Download presentation
Presentation is loading. Please wait.

2
Patient-Reported Outcomes: Introducion and Overview Pythia Nieuwkerk, PhD Department of Medical Psychology Academic Medical Center, Amsterdam

3
Outline presentation What are patient–reported outcomes (PROs)? –How do PROs complement traditional clinical outcome measures? How can we measure PROs? –Type of measures How are PROs used in clinical research? –Examples

4
What is a Patient-Reported Outcome? A PRO is any report of the status of a patient’s health condition that comes directly from the patient –without interpretation of the patient’s response by a clinician or anyone else. 1 The term PRO addresses the source of the report, and not the concept or content of the report. 2 1. FDA, 2009, 2. Patrick et al. 2007

5
What concepts do PRO instruments measure? Concepts measured by PROs differ in their degree of complexity: –From simple eg, presence of a symptom –To more complex concepts eg, ability to carry out activities of daily living –To even more complex concepts eg, health-related quality of life

6
What is health-related quality of life? Health: A state of complete physical, social, and mental well-being, not merely the absence of disease or infirmity WHO, 1948

7
WHO-based consensus of “Quality of Life”MentalFunctioning PhysicalFunctioning Social Functioning Multi-dimensional Subjective Affected by disease/treatment

8
Subjectivity and Objectivity HRQoL is not subjective in the usual sense of the term It can be measured accurately in an individual, and in a group It is “subjective” in that it: –derives from the individual patient. –represents what is important to the individual patient.

9
How do PROs complement traditional clinical outcome measures?

10
WILSON-CLEARY MODEL OF HEALTH OUTCOMES Characteristics of Individual Biological and Physiological Variables Symptoms Functional Status General Health Perceptions Quality of Life Characteristics of Environment Wilson & Cleary JAMA (1995)
")
11
Motivations for PRO/QOL research Changing the concept of treatment model –Switching from biomedical model to patient-centered model –Living longer and comfortable, especially for cancer patients, elderly population, etc.

12
Number of papers on “quality of life” published each year (PubMed)
")
13
Motivations for PRO/QOL research Some treatment effects are known only to the patient –eg, pain intensity and fatigue Capturing different aspects of health outcomes extended beyond biomedical / clinical indicators –eg, symptoms and functioning, comprehensive assessment of impact of disease and treatment

14
When are PROs most relevant When no survival gain is expected (e.g. palliative treatments) When no significant differences in survival are expected Where survival is gained at the expense of major toxicity and treatment burden
 When no significant differences in survival are expected Where survival is gained at the expense of major toxicity and treatment burden.")
15
How can we measure PROs?

16
www.proqolid.org
17
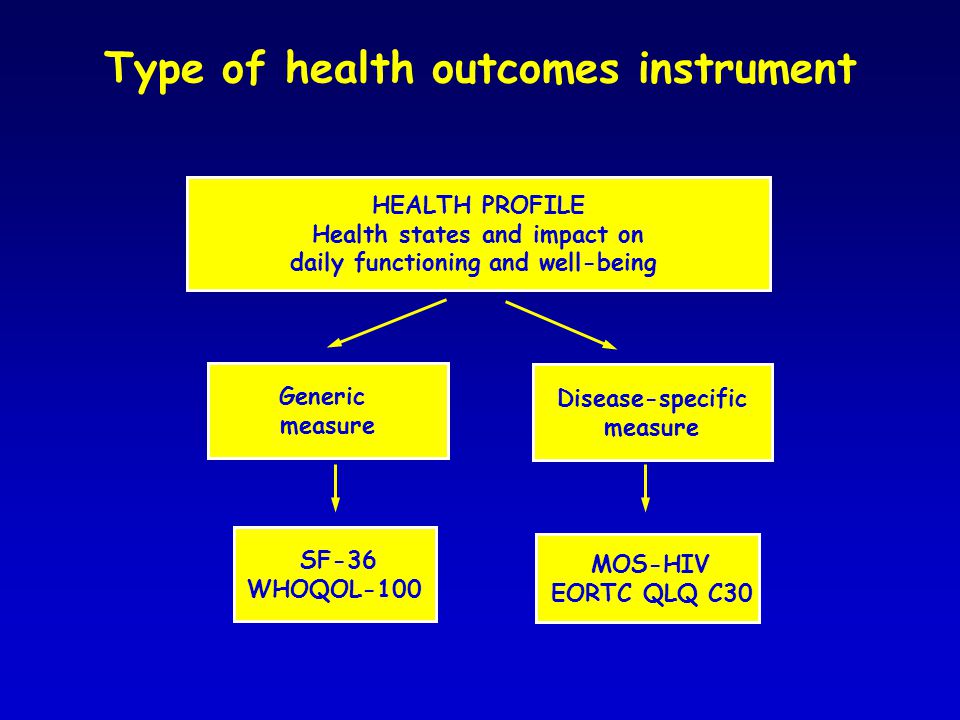
Type of health outcomes instrument HEALTH PROFILE Health states and impact on daily functioning and well-being Generic measure Disease-specific measure SF-36 WHOQOL-100 MOS-HIV EORTC QLQ C30

18
Generic instrument- SF-36 Health profile: 8 domains Physical functioning (10 items) Role limitations/physical (4 items) Role limitations/emotional (3 items) Social functioning (2 items) Emotional well-being (5 items) Energy/fatigue (4 items) Pain (2 items) General health perceptions (5 items)
 Role limitations/physical (4 items) Role limitations/emotional (3 items) Social functioning (2 items) Emotional well-being (5 items) Energy/fatigue (4 items) Pain (2 items) General health perceptions (5 items)")
19
Does your health now limit you in walking more than a mile? (If so, how much?) No, not limited at all Yes, limited a little Yes, limited a lot
 No, not limited at all Yes, limited a little Yes, limited a lot.")
20
How much of the time during the past 4 weeks have you been happy? None of the time A little of the time Some of the time Most of the time All of the time

21
Physical Health Physical function Role function- physical Pain General Health SF-36 Physical Health

22
SF-36 Mental Health Mental Health Emotional Well-Being Role function- emotional Energy Social function

23
Generic instrument – WHOQOL-100 Health profile: 6 domains Physical health (12 items) Psychological health (20 items) Level of independence (16 items) Social relationship (12 items) Environment (32 items) Spirituality, religiousness & personal beliefs (4 items)
 Psychological health (20 items) Level of independence (16 items) Social relationship (12 items) Environment (32 items) Spirituality, religiousness & personal beliefs (4 items)")
24
Same domain, different content Social domain: Social functioning versus social well being Social functioning: limitations due to disease/treatment (SF36, EORTC-QLQ-C30) –More likely to respond to medical treatment Social wellbeing: closeness with family and friends (FACT-G) –More likely to respond to psychosocial interventions
 –More likely to respond to medical treatment Social wellbeing: closeness with family and friends (FACT-G) –More likely to respond to psychosocial interventions")
25
Generic versus Disease specific PROs Generic PRO Intended for use across broad chronic disease populations Allow comparisons across these groups Disadvantage: may not permit adequate disease-specific focus –Disease caused symptoms –Treated related symptoms

26
RELATIVE DISEASE BURDEN: Generic PROs allow for cross-disease comparison of disease impact 30 3436 4050 55 Average Adult Average Well Adult SF-36’s Physical Component Summary (PCS) Type-2 Diabetes Depression Congestive Heart Failure Chronic Lung Disease Asthma Ware & Kosinski, 2001
 Type-2 Diabetes Depression Congestive Heart Failure Chronic Lung Disease Asthma Ware & Kosinski, 2001")
27
Generic versus Disease specific PROs Disease specific PRO Focus on the impact of a particular condition on the patient’s functioning and experience Responsive to disease-related changes Cannot be used across populations with other diseases

28
WILSON-CLEARY MODEL OF HEALTH OUTCOMES Characteristics of Individual Biological and Physiological Variables Symptoms Functional Status General Health Perceptions Quality of Life Characteristics of Environment Wilson & Cleary JAMA (1995)
")
29
Combining PRO measures Disease-specific and Generic PROs are complementary: When both are included in a study, it is possible to capture: –Disease-specific concepts –Generic concepts, compare to norm: (relative) burden of illness / benefit of treatment
 burden of illness / benefit of treatment")
30
Measuring PROs/HRQL No standard scale, need to specify what we want to measure –What is your research question? –Who are your patients? –What do you anticipate what will happen? Appropriateness of the measure to the question or issue of concern. Correspondence between the content of the measure and goals of the study.

31
How are PROs used in clinical research?

32
Characterizing the burden of disease and treatment Characterizing treatment-specific outcomes for use in shared decision making Predicting patient outcomes Evaluating the effectiveness of interventions Study Goals

34
Functional scales Physical functioning Role functioning Cognitive functioning Social functioning Emotional functioning The EORTC QLQ-C30

35
Functional scales Physical functioning Role functioning Cognitive functioning Social functioning Emotional functioning Fatigue Pain Nausea and Vomiting Dyspnea Insomnia Appetite loss Constipation Diarrhea Financial difficulties Symptoms The EORTC QLQ-C30

36
Functional scales Physical functioning Role functioning Cognitive functioning Social functioning Emotional functioning Fatigue Pain Nausea and Vomiting Dyspnea Insomnia Appetite loss Constipation Diarrhea Financial difficulties Symptoms Global health status Overall QoL Global health status scale The EORTC QLQ-C30

37
Functional scales Physical functioning Role functioning Cognitive functioning Social functioning Emotional functioning Fatigue Pain Nausea and Vomiting Dyspnea Insomnia Appetite loss Constipation Diarrhea Financial difficulties Symptoms Global health status Overall QoL Global health status scale Range 0 - 100 Standardized score The EORTC QLQ-C30

38
Functional scales Physical functioning Role functioning Cognitive functioning Social functioning Emotional functioning Fatigue Pain Nausea and Vomiting Dyspnea Insomnia Appetite loss Constipation Diarrhea Financial difficulties Symptoms Global health status Overall QoL Global health status scale Range 0 - 100 Standardized score The EORTC QLQ-C30 A higher score indicates a higher level of functioning A higher score indicates a higher level of symptoms A higher score indicates a higher level of QoL

39
0 = Poor QOL 71 63 83 62 71 38 10 31 28 34 20 11 7 64 14 2 6 4 2 4 71 96 93 94 77 91 Physical functioning Role functioning Cognitive functioning Emotional functioning Social functioning Fatigue Pain Nausea and Vomiting Dyspnea Insomnia Appetite loss Constipation Diarrhea Global health status Functional scales Healthy women (50-59 years) (Schwarz et al. Eur J Cancer, 2001) Metastatic breast cancer baseline (Bottomley et al 2003) Metastatic breast cancer at cycle 2 of doxorubicin/cyclophosphamide 100 = Many symptoms O= No symptoms 100 = Good QOL Profiles Symptoms scales
 Metastatic breast cancer baseline (Bottomley et al 2003) Metastatic breast cancer at cycle 2 of doxorubicin/cyclophosphamide 100 = Many symptoms O= No symptoms 100 = Good QOL Profiles Symptoms scales.")
40
Characterizing the burden of disease and treatment Characterizing treatment-specific outcomes for use in shared decision making Predicting patient outcomes Evaluating the effectiveness of interventions Study Goals

41
Changes in HRQL from start to 18 months of antiretroviral therapy for HIV-infection Physical functionRole functionSocial functionCognitive function Pain VitalityHealth distressGeneral healthMental healthOverall QoL

42
Ccharacterizing the burden of disease and treatment Characterizing treatment-specific outcomes for use in shared decision making Predicting patient outcomes Evaluating the effectiveness of interventions Study Goals

43
Predicting survival in HIV infection 560 HIV infected patients starting HAART. Completed the MOS HIV between 1998-2000. All cause mortality established in March 2008. 66 patients (11.8%) died during follow-up. Physical Health Summary score (MOS HIV) significant predictor of survival, independent of other (clinical) parameters. de Boer-van der Kolk: CID 2010
 died during follow-up. Physical Health Summary score (MOS HIV) significant predictor of survival, independent of other (clinical) parameters. de Boer-van der Kolk: CID")
44
Physical Health summary score (MOS-HIV) de Boer-van der Kolk: CID 2010
 de Boer-van der Kolk: CID 2010")
45
Predicting Outcomes Baseline HRQL has been shown to be an independent predictor for overall survival –Overview of 36 trials that assessed baseline PROs and mortality (Gotay, JCO 26:1355, 2009) PRO is a complex biomarker that can be highly predictive –Help signal those patients who are in need of medical attention –Can be an early warning useful for clinical decision making –Can be used as a stratification variable in research
 PRO is a complex biomarker that can be highly predictive –Help signal those patients who are in need of medical attention –Can be an early warning useful for clinical decision making –Can be used as a stratification variable in research")
46
Characterizing the burden of disease and treatment Characterizing treatment-specific outcomes for use in shared decision making Predicting patient outcomes Evaluating the effectiveness of interventions Study Goals

47
VITAL study Prevention of Coronary Heart Disease Intervention to enhance adherence to statin therapy and life-style recommendations

48
Protocolized (nurse practitioner). Identification individual risk factors. Calculation Absolute Cardiovascular Risk (Framingham risk score) Graphical presentation personal risk Risk Passport. Life style counseling (stop smoking, weight reduction) Risk counseling
 Graphical presentation personal risk Risk Passport. Life style counseling (stop smoking, weight reduction) Risk counseling.")
49
Risk Passport

50
Inclusion Criteria > 18 yrs Indication for statin therapy - primary prevention - secondary prevention Subjects (n = 201, from outpatient clinics)
")
51
Study endpoints Primary endpointsPrimary endpoints –LDL cholesterol levels –Adherence to statins –Anxiety Secondary endpointSecondary endpoint –Quality of Life (QOL)
")
52
PROs Adherence to statins:Adherence to statins: Please estimate the percentage of prescribed lipid lowering medication that you have taken during the last month –9 point scale (<30% to 100%) Anxiety (HADS)Anxiety (HADS) Quality of Life (SF-12)Quality of Life (SF-12)
 Anxiety (HADS)Anxiety (HADS) Quality of Life (SF-12)Quality of Life (SF-12)")
53
0 3 9 18 (month) 0 3 9 18 (month) Questionnaire Weight, RR LDL cholesterol risk counseling risk calculation Questionnaire Weight, RR LDL cholesterol risk counseling risk calculation Questionnaire Weight, RR LDL cholesterol risk counseling risk calculation Questionnaire Weight, RR LLDL cholesterol risk counseling risk calculation Extended care Questionnaire Weight, RR LDL cholesterol Questionnaire Weight, RR LDL cholesterol Questionnaire Weight, RR LDL cholesterol Questionnaire Weight, RR LLDL cholesterol Routine care
 (month) Questionnaire Weight, RR LDL cholesterol risk counseling risk calculation Questionnaire Weight, RR LDL cholesterol risk counseling risk calculation Questionnaire Weight, RR LDL cholesterol risk counseling risk calculation Questionnaire Weight, RR LLDL cholesterol risk counseling risk calculation Extended care Questionnaire Weight, RR LDL cholesterol Questionnaire Weight, RR LDL cholesterol Questionnaire Weight, RR LDL cholesterol Questionnaire Weight, RR LLDL cholesterol Routine care")
54
Result: LDL cholesterol Primary prevention Secondary prevention Extended care Routine care

55
Results: Anxiety and adherence Extended care Routine care

56
Results: HRQL Extended care Routine care

57
Summary PROs can be used to assess the impact of disease and treatment from the patient perspective. Various PRO measures are available from which you can choose depending on your study goals. PROs can complement traditional clinical outcome measures when applied in clinical research.

Similar presentations

>")




 Claims Ann Marie Trentacosti, M.D. Study Endpoints and Labeling Office of New Drugs Food.>")







 measure for your clinical study Dr Keith Meadows, DHP Research & Consultancy Ltd.>")




