Download presentation
Presentation is loading. Please wait.

1
Case Study 78 by Erica Ducker
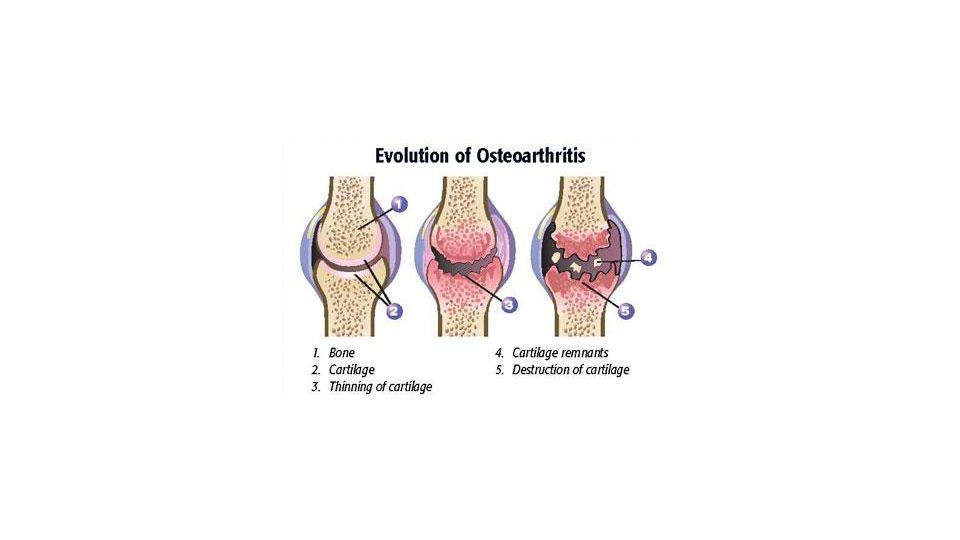
Osteoarthritis Case Study 78 by Erica Ducker

5
Chief Complaints -Trouble moving and going places
-Joint pain, most severe in knees and in lower back.

6
History of Present Illness
-71 year old, overweight woman. -Complaining of long history or bilateral knee discomfort. -Discomfort in left knee greater than in the right knee. -Had lower back pain for many years, but recently has become worse. -Has difficulty using the stairs at home. -Rheumatologist tried a variety of nonsteroidal anti-inflammatory drugs to help with pain control, but they only gave her mild relief and caused significant intolerable stomach discomfort. -Pain alleviated with oxycodone. -Knees got significantly more painful after she gained 20 lbs in a span of 9 months. Complaining of long history or bilateral knee discomfort that becomes worse when it rains and feels better in warm dry weather. However, warm dry weather no longer improves her arthritis. Discomfort in left knee greater than in the right knee. Had lower back pain for many years, but recently has become worse. Has difficulty using the stairs at home. Rheumatologist tried a variety of NSAIDs to help with pain control, but they only gave her mild relief and caused significant intolerable stomach discomfort. Pain alleviated with oxycodone. Began to build tolerance toward it, requested higher doses, physician could not prescribe a higher dose, suggested surgery. Knees got significantly more painful after she gained 20 lbs in a span of 9 months. Joints feel stiff after long periods without movement. Tend to “loosen up” with activity. Worried about osteoporosis due to family history. However, no clinical manifestations have developed. Pain alleviated with oxycodone (Treats moderate to severe pain when around-the-clock pain relief is needed for a long period of time. Slow-release oxycodone is a narcotic medicine that should not be taken more often than every 12 hours.) Began to build tolerance toward it, requested higher doses, physician could not prescribe a higher dose, suggested surgery. Joints feel stiff after long periods without movement. Tend to “loosen up” with activity. Worried about osteoporosis due to family history. However, no clinical manifestations have developed.
 Began to build tolerance toward it, requested higher doses, physician could not prescribe a higher dose, suggested surgery. Joints feel stiff after long periods without movement. Tend to loosen up with activity. Worried about osteoporosis due to family history. However, no clinical manifestations have developed.")
7
Past Medical History -At age 23, left knee injury in a motor vehicle accident, no surgery required. -Broken hip at age 60 by falling on icy sidewalk. Hip healed well, no significant symptoms suggest no hip involvement in present complaints. -14 year history of osteoarthritis, 10 year history of hypertension, 4 year history of hypercholesterolemia, 4 year history of diabetes mellitus type 2, -hospitalized for diverticulitis incident 2 years ago. -Only surgery was hysterectomy without oophorectomy 21 years ago. Menopause at age 49, never has taken hormones. diverticulitis: Diverticulitis is small, bulging sacs or pouches of the inner lining of the intestine (diverticulosis) that become inflamed or infected. Most often, these pouches are in the large intestine (colon)
 that become inflamed or infected. Most often, these pouches are in the large intestine (colon)")
8
Family History -Father died of acute myocardial infarction at age 53
-Mother died of breast cancer at age 80 -Brother age 68, hypertension -Sister age 74, severe allergies, two mitral valve replacements for rheumatic heart disease -Sister age 72, osteoarthritis -Positive history of osteoporosis in mother and maternal grandmother

9
Social History -Lives with her 72 year old sister in 3-story townhouse near the beach. -Exercises regularly in the pool, sometimes ocean. Can no longer walk long distances daily as she did in the past. -Well balanced diet with plenty of fresh fruit, vegetables, whole grains, dairy, admits to eating too many sweets. -Has Medicare but no other health insurance. -Does not smoke -Drinks 1-2 cocktails or glasses of white wine with dinner. -Hobbies: quilting, baking, teaching piano to children.

10
Review of Systems -Mild pain in right shoulder with lifting and carrying. -Lower back pain with occasional shooting pains radiating to back of thigh. -Deep aching pain in the pretibial area bilaterally and extending distally to the ankles and toes. -Denies swollen, red, hot joints, but notes “hard lumps” at the margins of the interphalangeal joints. -Denies numbness and weakness in legs, denies discomfort in wrists and elbows. -Negative for headaches, neck stiffness, shortness of breath, chest pains, urinary frequency or dysuria, constipation, diarrhea, nausea, loss of appetite, or significant changes in the appearance of urine or stools. -Finger-stick blood glucose levels are usually around 180 mg/dL -Occasional polyuria but no changes in vision Why are changes in vision important to note with polyuria? Diabetes mellitus: high volume of pee, body trying to rid itself of extra sugar, blurred vision is caused by hyperosmolar state of blood due to hyperglycemia. These two conditions together relate to patient’s diabetes mellitus type 2 and blood sugar level maintenance.

11
Medications Zolpidem 10 mg po Q HS PRN Atorvastatin 20 mg po Q HS
Atenolol 25 mg po QD Lisinopril 40 mg po QD Metformin 250 mg po QD Glipizide 2.5 mg po QD Acetaminophen 1000 mg po TID High-potency multivitamin supplement with calcium, iron, and zinc po QD Calcium 600 mg with Vitamin D 125 IU supplement po BID with meals No known allergies Zolpidem? Why both meformin and glipizide for DM type 2? Why both atenolol and lisinopril for hypertension?

12
Physical Exam General Vital Signs
Alert, well developed and well nourished, overweight caucasian female who appears slightly anxious but otherwise in no acute or apparent distress. Vital Signs Blood pressure, sitting, left arm 155/88 Pulse 72 and regular Respiratory rate 15 and unlabored Temperature 98.8 Degrees F Height 5’3” Weight 164 lbs

13
Physical Exam Skin Head, Eyes, Ears, Nose, Throat
Warm, dry, normal turgor, no petechiae, ecchymoses, or rash Head, Eyes, Ears, Nose, Throat Normocephalic/Atraumatic Pupils equal, round, and reactive to light and accommodation Funduscopic exam reveals sharp discs with no vascular abnormalities or papilledema Negative scleral icterus Tympanic membranes intact Mucous membranes moist Negative lateral deviation of tongue, pharyngeal edema, or erythema

14
Physical Exam Neck/Lymph nodes Chest/Lungs Heart Abdomen Breasts
Neck supple, negative for thyromegaly, adenopathy, masses, jugular venous distension, or carotid bruits Chest/Lungs Good chest excursion, Lungs clear to auscultation and pulse Heart Normal S1 and S2, point of maximal impulse normal at 5th intercostal space, regular rate and rhythmn, No murmur/rub/gallop Abdomen Soft and non-tender without guarding, positive for bowel sounds, negative organomegaly, bruits, and masses Breasts Symmetric, no apparent masses, discharge, discoloration, or dimpling

15
Physical Exam Genitalia/Rectum Musculoskeletal/Extremities
Normal female genitalia, positive for mild vaginal atrophy, normal anal sphincter tone, stool heme-negative. Musculoskeletal/Extremities Back with decreased flexion and extension Back pain radiating to right buttock with straight right leg raising >60 degrees Full range of motion at left shoulder, elbows, and ankles Mild left hip discomfort with flexion >90 degrees and with internal and external rotation >45 degrees Hips not tender to palpation Bilateral knee crepitus and enlargement but more pronounced in left knee Slight decrease in range of motion and both Bouchard and Heberden nodes observed bilaterally during hand examination; no tenderness in finger joints Feet without breakdown, ulcers, erythema, or edema Feet without breakdown, ulcers, erythema, or edema relevant b/c patient has diabetes mellitus. Too much sugar in blood can cause diabetic neuropathy, damaged nerves in extremities renders person unable to feel pain or injury. Also may cause muscles of feet to malfunction, causing improper foot alignment and causes foot ulcers to form due to differences in pressure in parts of foot. Also can cause edema in feet. Prevents proper blood flow, prevents proper healing of a wound: can cause necrosis of tissue.

18
edema and erythema: skin infection due to diabetes.

19
Laboratory Blood Test Results
Na meq/L K meq/L Cl meq/L HCO3 23 meq/L BUN 7 mg/dL Cr mg/dL Glu, fasting 241 mg/dL Hb g/dL Hct 39.1% MCV 87 fl MCH pg MCHC g/dL WBC 5.2x10^3/mm^3 Plt x 10^3/mm^3 AST IU/L ALT IU/L Bilirubin, total 0.6 mg/dL Alk phos 97 IU/L Protein, total g/dL Alb g/dL Cholesterol mg/dL HbA1c % Ca mg/dL PO mg/dL Mg mg/dL ESR 14 mm/hr TSH uU/mL

20
Urinalysis Appearance: Pale yellow, clear Specific gravity 1.017
pH 6.3 WBC 0/HPF RBC 0/HPF Leukocyte esterase: negative Nitrites: negative Bacteria: negative Protein: negative Ketones: negative

21
X-Rays Lumbosacral spine
Advanced degenerative changes with disk space narrowing and osteophyte formation at L3-4 and L4-5.

24
X-Rays -No evidence of compression fracture left hip
-Mild to moderate degenerative changes with mild osteophytosis of femoral head -Slight narrowing in joint space, right and left knees -Moderate degenerative changes with joint space narrowing, subchondral sclerosis, and bone cysts -No radiographic evidence of osteoporosis or joint effusions, right shoulder -Mild degenerative changes with bone spurs at head of humerus -Slight narrowing in joint space

25
Case Questions What is crepitus?
What are four risk factors of Osteoarthritis? What is the primary cause for limited range of motion in osteoarthritis? What blood test result distinguishes between gouty arthritis and osteoarthritis?

26
Thank you for your attention!

Similar presentations










 Etiology Result of lifestyle, overweight, smoking, lack of exercise, stress S/S No symptoms If left untreated:>")










 vaccinated for influenza six months ago.>")



