Download presentation
Presentation is loading. Please wait.

1
Pancreas Transplant Pathology: Controversial Lesions Lois J. Arend PhD, MD University of Cincinnati Department of Pathology

2
American Journal of Transplantation 2008; 8: 1237–1249 Banff Schema for Grading Pancreas Allograft Rejection: Working Proposal by a Multi-Disciplinary International Consensus Panel C. B. Drachenberg, J. Odorico, A.J. Demetris, L. Arend, I. M. Bajema, J. A. Bruijn, D. Cantarovich, H. P. Cathro, J. Chapman, K. Dimosthenous, B. Fyfe-Kirschner, L. Gaber, O. Gaber, J. Goldberg, E. Honsova, S. S. Iskandar, D. K. Klassen, B. Nankivell, J. C. Papadimitriou, L. C. Racusen, P. Randhawa, F. P. Reinholt, K. Renaudin, P. P. Revelo, P. Ruiz, J. R. Torrealba, E. Vazquez-Martul, L. Voska, R. Stratta, S. T. Bartlett and D. E. R. Sutherland

3
1. Normal 2. Indeterminate 3. Cell-mediated rejection Acute cell-mediated rejection - Grade I/Mild acute cell-mediated rejection - Grade II/Moderate acute cell-mediated rejection - Grade III/Severe acute cell-mediated rejection Chronic active cell-mediated rejection 4. Antibody-mediated rejection = C4d + donor specific antibodies + graft dysfunction Hyperacute rejection Accelerated antibody-mediated rejection Acute antibody-mediated rejection Chronic active antibody-mediated rejection 5. Chronic allograft rejection/graft sclerosis - Stage I (mild graft sclerosis) - Stage II (moderate graft sclerosis) - Stage III (severe graft sclerosis) 6. Other histological diagnosis. e.g. CMV pancreatitis, PTLD, etc. Allograft Pancreas Grading American Journal of Transplantation 2008; 8: 1237–1249
 - Stage II (moderate graft sclerosis) - Stage III (severe graft sclerosis) 6. Other histological diagnosis. e.g. CMV pancreatitis, PTLD, etc. Allograft Pancreas Grading American Journal of Transplantation 2008; 8: 1237–1249.")
4
Outline Drug Toxicity Significance of C4d Labeling Significance of Acinar Inflammation Chronic Rejection/Sclerosis

5
Drug Toxicity Exocrine pancreas –Acute pancreatitis Anti-neoplastics, sulfonamides, diuretics, alcohol, azathioprine, oral contraceptives Acinar cell necrosis or apoptosis, inflammation, necrosis Endocrine pancreas – Diabetes Calcineurin inhibitors, thiazide diuretics Vacuolation, swelling, apoptosis of islet cells Reduced insulin staining of beta cells

6
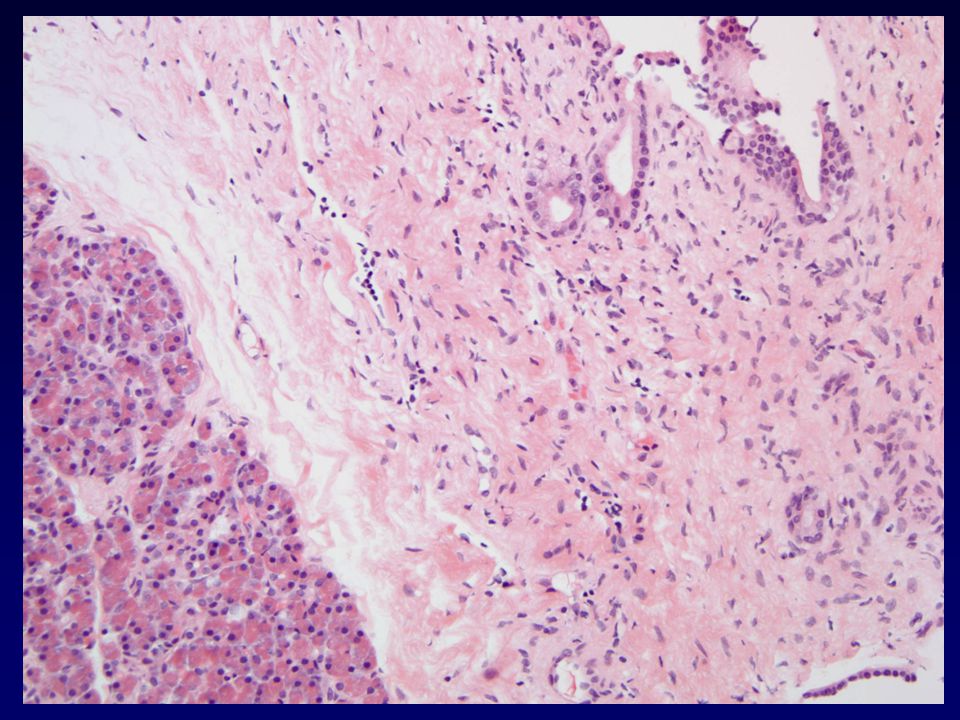
Exocrine Pancreas Acute pancreatitis –Drugs, duct obstruction, viruses, toxic chemicals, trauma Some features of acute pancreatitis can overlap with acute rejection Distinguishing between the two can be difficult Venulitis and more mononuclear dominant infiltrate favors rejection Many centers will treat for rejection if no clinical reason for pancreatitis is evident

7
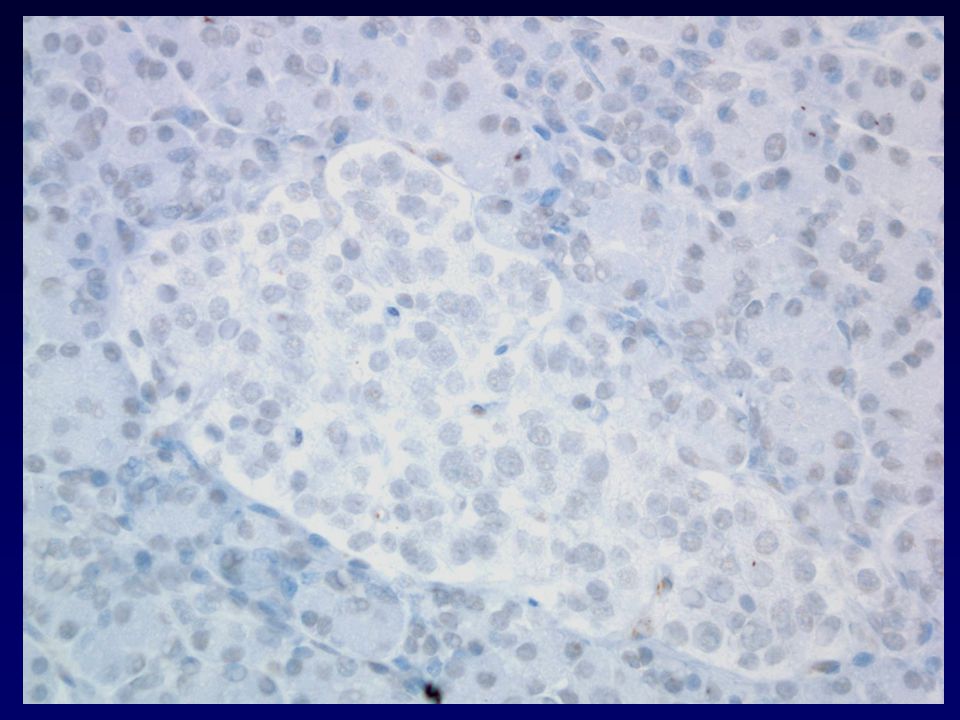
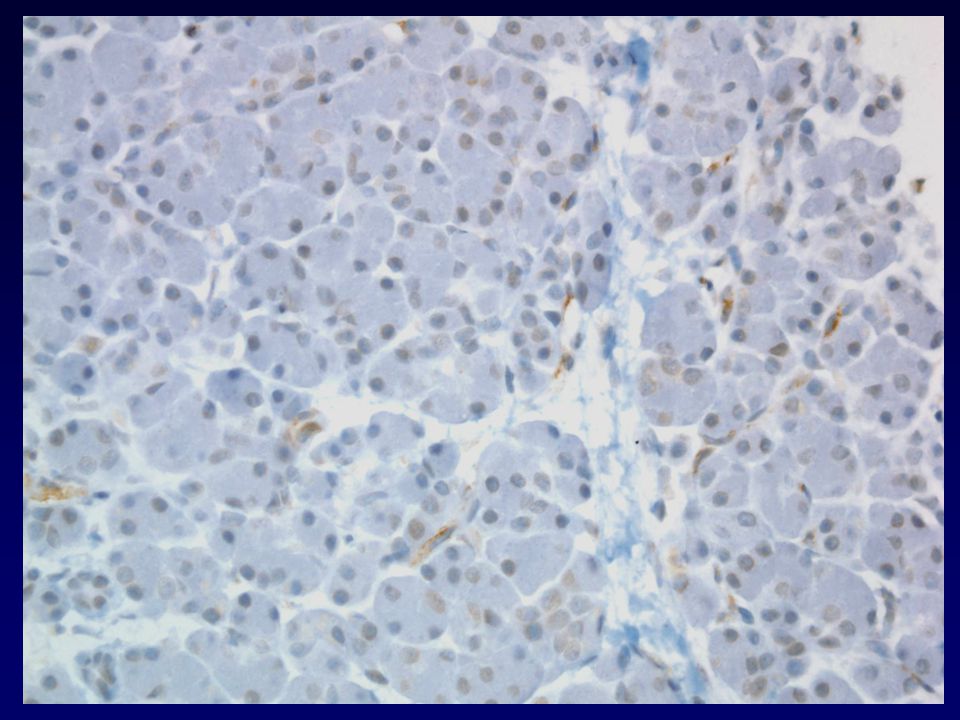
Endocrine Pancreas Diabetes –Caused by immunosuppressive agents No inflammation – vacuolation or drop-out –Caused by recurrent autoimmune disease Mononuclear cell infiltrate, similar to rejection –Should routine immunostaining be included as part of the grading scheme? Immunostaining for insulin and glucagon may not be routine at some centers

8
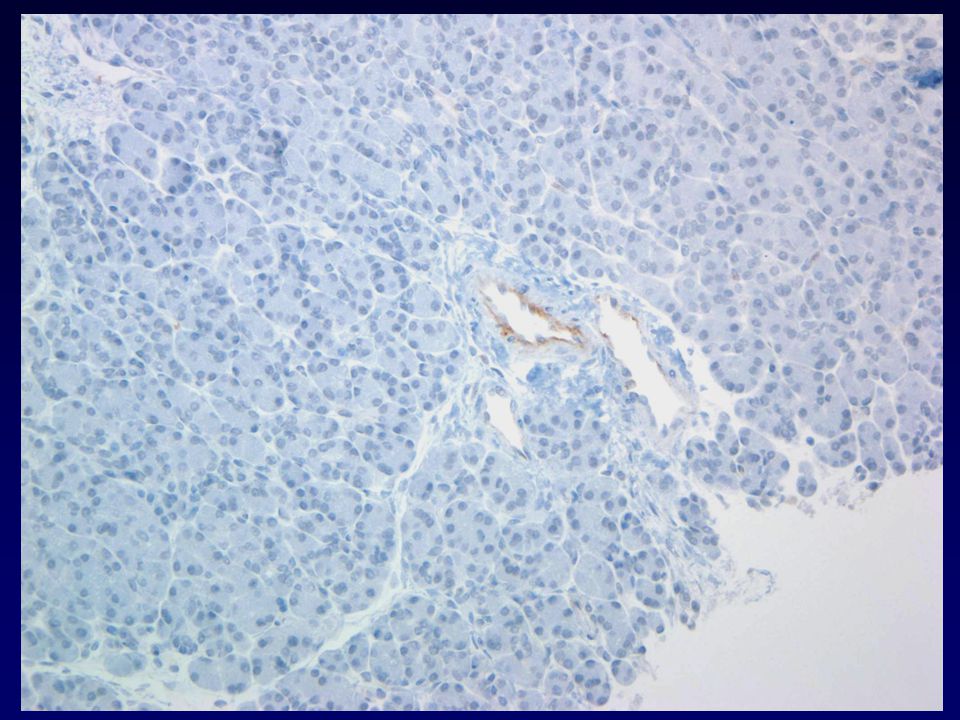
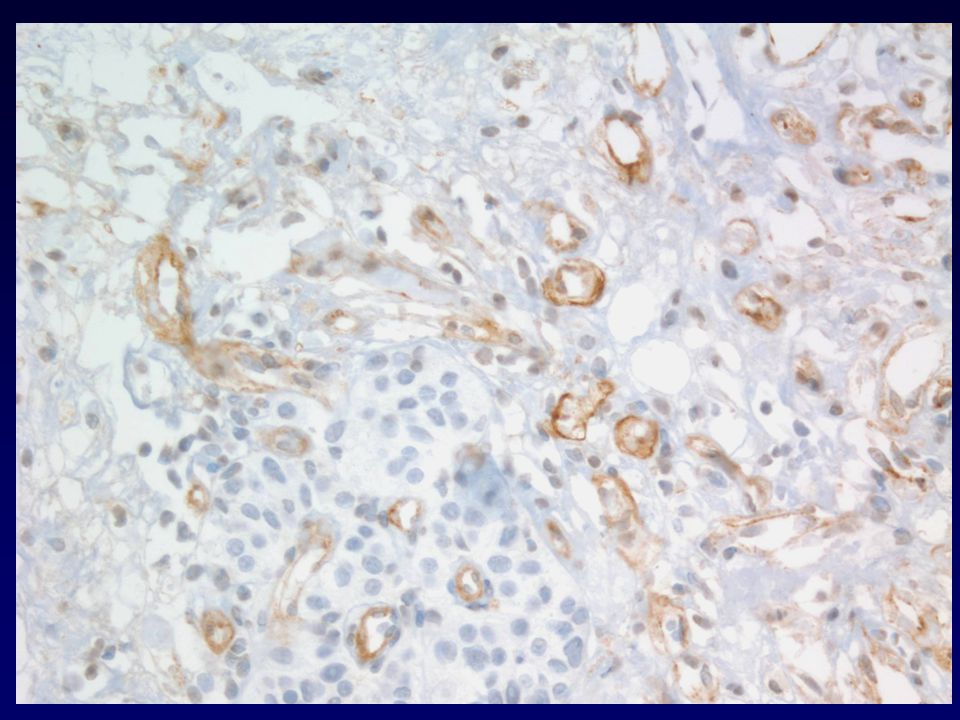
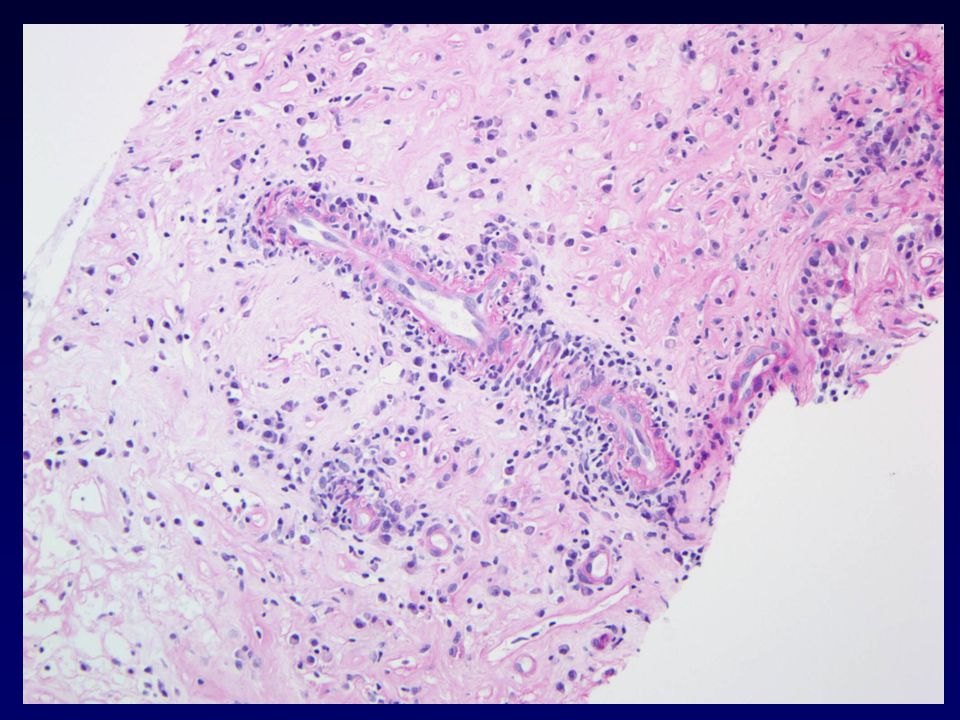
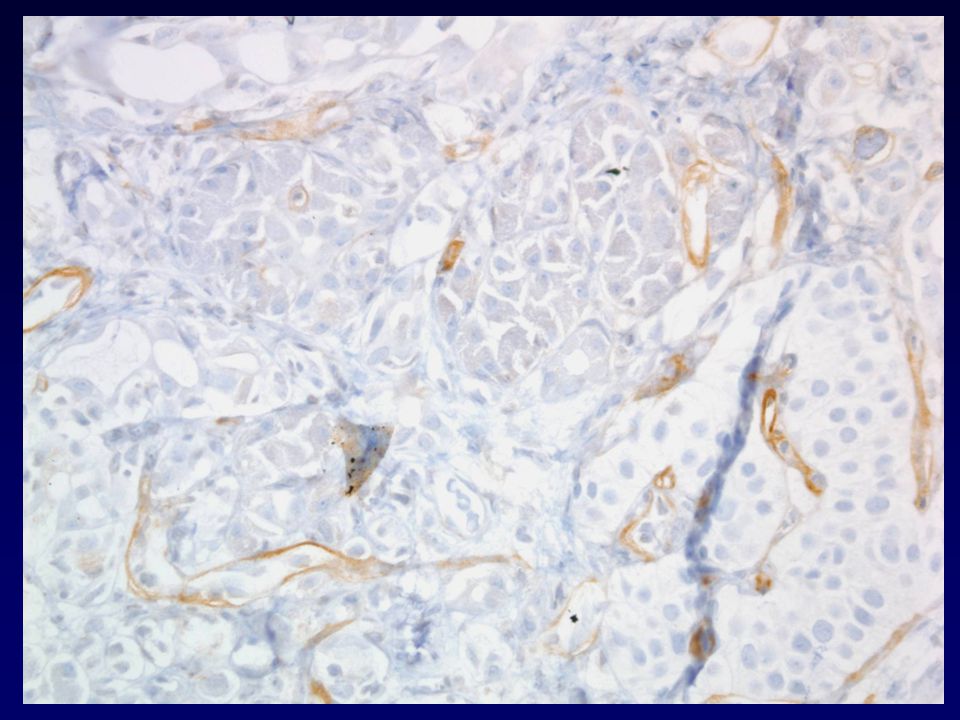
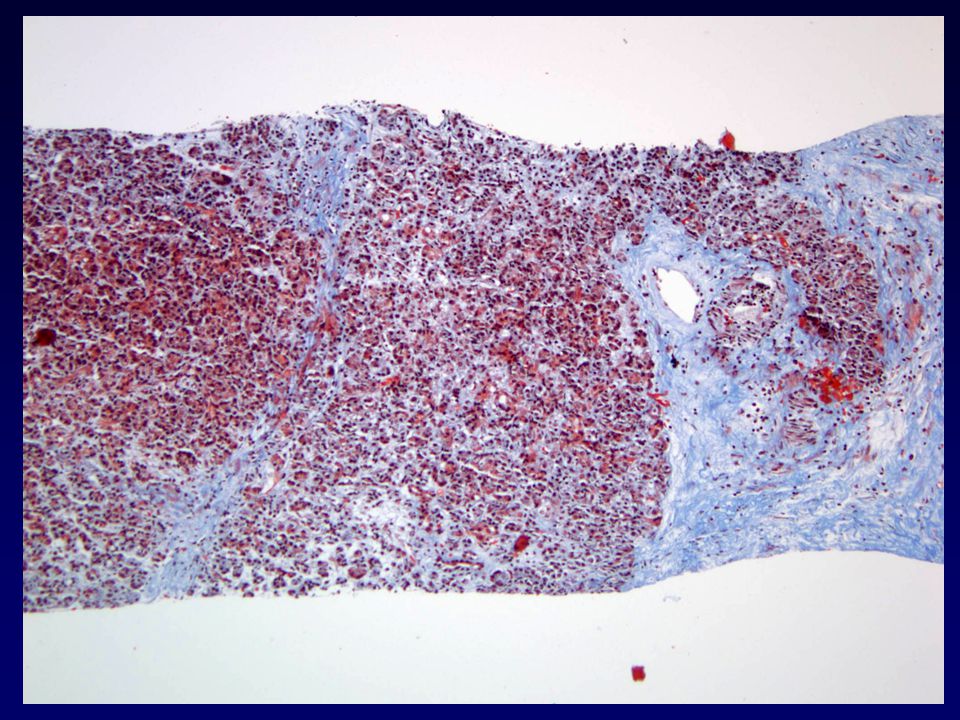
Significance of C4d Staining Antibody-mediated rejection, complement activation, deposition on endothelial cells –Indication of AMR Acute Chronic? Accessibility of staining by IHC on paraffin Non-specificity of paraffin section staining Frozen sections for IF?

9
Significance of C4d Staining Correlation between C4d+ IAC and: –Development of DSA –Allograft dysfunction C4d staining of artery intima or media, and interstitial collagen –No correlation with DSA or dysfunction Islet capillaries –No correlation with DSA or blood glucose C4d+ IAC correlated with DSA and graft dysfunction Torrealba, et al Transplantation 2008; 86: 1849

10
Retrospective Review of C4d Staining 2003 – 2009 22 biopsies with C4d immunostaining performed 2 cases with C4d+ IAC labeling No correlation with rejection grade –Sclerosing grade III; ACR III (old grade V) DSA not available
 DSA not available")
20
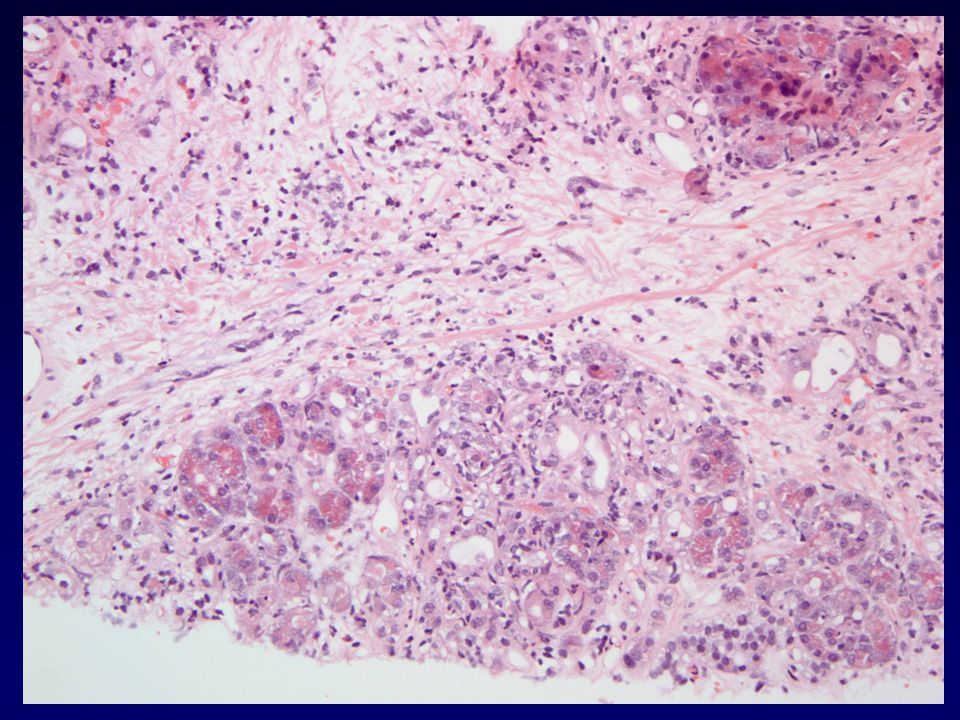
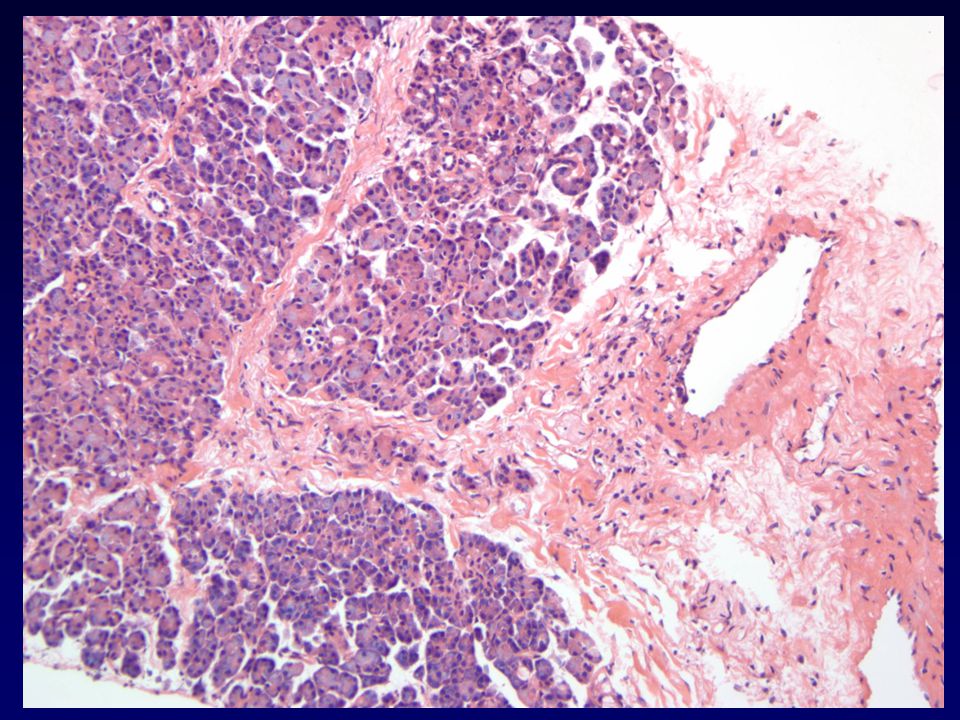
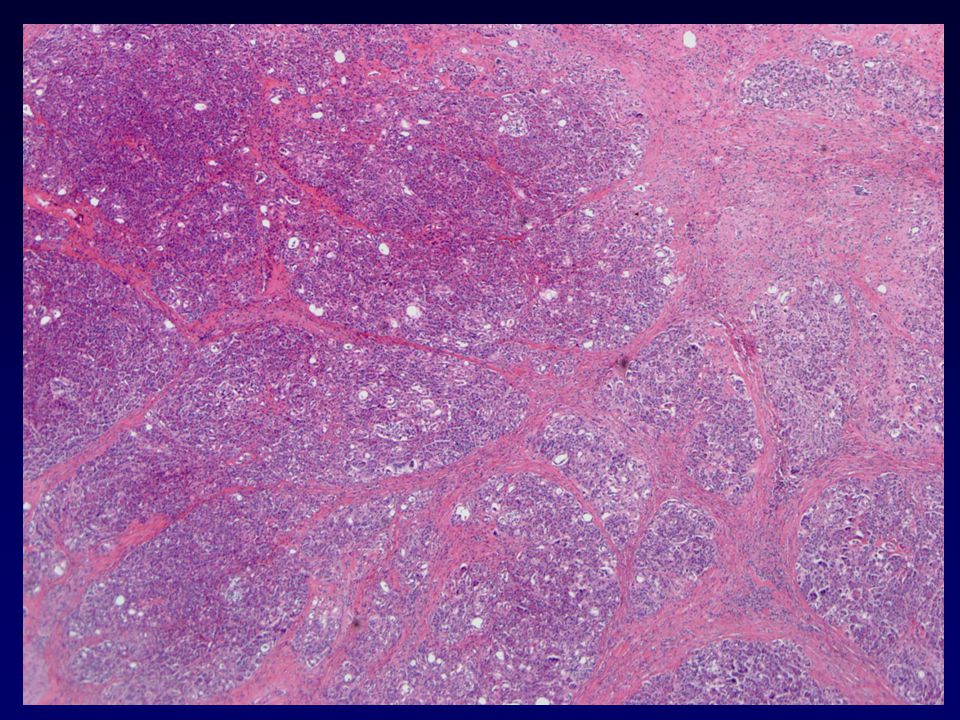
Significance of Acinar Inflammation – Mild acinar inflammation and injury to acinar cells (Grade I) Acinar injury easily leads to fibrosis Fibrosis -> poor prognosis
 Acinar injury easily leads to fibrosis Fibrosis -> poor prognosis")
21
Significance of Acinar Inflammation – Mayo clinic study 2 year period – 18 biopsies for grade II 25 follow-up biopsies 10 were unchanged, 1 grade III, 1 grade IV Conclusion: Grade II may not have unfavorable prognosis Casey, et al., Transpl, 2005

22
Significance of Acinar Inflammation – Minnesota study 8 year period – 914 pancreas grafts 80 grafts lost to chronic rejection 91% of these had prior rejection episode 70% with late functioning grafts had never had acute rejection Humar, et al., Transpl, 2003

23
Cincinnati Experience – Small sample Two cases with Grade II rejection One graft progressed to Stage III sclerosis in one year One graft progressed to Stage III sclerosis in nine months

24
1 month post-txp

26
4 months post-txp

27
7 months post-txp

28
10 months post-txp

30
12 months post-txp

32
Proposal – Should acinar inflammation of any degree be considered severe and treated aggressively? –Septal category of rejection –Acinar category –Arteritis category

33
Treatment of rejection Treat any form of pancreatic rejection aggressively –All but mildest cases treated with anti- thymocyte therapy Low threshold for treatment of pancreas rejection

34
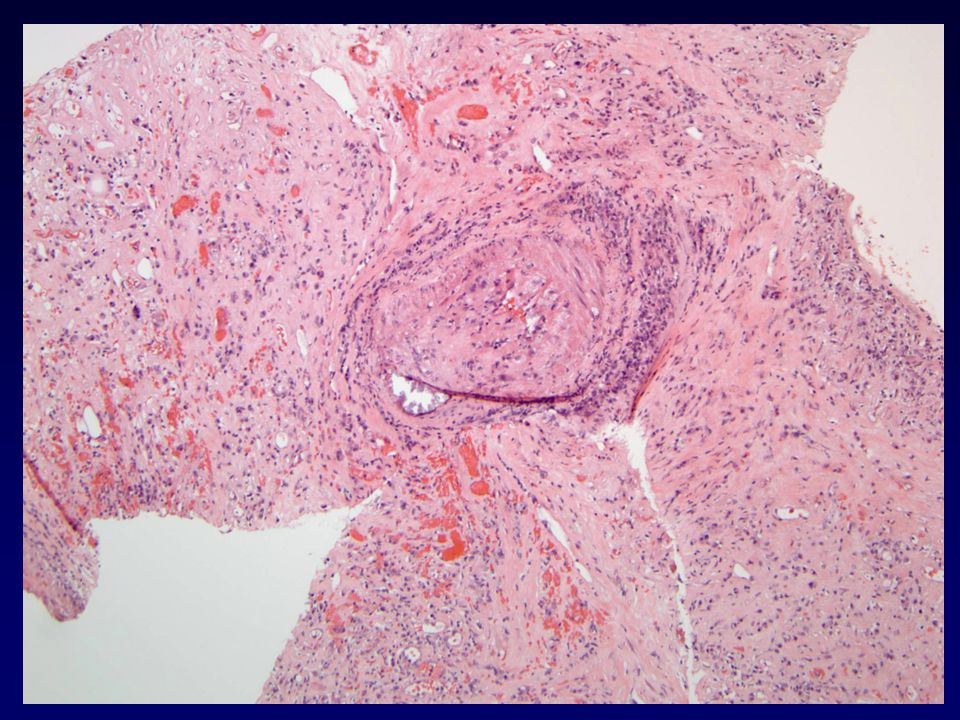
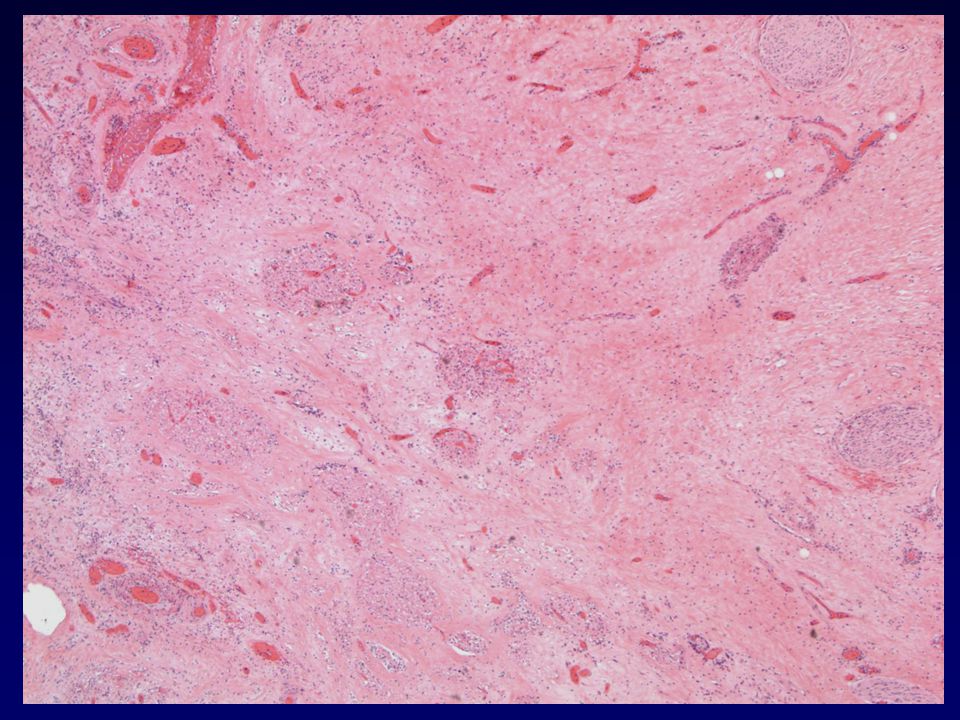
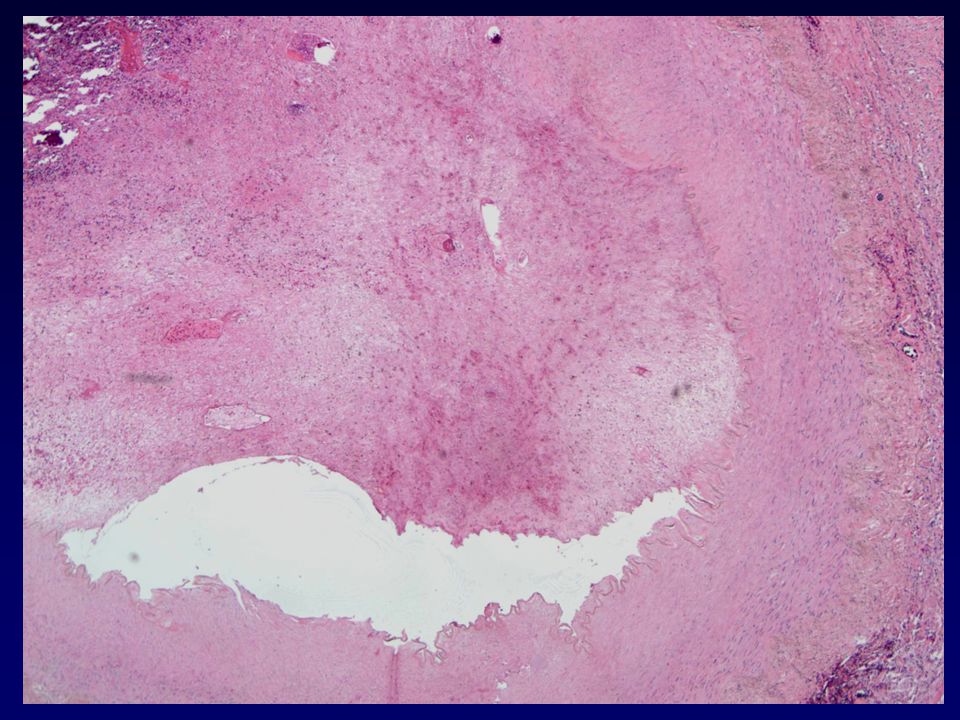
Chronic Rejection/Sclerosis Is graft sclerosis always due to rejection? Drug toxicity, infections, vascular complications Avoid CAN analog ?CAP Distinguish cause of sclerosis if possible

37
Summary Distinguishing rejection from many other insults can be difficult Significance of C4d+ unclear Any degree of acinar inflammation may benefit from early aggressive treatment Defining causes of chronic injury Rejection grade correlation with outcome

38
Acknowledgements Surgery Steve Woodle, MD Transplant Pharmacy Jason Everly, PharmD Rita Alloway, PharmD Nephrology Prabir Roy-Chaudhury, MD Gautham Mogilishetty, MD Amit Govil, MD Pathology Pravina Desai NEJM 356; 2007

Similar presentations








 EXOCRINE PANCREASE Lecture Dr. Gamal Hamra Wednesday 01/12/1430 (18/11/2009)>")

 Histopathologic findings Immunopathologic findings Immunohistochemistry on paraffin sections.>")
 inflammatory lesions 3.Changes in late post-transplant biopsies Banff 2001 ->")







