Download presentation
Presentation is loading. Please wait.

1
Presented by: Dr. AbdulRahman Al-Garni
NONUNION OF FRACTURES Presented by: Dr. AbdulRahman Al-Garni

2
Introduction: 5% of long bone fractures will result in nonunion and even more in delayed union. Nonunion is considered when healing has not advanced at the average rate for the location and type of fracture (usually more than 6 months).
.")
3
Nonunion is difficult to define because of the many different factors that must be considered. In general, the absence of any clinical or radiographic evidence of progression of fracture healing for 2-3 months after the expected time period for healing constitutes a nonunion.

4
Causes: Although the exact causes of non- union are unknown, both systemic and local factors are thought to contribute to the development. Systemic factors include the patients metabolic and nutritional status, general health and activity level. Smoking and the use of alcohol has been implicated.

5
Local factors: Nonunion is more common when the fracture of long bone is open, infected, segmental with impaired blood supply usually to the middle fragment, immobilised for an insufficient time, distracted (either by traction or plating) or fracture of irradiated bone).
 or fracture of irradiated bone).")
6
The incidence of nonunion in the long bones varies with each bone and with the methods of treating acute fractures.

7
Tibia probably is the most frequent site of nonunion with the increasing frequency of severe open tibial fractures, however, with the more frequent use of interlocking femoral nails, nonunion after femoral fractures have become rare.

9
In a non union, the normal. fracture. repair process occurs
In a non union, the normal fracture repair process occurs only minimally, is interrupted, or does not result in the formation of bridging bone. The most common cause of non union in humans despite modern treatment, is excessive motion at the fracture site. It results in cell and matrix disruption that prevents bridging of the fracture site by calcified or ossified tissue.

10
Loss of blood supply to the bone. ends at the fracture site or in
Loss of blood supply to the bone ends at the fracture site or in the surrounding soft-tissue envelope. Certain fractures have a higher incidence of non union due to anatomic factors in the vascular supply to one or more of the major bone fragments.

11
Typical examples are displaced. subcapital fractures of the femoral
Typical examples are displaced subcapital fractures of the femoral neck, which result in avascular necrosis of the femoral head and non union of the femoral neck; fractures at the waist of the carpal scaphoid, which result in avascularity of the proximal pole and nonunion; and fractures of the neck of the talus, which can result in loss of blood supply to the body of the talus, particularly if associated with a subtalar or ankle dislocation.

12
Classification: A. Hypertrophic (Hypervascular):
Nonunion can be classified according to the status of bone ends into: A. Hypertrophic (Hypervascular): Sclerotic and flared out. B. Atrophic (Avascular): Osteoporotic, narrowed and rounded.
: Sclerotic and flared out. B. Atrophic (Avascular): Osteoporotic, narrowed and rounded.")
16
Hypervascular nonunion can be
subdivided into: 1. Elephant’s foot: Hypertrophic and rich in callus. 2. Horse hoof: Mildly hypertrophic and poor in callus. 3. Oligotrophic: Not hypertrophic but are vascular.

18
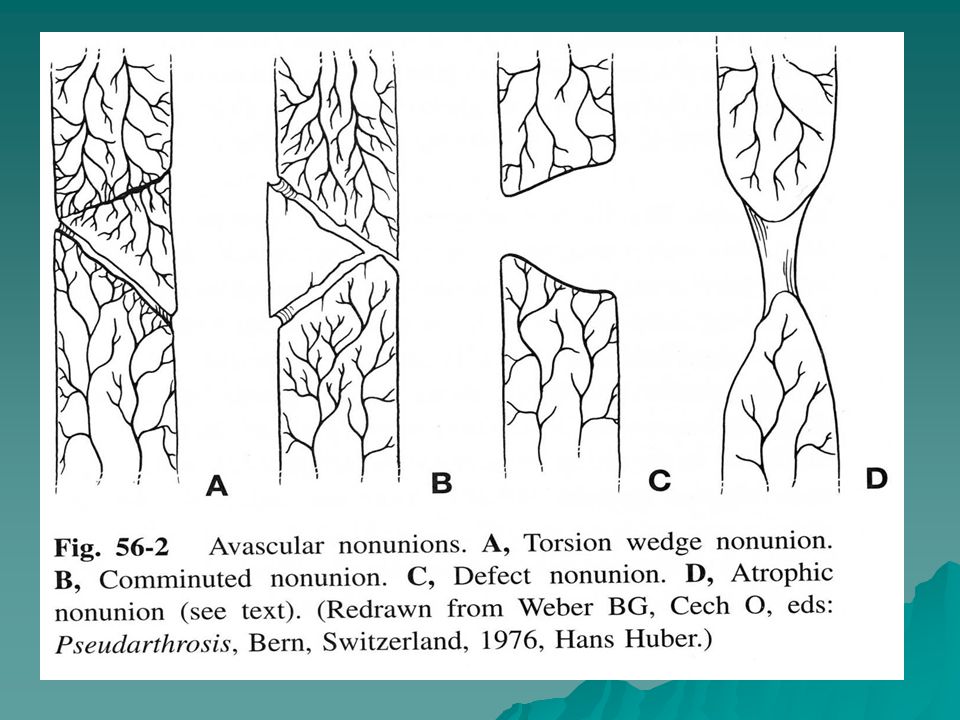
Avascular Non-union: Torsion wedge : An intermediate fragment has healed to one main fragment. Comminuted: One or more necrotic intermediate fragments. Defect: Loss of fragment of a diaphysis of a long bone. Atrophic: Final result

20
Infected non unions must be. recognized. A history of prior
Infected non unions must be recognized. A history of prior infection is important, but if the nonunion site shows no local signs of infection and there has been no active drainage for 6 mos. or more (particularly if the previous infection was caused by an antibiotic-sensitive organism that was successfully eradicated), then operative intervention can usually proceed.
, then operative intervention can usually proceed.")
21
Nonunion with active signs of infection ,however usually require eradication of the infection first,with thorough irrigation and debridement,removal of all devitalised bone ,good stability(usually with external fixator),and achievement of good quality,soft tissue coverage.
,and achievement of good quality,soft tissue coverage.")
22
It is possible to achieve union in the presence of active infection,but usually it must be eradicated before proceeding with treatment .

23
PRINCIPLES OF TREATMENT
The primary objective is to achieve solid union of the fracture site,good level of function,little or no shortening or malalignment and good range of motion,musle strength and neurovascular function.

25
DIAGNOSIS History : original injury and the initial treatment,infection at any time,systemic illness and habits.

26
DIAGNOSIS The most typical complaint is pain at fracture site often severe and aggravated by motion and weight bearing.

27
DIAGNOSIS In the physical examination,the
pathognomonic sign is motion in the fracture site,occasionally with crepitus.Limb alignment,joint and NV status.

28
IMAGING Plain radiograph:AP,lateral and or oblique.The key to dignosis on plain films is placing the nonunion in line with the cetral beam of the radiograph.

31
IMAGING CT with reconstruction particularly for metaphyseal and juxaarticular fractures.

32
IMAGING Use technetium bone scans to rule out synovial pseudarthrosis in hypertrophic non unions of which you are contemplating treatment with either electrical stimulation or closed intramedullary nailing.

33
NONOPERATIVE TREATMENT
Cast and brace immobilisation:little role.

34
ELECTRICAL STIMULATION
In tissue and bone cells, the intial response to electricity is increased bone cell proliferation and no change in or decreased matrix production and alkaline phosphatase activity. Later, matrix production increases and matrix calcification is stimulated or increased.

35
ELECTRICAL STIMULATION
The most common indication is delayed union in good position particularly of the diaphysis of the tibia or femur.Other indications include fractures in acceptable alignment,which can be immobilised in functional casts or brace in patients who significants contraindications to surgery such as systemic illness,poor quality soft tissue and infection.

36
ELETRICAL STIMULATION
Contraindications to non invasive electrical stimulation for treating nonunion include a large gap at the fracture site and synovial pseudarthrosis. Success rate is 74% to 79%.

37
Ultrasound and Bone Marrow Injection: may have a role however not proven.

38
SURGICAL TREATMENT Proper preoperative planning.

39
PLATE FIXATION Plate fixation without bone graft is applicable to hypertrophic and well vascularized nonunions where increasing the stability of the fracture site alone will result in union. Oligotrophic nonunions and all of the avascular nonunions require bone grafting.

40
IM NAILING Locked IM nailing is most useful for nonunions in the diaphysis of tibia or femur.

41
The best indication for. dynamization is a nonunion of. the
The best indication for dynamization is a nonunion of the femur or tibia that already has a large reamed nail in place and where the fracture is oblique so that weight bearing will cause increasing stability, particularly in rotation. Exchange nailing

42
Ilizarov technique Severe shortening,major bone deficiency,deformity and soft tissue contractures.

43
THANK YOU

Similar presentations









, F.R.C.S.(C )>")















>")
