Download presentation
Presentation is loading. Please wait.

1
VARIANT CJD AN UPDATE DR. HESTER WARD National CJD Surveillance Centre Edinburgh, UK h.ward@ed.ac.uk

2
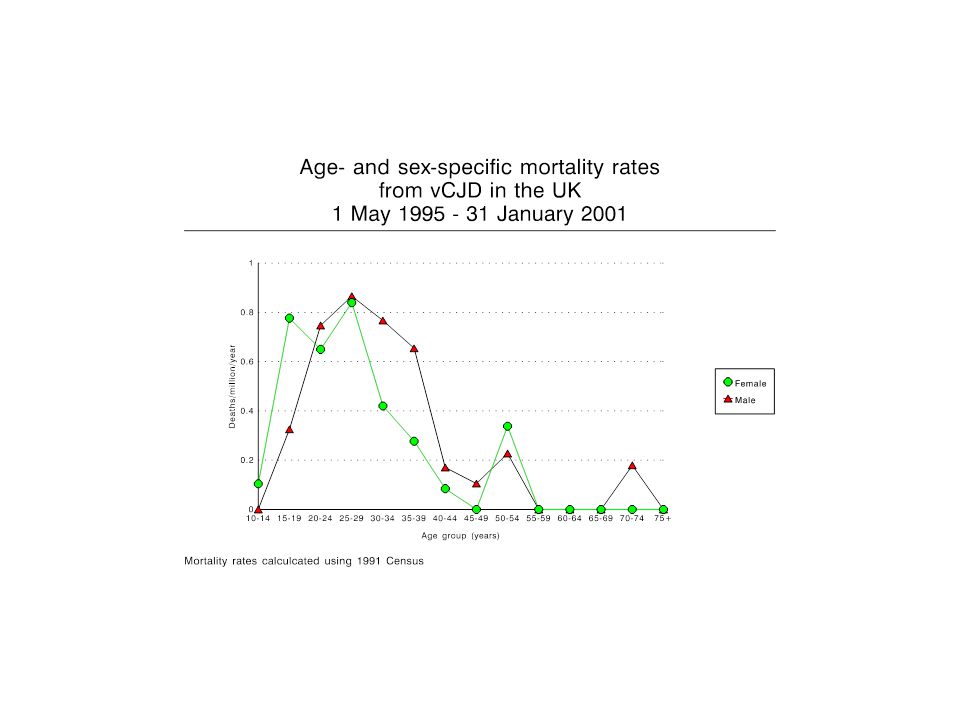
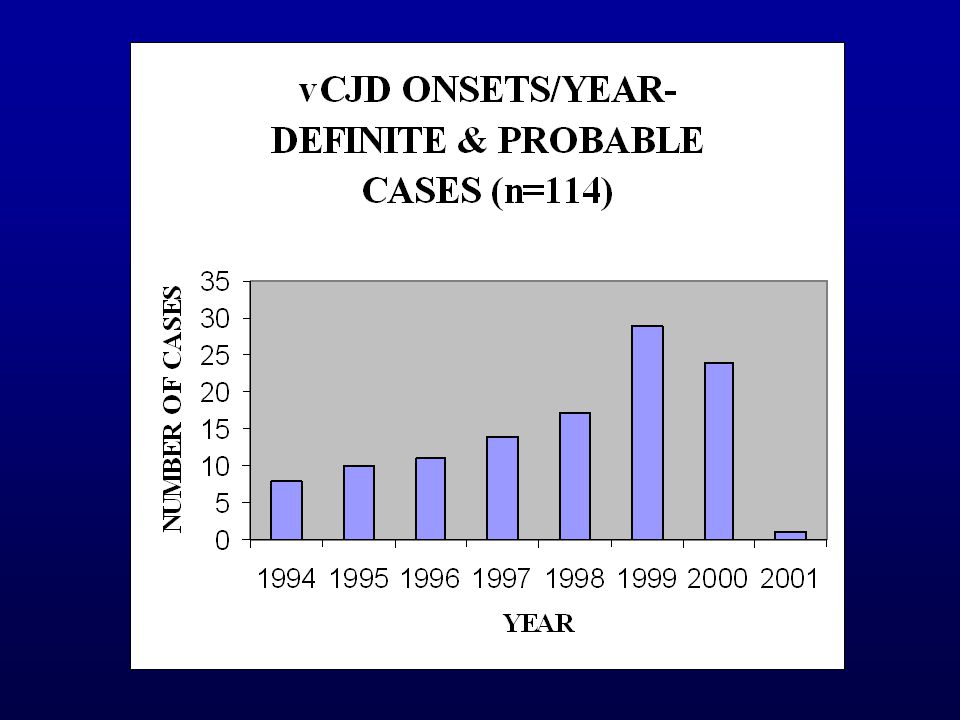
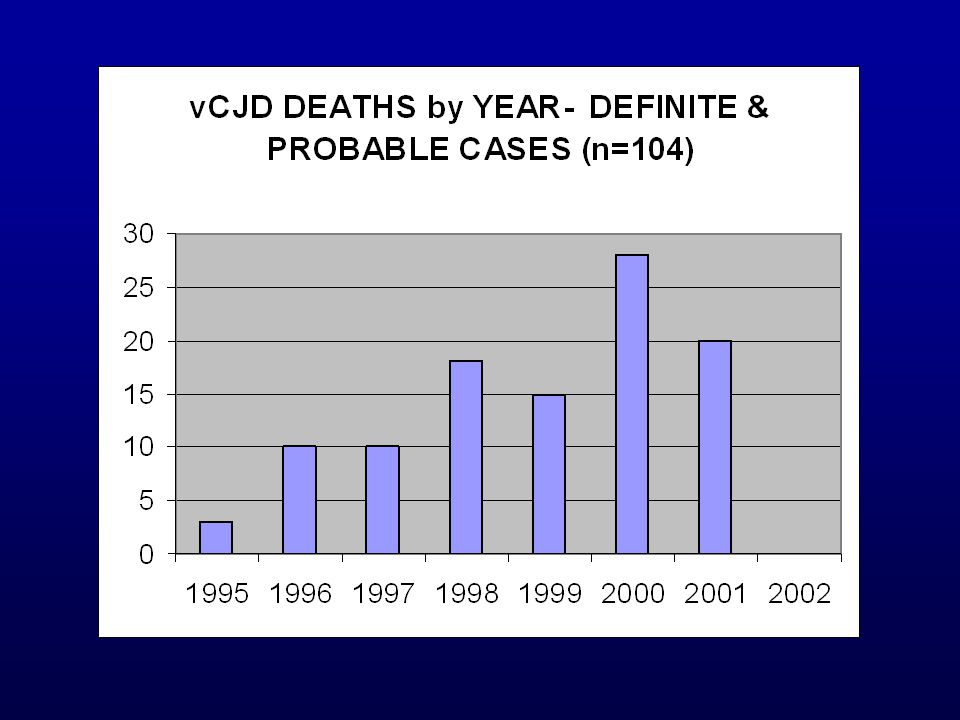
UK frequency of CJD

3
Variant CJD UK 114 definite & probable cases 89 definite cases- confirmed neuropathologically 14 probable cases- died- no post mortem 1 probable case- died- awaiting post mortem 10 probable cases- alive FRANCE: 3 definite & 2 alive probable cases REPUBLIC OF IRELAND: 1 definite case

4
Variant CJD AGE Median age at onset :26 years (range 12 - 74 years) Median age at death :28 years (range 14 - 74 years) GENDER: 60 males : 54 females DURATION OF ILLNES Median: 13 months (range 6 - 39 months) GENETICS: All tested = MM at codon 129 (n= 97)
 Median age at death :28 years (range years) GENDER: 60 males : 54 females DURATION OF ILLNES Median: 13 months (range months) GENETICS: All tested = MM at codon 129 (n= 97)")
8
Courtesy of Nick Andrews, PHLS Statistics Unit, London

9
Geographical distribution of places of residence at onset of symptoms of vCJD cases (n=93)
")
10
Variant CJD - GEOGRAPHY

13
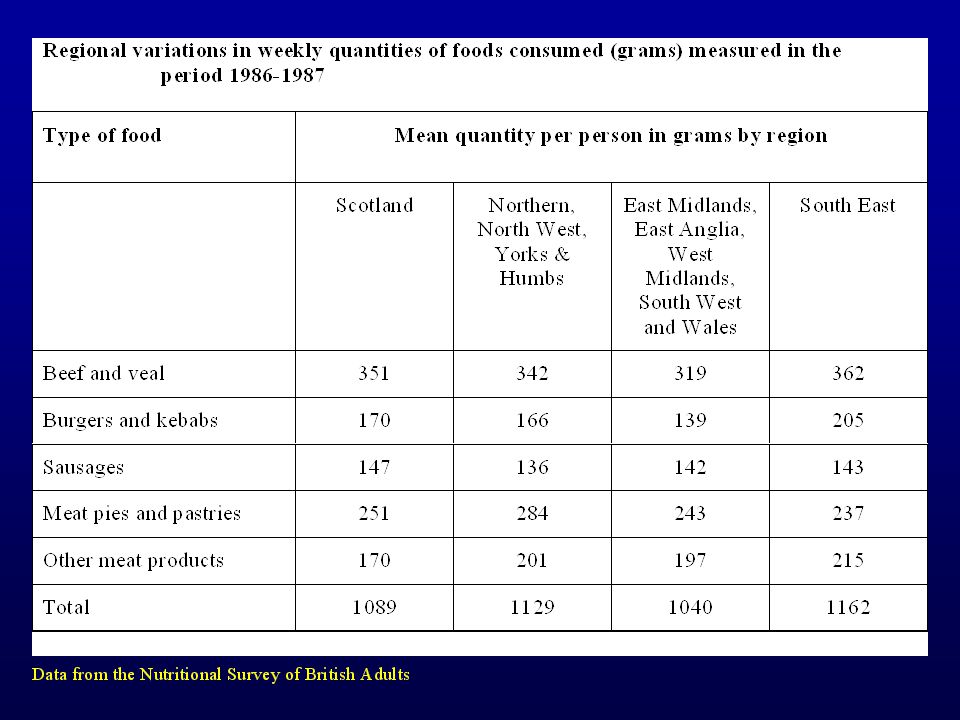
Dietary & Nutritional Survey of British Adults 1986 - 1987 2197 adults aged 16 to 64 years weighed, 7 day dietary records Household Food consumption & Expenditure Report 1984 - 1986 20, 000 households One week records of all foods entering home for consumption

16
Scatterplot of cumulative, age-standardised vCJD incidence against weekly consumption of other meat and meat products (grams) by region (Household Food Consumption and Expenditure: 1988) of cumulative, age-standardised vCJD incidence against weekly consumption of other meat and meat products (grams) by region (dietary data from Household Food Consumption and Expenditure:1988)
 by region (Household Food Consumption and Expenditure: 1988) of cumulative, age-standardised vCJD incidence against weekly consumption of other meat and meat products (grams) by region (dietary data from Household Food Consumption and Expenditure:1988)")
17
GEOGRAPHICALLY ASSOCIATED CASES (GACs) of vCJD
 of vCJD")
18
Geographically associated cases Definition : 2 or more cases of probable or definite vCJD where preliminary investigations suggest there is an association between the cases because of: a) Geographical proximity of residence at some time, either now or in the past; b) Other link with the same geographic area, eg. attending the same school or work place or attending functions in the same area.

19
The Leicester cluster 5 cases of variant CJD lived in Leicestershire (population 870, 000) Cumulative incidence: UK 1.5/ millionLeicester 5.7/ million 4/5 from Charnwood (142, 000): 28.2 / million Kulldorff’s method- spatial scan statistic- Leicestershire- most likely cluster (p<0.004) No other significant clusters (Cousens et al. Lancet 2001; 357: 1002- 1007)
.")
20
The Leicester cluster 4/5 were reported to have bought meat from butchers who processed whole carcass beasts & split the heads to remove the brains for commercial purposes Hypothesis- cases bought meat from butchers that split heads Tested - control study- matched each case to 6 community controls OR 15 (1.6- 139)
")
21
The Leicester cluster If true: minimal incubation- between 10- 16years Does this explain other cases in UK & in other countries? BUT Bias Interview with butchers Brain- where did it go?- food chain…..

22
Variant CJD- RISK FACTORS TO DATE from case control study: No evidence of increased risk of CJD associated with diet, surgery or occupation (although, some differences in diet between cases & controls) BUT- rare disease, recall bias, surrogate witnesses, small numbers, control recruitment
 BUT- rare disease, recall bias, surrogate witnesses, small numbers, control recruitment")
23
Size of the vCJD epidemic- predictions 1997: Cousens et al. Nature; 385: 197-198 (n=14 vCJD) 75- 80, 000 Back calculation MM genotype 2000: Ghani et al. Nature; 406: 583- 584 (n= 55 vCJD) 63- 136 000 Scenario analysis (> 5 million combinations of parameters) MM genotype < 2 cases vCJD per infectious bovine
 , 000 Back calculation MM genotype 2000: Ghani et al. Nature; 406: (n= 55 vCJD) Scenario analysis (> 5 million combinations of parameters) MM genotype < 2 cases vCJD per infectious bovine.")
24
Size of the epidemic- predictions 2001: Huillard d’Aignaux et al. Science; 294: 1792- 1931 (n= 82) Clinical cases: hundreds - few thousands Infected individuals: hundreds - millions, but long mean incubation period & so die from competing causes Close to peak of epidemic Back calculation- calc. number infected based on assumptions of when infected & incubation pd Exposure cut off- 1996 MM genotype ? not reassuring re. potential secondary spread
 Clinical cases: hundreds - few thousands Infected individuals: hundreds - millions, but long mean incubation period & so die from competing causes Close to peak of epidemic Back calculation- calc. number infected based on assumptions of when infected & incubation pd Exposure cut off MM genotype . not reassuring re. potential secondary spread.")
25
Size of the epidemic- predictions 2001: Valleron et al. Science 294: 1726- 1728 (n=97) Total number of cases: 205 (upper limit 403) Mean incubation pd: 16.7 yrs (12- 23) Peak: 2000/ 2001 Bimodal age distribution Age at diagnosis= age at infection + incubation time. Assuming age of infection parallels BSE epidemic- incubation pd calc using deconvolution technique. Exposure cut off: 1990 Exponential decrease in susceptibility >15 years of age
 Total number of cases: 205 (upper limit 403) Mean incubation pd: 16.7 yrs (12- 23) Peak: 2000/ 2001 Bimodal age distribution Age at diagnosis= age at infection + incubation time. Assuming age of infection parallels BSE epidemic- incubation pd calc using deconvolution technique. Exposure cut off: 1990 Exponential decrease in susceptibility >15 years of age.")
26
Size of the epidemic- predictions 2002: Ferguson et al. Nature 9 January 2002; DOI 10.1038/nature 709 Predictions of future cases of vCJD based on BSE infection of British sheep Bovine BSE only: Upper 95% CIs: 50 000- 100 000 vCJD cases Bovine + ovine BSE: Upper 95% CIs: 150, 000 vCJD cases (BSE endemic in national flock) Past exposure to BSE in UK: majority from cattle On- going exposure to BSE: sheep greater than cattle- reduce risk up to 90%- age at slaughter & SRM controls Many assumptions: epidemiology based on scrapie & experimental BSE in sheep, tissue infectivity during incubation
 Past exposure to BSE in UK: majority from cattle On- going exposure to BSE: sheep greater than cattle- reduce risk up to 90%- age at slaughter & SRM controls Many assumptions: epidemiology based on scrapie & experimental BSE in sheep, tissue infectivity during incubation.")
27
Size of the epidemic- predictions Conclusions Much uncertainty, esp incubation period, risk from sheep Only based on MM genotypes (40% of population) ? not necessarily reassuring if considering secondary spread

28
Transfusion Medicine Epidemiology Review (TMER) Joint project between National Blood Service & NCJDSU AIM: to investigate whether any evidence that CJD, including vCJD, may be transmitted via blood supply
 Joint project between National Blood Service & NCJDSU AIM: to investigate whether any evidence that CJD, including vCJD, may be transmitted via blood supply")
29
TMER- vCJD TMER All definite + probable cases vCJD- reported to transfusion service of relevant country (England, Wales, Scotland & Northern Ireland) If a donor- trace fate of all donations- recipient details passed to NCJDSU Reverse TMER vCJD cases (& matched controls) who have received blood transfusions- details passed to BTS Details of donors passed back to NCJDSU
 If a donor- trace fate of all donations- recipient details passed to NCJDSU Reverse TMER vCJD cases (& matched controls) who have received blood transfusions- details passed to BTS Details of donors passed back to NCJDSU")
30
TMER- vCJD RESULTS (April 2001) (n= 87 vCJD cases) TMER 8 cases vCJD were blood donors- 22 recipients between 1981- 1999 None have developed CJD to date- 9 have died from other causes None have registered as blood donors
 (n= 87 vCJD cases) TMER 8 cases vCJD were blood donors- 22 recipients between None have developed CJD to date- 9 have died from other causes None have registered as blood donors")
31
TMER- vCJD Reverse TMER 4 cases of vCJD received blood components (117- 1 case 103 of these) 111 donors- none have developed CJD to date
 111 donors- none have developed CJD to date")
32
National CJD Surveillance Unit, UK Director & Neuropathology- Professor J. Ironside Neurology- Professor R.G. Will & Dr. R. Knight Protein Biochemistry- Dr. M. Head Genetics- Mr. M. Bishop CSF Biochemistry- Dr. A. Green Epidemiology- Dr. H. Ward Care co-ordinator- Dr. B. Weller

34
Blood transmission studies: on going Tests of CJD Blood/ urine Screening vs. diagnostic

35
DIAGNOSTIC CRITERIA FOR vCJD IAProgressive neuropsychiatric disorder BDuration of illness > 6 months CRoutine investigations do not suggest an alternative diagnosis DNo history of potential iatrogenic exposure ENo evidence of a familial form of TSE IIAEarly psychiatric symptoms a BPersistent painful sensory symptoms b CAtaxia DMyoclonus or chorea or dystonia EDementia IIIAEEG does not show the typical appearance of sporadic CJD c (or no EEG performed) BBilateral pulvinar high signal on MRI scan IVAPositive tonsil biopsy d
 BBilateral pulvinar high signal on MRI scan IVAPositive tonsil biopsy d")
36
DEFINITE:I A and neuropathological confirmation of vCJD (spongiform change and extensive PrP deposition with florid plaques, throughout the cerebrum and cerebellum) PROBABLE:I and 4/5 of II and III A and III B OR I and IV A d POSSIBLE:I and 4/5 of II and III A a depression, anxiety, apathy, withdrawal, delusions. b this includes both frank pain and/or dysaesthesia. c generalised triphasic periodic complexes at approximately one per second. d tonsil biopsy is not recommended routinely, nor in cases with EEG appearances typical of sporadic CJD, but may be useful in suspect cases in which the clinical features are compatible with vCJD and MRI does not show bilateral pulvinar high signal. e spongiform change and extensive PrP deposition with florid plaques, throughout the cerebrum and cerebellum.

Similar presentations







 in Canada Pedro Piccardo, MD Division of Emerging and Transfusion-Transmitted Diseases Office of Blood Research.>")
 and Variant Creutzfeldt-Jakob.>")












, is a fatal brain disorder that occurs in cattle.>")

