d + furosemide 160 mg/d. Canrenoate, Amiloride (5-30 mg/d), or Torasemide may be used alternatively.")
91
Treatment of ascites: Complications of diuretic therapy
Electrolyte imbalance (hyponatremia, hypo/hyperkalemia, metabolic acidosis, metabolic hypochloremic alkalosis) if hyperkalemia > 6 mmol/l: stop spironolactone if hypokalemia < 3.5 mmol/l: stop furosemide Renal impairment Hepatic Encephalopathy Gynecomastia Testis hypotrophia Muscle cramps (also related to effective hypovolemia): may benefit from albumin, Zn sulfate
 if hyperkalemia > 6 mmol/l: stop spironolactone. if hypokalemia < 3.5 mmol/l: stop furosemide. Renal impairment. Hepatic Encephalopathy. Gynecomastia. Testis hypotrophia. Muscle cramps (also related to effective hypovolemia): may benefit from albumin, Zn sulfate.")
92
Treatment of ascites: Contraindications of diuretic therapy
Severe hyponatremia (< 120 mmol/l) Renal impairment (serum creatinine > 150 umol/l) Active bacterial infection
 Renal impairment (serum creatinine > 150 umol/l) Active bacterial infection.")
93
Treatment of ascites: Grade 3 Ascites
Paracentesis, followed by Sodium restriction Diuretic therapy to reduce the risk of recurrence within 4 wks (90% vs 20%)
")
94
Treatment of ascites: use of Paracentesis in Grade 3 Ascites
Effective and safe in single session All ascitic fluid may be removed, even though in large amount Plasma volume expansion once paracentesis has been completed Plasma substitute if paracentesis < 5 l Albumin if paracentesis > 5 l (6-8 g/l of ascites removed)
")
95
Treatment of ascites: Contraindications and complications of paracentesis
Severe coagulopathy or marked thrombocytopenia (< /ml) Previous surgery or peritoneal adhesions (risk of bowel perforations) Bleeding (may be fatal) Leakage of ascitic fluid Renal impairment
 Previous surgery or peritoneal adhesions (risk of bowel perforations) Bleeding (may be fatal) Leakage of ascitic fluid. Renal impairment.")
96
Treatment of ascites: Refractory Ascites
Repeated total paracentesis, followed by Sodium restriction Diuretic therapy (if tolerated; stop when urine sodium output < 30 mmol/d) TIPS (if paracentesis are not tolerated any more)
 TIPS (if paracentesis are not tolerated any more)")
97
Treatment of dilutional hyponatremia
No published controlled trials Water restriction is ineffective Plasma volume expansion with colloids may have some benefit Vasopressin-2 receptor antagonists seem to be promising

98
Therapy of Hepatorenal Syndrome: present and future
Liver Transplantation Vasopressin Analogues α-Adrenergic Agonists Molecular Adsorbent Recirculating System

99
Therapy of Hepatorenal Syndrome: Vasopressin Analogues (Ornipressin, Terlipressin)
Rationale: increase of splanchnic and systemic vascular resistance, resulting in a redistribution of the circulating blood volume, via suppression of the RAA and sympathetic activities Useful in combination with albumin and low-dose dopamin

100
Therapy of Hepatorenal Syndrome: α-Adrenergic Agonists (midodrine)
Rationale: improvement of systemic vasoconstriction and urinary sodium excretion Effective in combination with plasma volume expansion and octreotide (an inhibitor of the release of endogenous vasodilators)
")
101
HE:FATTORI PRECIPITANTI
ABUSO DI FARMACI (diuretici, sedativi, oppiati) INFEZIONI INTERCORRENTI ECCESSO DI ALCOL / PROTEINE EMORRAGIA DIGESTIVA INTERVENTI CHIRURGICI COPROSTASI IPERAZOTEMIA ALCALOSI IPOKALIEMICA HCC
 INFEZIONI INTERCORRENTI. ECCESSO DI ALCOL / PROTEINE. EMORRAGIA DIGESTIVA. INTERVENTI CHIRURGICI. COPROSTASI. IPERAZOTEMIA. ALCALOSI IPOKALIEMICA. HCC.")
102
HE: TERAPIA MEDICA IDENTIFICARE FATTORE PRECIPITANTE
LIMITARE INTROITO PROTEICO LATTULOSIO (attenzione meteorismo!) ANTIBIOTICI TOPICI (Paromomicina, Rifaximina) CLISTERINI MEDICATI sistematicamente!!!
 ANTIBIOTICI TOPICI (Paromomicina, Rifaximina) CLISTERINI MEDICATI sistematicamente!!!")
Similar presentations













>")
: 337–342. Canadian Journal of Surgery The.>")







 that progresses to cirrhosis Replacement of liver tissue.>")
 Cause ( Etiology) Complication Complication.>")



