Download presentation
Presentation is loading. Please wait.

1
Squint Dr. monn salah

2
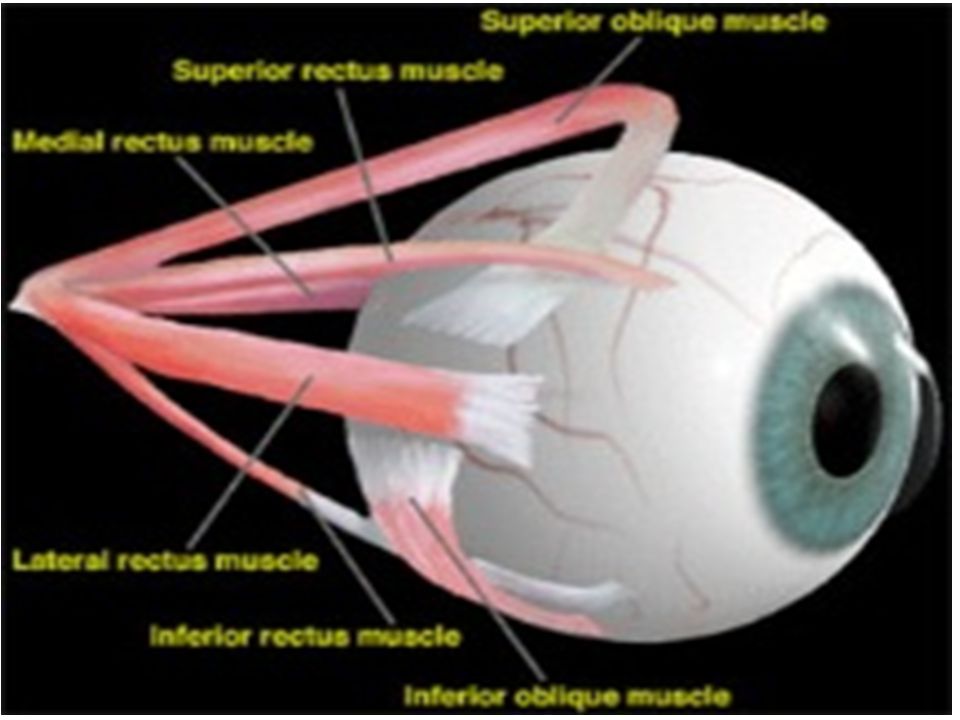
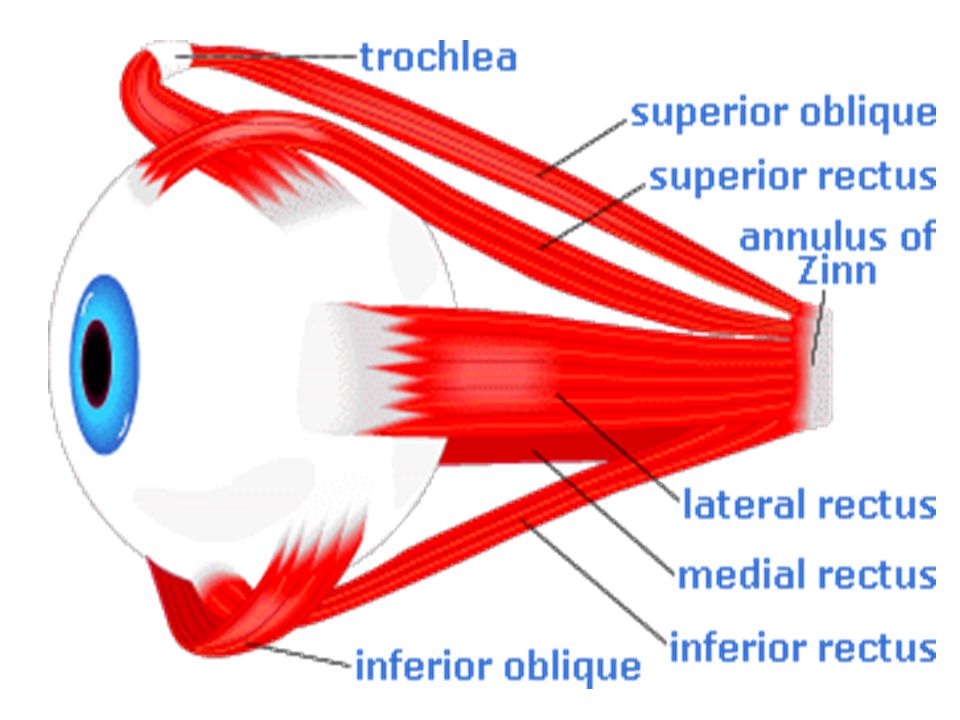
Extraocular Muscles Origin Common tendon at the apex of orbit. (Annulus tendinious communis of zinn)
.")
4
Insertion

7
Action M.R : Adduction L.R : Abduction S.R : Elevation (when eye looks out) I.R : Depression (when eye looks out) S.D : Depression (when eye looks in) I.O : Elevation (when eye looks in)
 I.R : Depression (when eye looks out) S.D : Depression (when eye looks in) I.O : Elevation (when eye looks in)")
8
Nerve Supply 1.Oculomotor (3 rd cn) : All muscles except LR and SO. 2.Abducent : LR 3. Trochlear : SO

9
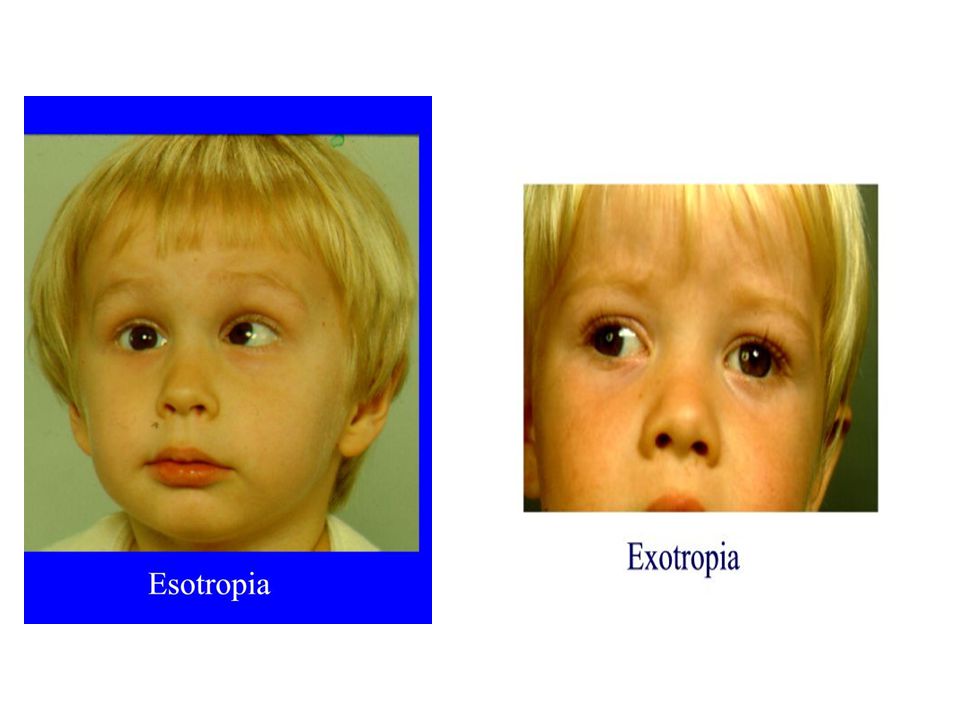
Types of Squint Apparent vs. True Horizontal vs. Vertical Uniocular vs. alternating Concomitant vs. Non Comcominant

11
Apparent Squint

12
Causes: Epicanthus Abnormal angle alpha Large positive angle (hypermetropia) apparent convergent squint Negative angle alpha (High myopia) apparent divergent squint Abnormal IPD Wide IPD apparent divergent squint Small IPD apparent convergent squint
 apparent convergent squint Negative angle alpha (High myopia) apparent divergent squint Abnormal IPD Wide IPD apparent divergent squint Small IPD apparent convergent squint")
13
Diagnosis: Cause is present Central corneal reflex No ocular movement on cover-uncover test

14
Latent Squint (Heterophoria)
")
15
Tendency to ocular deviation due to muscular imbalance, checked by brain to maintain binocular vision.

16
Types: Horizontal (Eso or exophoria) Vertical (Hyper or Hypophoria) Torsional (incyclo or excyclophoria)
 Vertical (Hyper or Hypophoria) Torsional (incyclo or excyclophoria)")
17
Symptoms: Rule: If fully compensated, no symptoms. Eye strain (muscular asthenopia) ( Ocular ache, Burning sensation, Headache, Lacrimation, Photophobia, Blurring of vision) Running of letters due to transient diplopia Difficulty to follow a rapidly moving object Difficulty to change focus from near to far objects Intermittent diplopia
 ( Ocular ache, Burning sensation, Headache, Lacrimation, Photophobia, Blurring of vision) Running of letters due to transient diplopia Difficulty to follow a rapidly moving object Difficulty to change focus from near to far objects Intermittent diplopia.")
18
Diagnosis: Cover test Maddox rod test Maddox wing test

19
Cover Test

20
Maddox rod It measures heterophorias. It dissociates 2 eyes for dist. Fixation It consists of fused cylindrical red rods line perpendicular to axis of rod. Patient is asked to locate position of red line to white spot of light. To estimate the degree of squint, place prisms until red line is in the center of white spot

21
Maddox Rod Test

22
Maddox wing Measures heterophorias. It dissociates 2 eye for near fixation. R sees white vertical arrow and red horizontal arrow. L sees vertical and horizontal row of numbers Patient asked which number, arrow is pointing.

23
Maddox Wing Test

24
Treatment: No symptoms, no treatment Optical treatment (Prisms) - Exercising prism: Aim: Strengthen weak muscle Direction: Base of prism in the direction of dev. - Relieving prism: Aim: To relieve annoying symptoms Direction: Base of prism in opposite direction of latent deviation.

25
Concomitant Squint Angle of squint is the same in all directions of gaze.

26
Clinical picture: Ocular deviation (No doplopia) Amblyopia Eccentric fixation
 Amblyopia Eccentric fixation")
27
Investigation: 1.Measure visual acuity 2.Retinoscopy 3.Alternate cover test 4.Measurement of angle squint - Corneal reflex method - Prism cover test - Perimeter - Synoptophore

28
5. Diagnosis of amblyopia -Vision: No improvement with glasses - Synoptophore - Worth four dot test

29
6. Diagnosis of eccentric fixation 7. Grade of binocular vision (synoptophore) - Simultaneous perception - Fusion - Stereopsis
 - Simultaneous perception - Fusion - Stereopsis.")
30
Treatment: Depends upon: - Age of patient and duration of squint - Accommodative or non accommodative - Presence or absence of amblyopia - Type of fixation (central or eccentric) - Grade of binocular vision
 - Grade of binocular vision")
31
Aim of treatment: To restore binocular vision To improve visual acuity To restore normal appearance

32
Lines of treatment: Drugs: Atropine or miotics Spectacles Occlusion therapy Orthoptic exercises Surgical treatment

33
Binocular Vision Grading: 1. Simultaneous perception. 2. Fusion 3. Stereopsis Advantages: 1.Binocular field is larger than uniocular 2.Stereopsis 3.Better visual activity 4.Any defect in vision or field of one eye is masked by the other

34
V-Pattern Deviation It is a pattern in which horizontal deviation becomes more esotripoic on down-gaze and more exotropic on up-gaze. Cause: I.O over action S.O Polsy Tt: Weakening of I.O (recession or disinsertion)
.")
36
A-Pattern Deviation It is a pattern in which horizontal deviation becomes more esotropic on up-gaze and more exotropic on down-gaze. Causes: S.O over action I.O under action

37
Paralytic Squint It is a true manifest deviation of the eye due to paralysis of one or more of EOM, in which the deviation differs in different directions of the gaze.

38
Clinical Picture 1. Limitation of motility in the direction of action of paralysed muscles.

39
2. Deviation of the eye in opposite direction to action of paralysed muscles.

40
Angle of squint is not constant (max. on looking in dir. of action of affected mus. and min. in opp. direction) Secondary angle of deviation is much greater than primary angle of deviation. Primary angle of deviation: angle of squint when normal eye is fixing. Secondary angle: angle of squint when the paralyzed eye is fixing. Excessive impulses reach the paralysed muscles to contract and according to hering law, equal impulses reach the contralat. Synergist) more deviation
 Secondary angle of deviation is much greater than primary angle of deviation. Primary angle of deviation: angle of squint when normal eye is fixing. Secondary angle: angle of squint when the paralyzed eye is fixing. Excessive impulses reach the paralysed muscles to contract and according to hering law, equal impulses reach the contralat. Synergist) more deviation.")
41
3. Binocular diplopia

42
Occurs in direction of action of paralysed ms. and disappears when one eye is covered. Images fall on non-corresponding points of the retina resulting in 2 images. True image: Falls in fovea of normal eye False image: Falls outside fovea of paralysed eye. Diplopia maybe: Uncrossed: LR palsy Crossed : MR palsy

43
4. False projection Due to excessive innervation to move the paralysed eye. Cover normal eye and instruct patient to point to an object, his finger will be directed from the object in the direction of action of the paralysed eye.

44
5. Compensatory head posture ( to avoid diplopia) - Face turn - Chin elevation or depression - Head tilt
 - Face turn - Chin elevation or depression - Head tilt.")
45
6. Headache, vertigo, dizziness, uncertain gait, nausea and vomiting.

46
Investigations

47
Diplopia chart: Ina dark room, place red glass in front right eye and green glass in front left eye. Move a slit of light in all nine directions, ask the patient: - Areas of diplopia - Where is the red and green image - Distance between 2 images - Are the images side by side or higher or tilted

48
Hess screen: Principle: is to dissociate the 2 eyes for distant fixation with the red and green filters. (Hering’s law of equal and simultaneous Innervation of yoke muscles)
.")
50
Treatment

51
Tt. of the cause Surgical Tt. H. (a)If no recovery within 6 mon. surgery (b)Strengthening the ms. if is weak (paresis) (c)If completely paralysed, we operate on other muscles. - Weaken the direct antagonist - Weaken the contralat. Synergist - Strengthen the contralat. Antagonist - Ms. transposition
Strengthening the ms. if is weak (paresis) (c)If completely paralysed, we operate on other muscles. - Weaken the direct antagonist - Weaken the contralat. Synergist - Strengthen the contralat. Antagonist - Ms. transposition.")
52
Sixth nerve palsy e.g. Rt. LR palsy Rt. Convergent squint Limitation of abduction of rt. Eye Angle of squint is large when the patient looks to the right Angle of squint is larger when the rt. Eye attempts fixation Diplopia on looking to rt. side (uncrossed) False projection occurs to rt. side Face turn to the right
 False projection occurs to rt. side Face turn to the right.")
53
Third nerve palsy Ptosis Deviation of the eye out. Limitation of mov. in direction of involved muscles No diplopia (due to ptosis) Dilatation of pupil or loss of accom.
 Dilatation of pupil or loss of accom..")
Similar presentations