Download presentation
Presentation is loading. Please wait.

1
HLA Ab, Donor Reactivity and Risk of Rejection and Graft Loss HLA Ab, Donor Reactivity and Risk of Rejection and Graft Loss Ronald H. Kerman, PhD The University of Texas Medical School ~ Houston, TX Division of Immunology and Organ Transplantation Ronald H. Kerman, PhD The University of Texas Medical School ~ Houston, TX Division of Immunology and Organ Transplantation

2
Allograft Rejection Type: Hyperacute Accelerated Acute Chronic Type: Hyperacute Accelerated Acute Chronic Time: 0-48 hrs 5-7 days Early/delayed >60 days Time: 0-48 hrs 5-7 days Early/delayed >60 days Mediated by: Abs Abs/cells Cells/Abs Abs/cells/? Mediated by: Abs Abs/cells Cells/Abs Abs/cells/?

3
To identify clinically relevant recipient IgG HLA antibodies Responsibilities of the Histocompatibility Laboratory

4
Positive crossmatches, due to Abs or other factors not impacting on graft outcome, should not influence the donor- recipient pairing for transplantation.

5
Screen sera for reactivity vs target cells by cytotoxicity/fluorescence readouts. Use the most informative sera when performing the recipient vs donor crossmatch (historically most reactive, current and pretransplant sera). Screen sera for reactivity vs target cells by cytotoxicity/fluorescence readouts. Use the most informative sera when performing the recipient vs donor crossmatch (historically most reactive, current and pretransplant sera). Detection of Recipient Sensitization
. Screen sera for reactivity vs target cells by cytotoxicity/fluorescence readouts. Use the most informative sera when performing the recipient vs donor crossmatch (historically most reactive, current and pretransplant sera). Detection of Recipient Sensitization.")
6
NIH-CDC AHG-CDC Flow cytometry Membrane-dependent assays NIH-CDC AHG-CDC Flow cytometry Membrane-dependent assays Detection of Immunoglobulin Reactivity

7
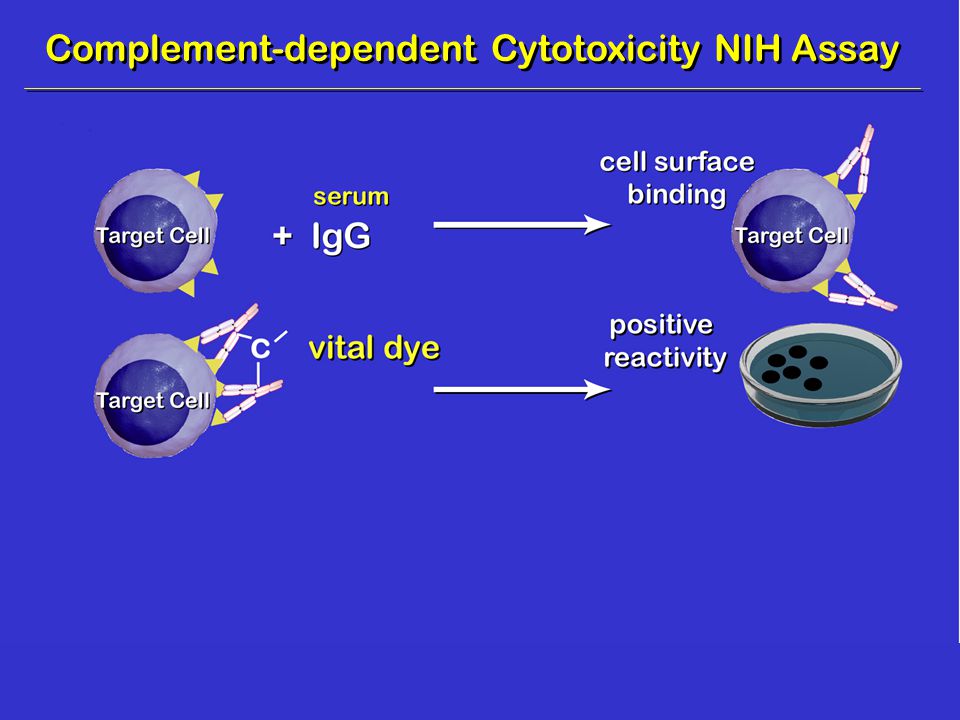
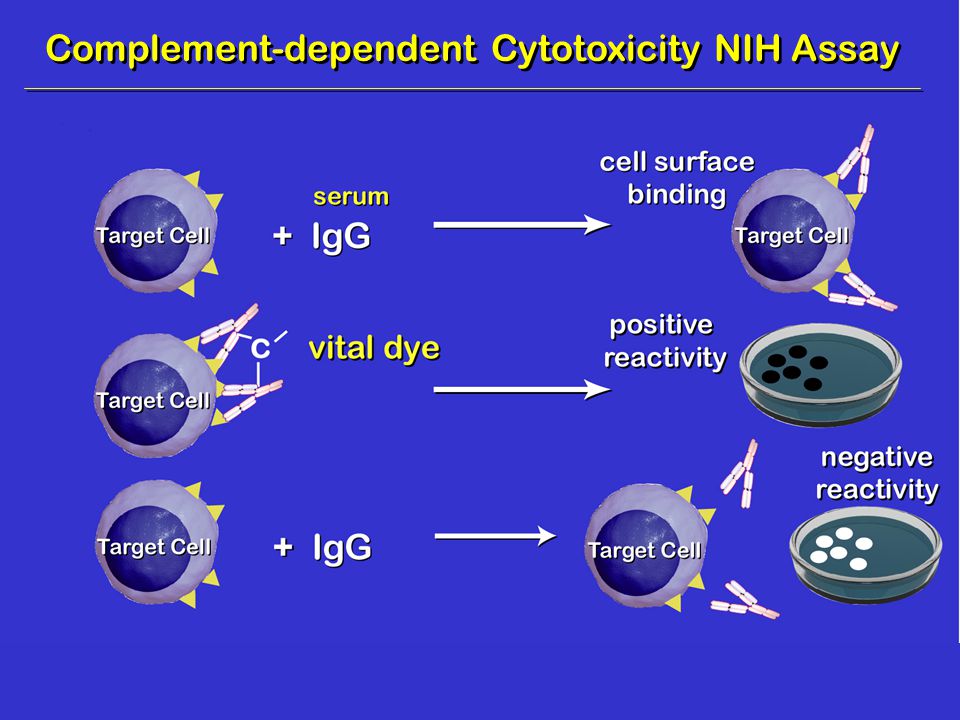
Complement-dependent Cytotoxicity NIH Assay

10
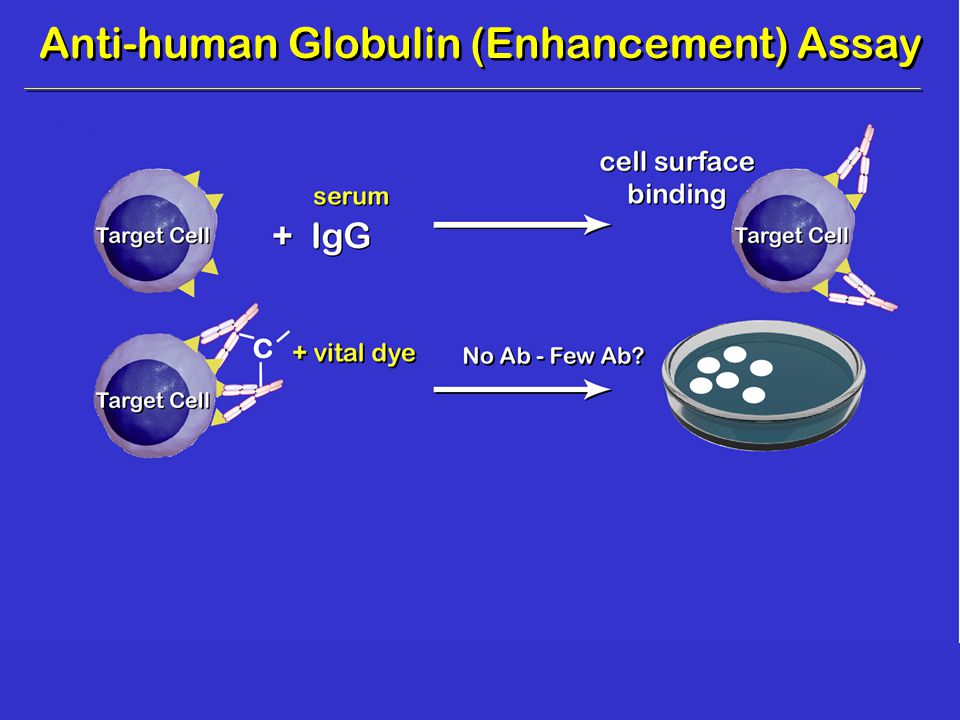
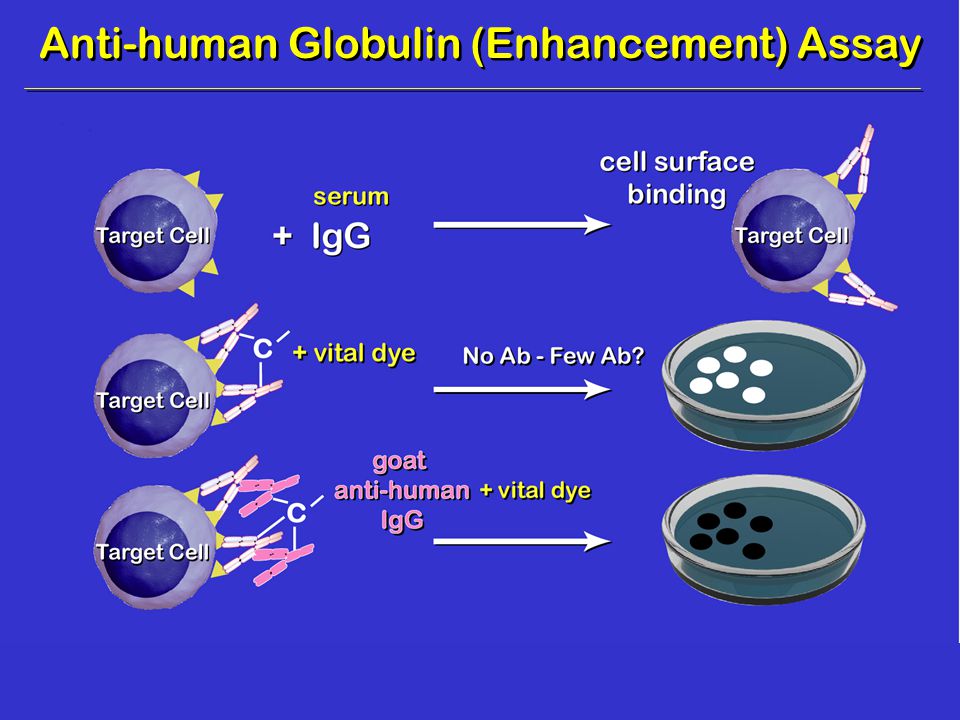
Anti-human Globulin (Enhancement) Assay
 Assay")
13
Flow Cytometry Assay NIH - CDCNegative AHG – CDCNegative Now measuring binding of IgG (absent C’) Flow Cytometry Assay NIH - CDCNegative AHG – CDCNegative Now measuring binding of IgG (absent C’)
 Flow Cytometry Assay NIH - CDCNegative AHG – CDCNegative Now measuring binding of IgG (absent C’)")
14
Cadaveric Renal Allograft Survival Among 1 o CsA-Pred Recipients at 12 months NIH Neg. n=166 81% (134/166) NIH Neg. n=166 81% (134/166) Kerman et al, Transplantation; 51:316, 1991 AHG Neg. Pos. n=151 n=15 82% 67% (124/151)(10/15) AHG Neg. Pos. n=151 n=15 82% 67% (124/151)(10/15) P<0.01
 NIH Neg. n=166 81% (134/166) Kerman et al, Transplantation; 51:316, 1991 AHG Neg. Pos. n=151 n=15 82% 67% (124/151)(10/15) AHG Neg. Pos. n=151 n=15 82% 67% (124/151)(10/15) P<0.01.")
15
Cadaveric Renal Allograft Survival Among 1 o CsA-Pred Recipients at 12 months AHG Pos. n=15 67% (10/15) AHG Pos. n=15 67% (10/15) Kerman et al, Transplantation; 51:316, 1991 DTE-AHG Neg.Pos. n=12n=3 83%0% (10/12)(0/3) DTE-AHG Neg.Pos. n=12n=3 83%0% (10/12)(0/3) P<0.01
 AHG Pos. n=15 67% (10/15) Kerman et al, Transplantation; 51:316, 1991 DTE-AHG Neg.Pos. n=12n=3 83%0% (10/12)(0/3) DTE-AHG Neg.Pos. n=12n=3 83%0% (10/12)(0/3) P<0.01.")
16
Cadaveric Renal Allograft Survival Among 1 o CsA-Pred Recipients at 12 months DTE/AHG XM Neg. n=166 81% DTE/AHG XM Neg. n=166 81% Kerman et al, Transplantation; 51:316, 1991 FCXM Neg.Pos. n=130n=3681% FCXM Neg.Pos. n=130n=3681%

17
Neg-NIH Extended XM: FCXM Study Ogura et al, Transplantation; 56:294, 1993 T-FCXM Pos. n=148 75% T-FCXM Pos. n=148 75% T-FCXM Neg. n=693 82% T-FCXM Neg. n=693 82% P<0.01

18
Could Ron Kerman have been wrong about his crossmatch results and interpretation?

19
Kerman et al, Transplantation; 68:1855, 1999 0 0 5 5 10 15 20 25 30 35 40 45 50 Negative (n=56) Negative (n=56) Positive (n=41) Positive (n=41) P=NS % Rejection IgG FCXM: Renal Allograft Study Frequency of Rejection in a Single Center IgG FCXM: Renal Allograft Study Frequency of Rejection in a Single Center
 Negative (n=56) Positive (n=41) Positive (n=41) P=NS % Rejection IgG FCXM: Renal Allograft Study Frequency of Rejection in a Single Center IgG FCXM: Renal Allograft Study Frequency of Rejection in a Single Center")
20
Could Ron Kerman have been wrong about his crossmatch results and interpretation? I don’t think so!

21
The Cell Surface Is a Jungle HLA

22
NIH-CDC AHG-CDC Flow cytometry NIH-CDC AHG-CDC Flow cytometry Membrane-dependent Assays Detection of membrane receptors may not be related to HLA!

23
ELISA-determined IgG HLA Abs vs MHC-I (pooled platelets) ELISA-determined IgG HLA Abs vs MHC-I/II (PBL cultures) Flow bead PRA-determined IgG HLA vs I/II (soluble HLA I/II antigens on microbeads measured by cytometry) ELISA-determined IgG HLA Abs vs MHC-I (pooled platelets) ELISA-determined IgG HLA Abs vs MHC-I/II (PBL cultures) Flow bead PRA-determined IgG HLA vs I/II (soluble HLA I/II antigens on microbeads measured by cytometry) Membrane-independent Assays
 ELISA-determined IgG HLA Abs vs MHC-I/II (PBL cultures) Flow bead PRA-determined IgG HLA vs I/II (soluble HLA I/II antigens on microbeads measured by cytometry) ELISA-determined IgG HLA Abs vs MHC-I (pooled platelets) ELISA-determined IgG HLA Abs vs MHC-I/II (PBL cultures) Flow bead PRA-determined IgG HLA vs I/II (soluble HLA I/II antigens on microbeads measured by cytometry) Membrane-independent Assays")
24
PRA by Different Methodologies Type: CDC AHG-CDC ELISA Flow Type: CDC AHG-CDC ELISA Flow Positive 102 116 127 139 Positive 102 116 127 139 Negative 162 148 137 125 Negative 162 148 137 125 Gebel & Bray, Transplantation; 69:1370, 2000

25
AHG-PRA vs Rejection 493 Consecutive CAD Recipients AHG-PRA vs Rejection 493 Consecutive CAD Recipients Rejection YES NO Rejection YES NO AHG-PRA P=NS <10% 134 159 <10% 134 159 10% 100 10% 100

26
ELISA-PRA and Rejection Rejection YES NO Rejection YES NO ELISA-PRA P<0.001 <10% 38 168 <10% 38 168 10% 117 63 10% 117 63

27
Correlation Between % ELISA-PRA and Graft Survival Graft Survival (months) 12 24 36 Graft Survival (months) 12 24 36 ELISA-PRA P<0.01 <10% (n=312) 85% 82% 81% <10% (n=312) 85% 82% 81% >10% (n=181) 74% 70% 67% >10% (n=181) 74% 70% 67% P<0.01
 Graft Survival (months) ELISA-PRA P<0.01 <10% (n=312) 85% 82% 81% <10% (n=312) 85% 82% 81% >10% (n=181) 74% 70% 67% >10% (n=181) 74% 70% 67% P<0.01")
28
Sensitivity and sensitization, defining the unsensitized patient Application of membrane-independent assays to identify HLA antibodies Sensitivity and sensitization, defining the unsensitized patient Application of membrane-independent assays to identify HLA antibodies Gebel & Bray, Transplantation; 69:1370, 2000

29
Tambur et al, Transplantation; 70:1055, 2000 Correlation of Pre-transplant Abs Detected by Flow PRA with Biopsy-documented Cardiac Rejection

30
Kerman et al, Transplantation; 68:1855, 1999 0 0 5 5 10 15 20 25 30 35 40 45 50 Negative (n=56) Negative (n=56) Positive (n=41) Positive (n=41) P=NS % Rejection IgG FCXM: Renal Allograft Study Frequency of Rejection in a Single Center IgG FCXM: Renal Allograft Study Frequency of Rejection in a Single Center Were positive crossmatches due to HLA Abs?
 Negative (n=56) Positive (n=41) Positive (n=41) P=NS % Rejection IgG FCXM: Renal Allograft Study Frequency of Rejection in a Single Center IgG FCXM: Renal Allograft Study Frequency of Rejection in a Single Center Were positive crossmatches due to HLA Abs")
31
Neoral - CsA Steroids Prograf - FK506 Cellcept - MMF Rapamycin - Sirolimus Thymoglobulin OKT3, anti-IL-2R, FTY720 Neoral - CsA Steroids Prograf - FK506 Cellcept - MMF Rapamycin - Sirolimus Thymoglobulin OKT3, anti-IL-2R, FTY720 Immunosuppressive Menu:

32
If new immunosuppressive therapies reduce the incidence of acute rejection, are pre-Tx HLA antibodies clinically relevant?

33
RAPA-CsA-Pred treated primary recipients of CAD renal allografts experience fewer acute rejections vs CsA-Pred recipients. We therefore tested their pre-Tx sera for the presence of HLA Abs and correlated the results to the occurrence of rejection during the first 12 months post-transplant. RAPA-CsA-Pred treated primary recipients of CAD renal allografts experience fewer acute rejections vs CsA-Pred recipients. We therefore tested their pre-Tx sera for the presence of HLA Abs and correlated the results to the occurrence of rejection during the first 12 months post-transplant.

34
147 RAPA-CsA-Pred recipients were studied 48 patients were chosen specifically because they had a rejection episode. 99 patients were chosen because they had not experienced a rejection episode during the first year post-transplant. 147 RAPA-CsA-Pred recipients were studied 48 patients were chosen specifically because they had a rejection episode. 99 patients were chosen because they had not experienced a rejection episode during the first year post-transplant.

35
PRA Testing Anti-human globulin (AHG) ELISA (One Lambda, Inc. LAT) Flow PRA (One Lambda, Inc.) PRA Testing Anti-human globulin (AHG) ELISA (One Lambda, Inc. LAT) Flow PRA (One Lambda, Inc.)
 Flow PRA (One Lambda, Inc.) PRA Testing Anti-human globulin (AHG) ELISA (One Lambda, Inc. LAT) Flow PRA (One Lambda, Inc.).")
36
AHG-PRA detected 18 reactive sera ELISA-PRA detected 25 reactive sera (11 vs HLA class I, 3 vs II, 11 vs I/II) Flow PRA detected 59 reactive sera (31 vs HLA class I, 9 vs II, 19 vs I/II) AHG-PRA detected 18 reactive sera ELISA-PRA detected 25 reactive sera (11 vs HLA class I, 3 vs II, 11 vs I/II) Flow PRA detected 59 reactive sera (31 vs HLA class I, 9 vs II, 19 vs I/II) Results:
 Flow PRA detected 59 reactive sera (31 vs HLA class I, 9 vs II, 19 vs I/II) AHG-PRA detected 18 reactive sera ELISA-PRA detected 25 reactive sera (11 vs HLA class I, 3 vs II, 11 vs I/II) Flow PRA detected 59 reactive sera (31 vs HLA class I, 9 vs II, 19 vs I/II) Results:")
37
There was no significant correlation between AHG-PRA, ELISA-detected HLA Abs, and Flow PRA HLA class II Abs and rejection. AHG vs RejectionP=NS LAT-I vs RejectionP=NS LAT-II vs RejectionP=NS LAT-I/II vs RejectionP=NS F-II vs RejectionP=NS AHG vs RejectionP=NS LAT-I vs RejectionP=NS LAT-II vs RejectionP=NS LAT-I/II vs RejectionP=NS F-II vs RejectionP=NS

38
Rejection NO YES Rejection NO YES Flow PRA-1 X 2 =15.7; P<0.001 <5% 76 21 <5% 76 21 5% 23 27 5% 23 27

39
Flow PRA 0% Flow PRA 0% No grafts lost (+) FCXM vs non-HLA Ab No grafts lost (+) FCXM vs non-HLA Ab Day of 1st Rejection 57 ± 34 Day of 1st Rejection 57 ± 34 FCXM Pos.Neg. 28 FCXM Pos.Neg. 28

40
Flow PRA 13 ± 9% Flow PRA 13 ± 9% No grafts lost. Day of 1st Rejection 55 ± 31 Day of 1st Rejection 55 ± 31 FCXM Pos.Neg. -30 FCXM Pos.Neg. -30

41
Flow PRA 28 ± 9% Flow PRA 28 ± 9% (+) HLA Ab and (-) FCXM: rejection, no grafts lost. (+) HLA Ab and (+) FCXM: rejection, 58% (7/12) grafts lost. (+) HLA Ab and (-) FCXM: rejection, no grafts lost. (+) HLA Ab and (+) FCXM: rejection, 58% (7/12) grafts lost. Day of 1st Rejection 32 ± 15 Day of 1st Rejection 32 ± 15 FCXM Pos.Neg. 1213 FCXM Pos.Neg. 1213
 HLA Ab and (+) FCXM: rejection, 58% (7/12) grafts lost. (+) HLA Ab and (-) FCXM: rejection, no grafts lost. (+) HLA Ab and (+) FCXM: rejection, 58% (7/12) grafts lost. Day of 1st Rejection 32 ± 15 Day of 1st Rejection 32 ± 15 FCXM Pos.Neg FCXM Pos.Neg")
42
Flow PRA 48 ± 31% Flow PRA 48 ± 31% (+) HLA Ab and (-) FCXM: rejection, no grafts lost. (+) HLA Ab and (+) FCXM: rejection, 63% (5/8) lost to AMR. (+) HLA Ab and (-) FCXM: rejection, no grafts lost. (+) HLA Ab and (+) FCXM: rejection, 63% (5/8) lost to AMR. Day of 1st Rejection 17 ± 12 Day of 1st Rejection 17 ± 12 FCXM Pos.Neg. 87 FCXM Pos.Neg. 87
 HLA Ab and (+) FCXM: rejection, 63% (5/8) lost to AMR. (+) HLA Ab and (-) FCXM: rejection, no grafts lost. (+) HLA Ab and (+) FCXM: rejection, 63% (5/8) lost to AMR. Day of 1st Rejection 17 ± 12 Day of 1st Rejection 17 ± 12 FCXM Pos.Neg. 87 FCXM Pos.Neg. 87.")
43
% PRA 0 13 ± 9 28 ± 9 48 ± 31 % PRA 0 13 ± 9 28 ± 9 48 ± 31 % Rejection 5% (4/75) 13% (4/32) 100% % Rejection 5% (4/75) 13% (4/32) 100% Day of Rejection 57 ± 34 55 ± 31 32 ± 9 17 ± 12 Day of Rejection 57 ± 34 55 ± 31 32 ± 9 17 ± 12 N 75 32 25 15 N 75 32 25 15
 13% (4/32) 100% % Rejection 5% (4/75) 13% (4/32) 100% Day of Rejection 57 ± ± ± 9 17 ± 12 Day of Rejection 57 ± ± ± 9 17 ± 12 N N")
44
1. Assays that measure binding of immunoglobulin to targets may not represent HLA Ab reactivity. 2. The AHG-XM protects RAPA-CsA-Pred recipients from hyperacute rejection. 3. The Flow PRA assay detects clinically relevant HLA Abs associated with rejection and/or graft loss. 1. Assays that measure binding of immunoglobulin to targets may not represent HLA Ab reactivity. 2. The AHG-XM protects RAPA-CsA-Pred recipients from hyperacute rejection. 3. The Flow PRA assay detects clinically relevant HLA Abs associated with rejection and/or graft loss.

45
4. How many antibodies are present may be clinically relevant. 5. The antibody titer may also be important. 6. Patients with pre-Tx (+) HLA Abs and (+) donor reactivity (+ FCXM) are at risk for graft rejection and loss. 4. How many antibodies are present may be clinically relevant. 5. The antibody titer may also be important. 6. Patients with pre-Tx (+) HLA Abs and (+) donor reactivity (+ FCXM) are at risk for graft rejection and loss.
 HLA Abs and (+) donor reactivity (+ FCXM) are at risk for graft rejection and loss. 4. How many antibodies are present may be clinically relevant. 5. The antibody titer may also be important. 6. Patients with pre-Tx (+) HLA Abs and (+) donor reactivity (+ FCXM) are at risk for graft rejection and loss..")
46
We have performed heart transplantation following a negative AHG-XM. We evaluated the clinical relevance of FCXM for heart recipients. We have performed heart transplantation following a negative AHG-XM. We evaluated the clinical relevance of FCXM for heart recipients.

47
IgG FCXM IgG FCXM Neg. Neg. 1YGS 86% IgG FCXM IgG FCXM Neg. Neg. 1YGS 86% Of the 22 IgG FCXM-Pos. Recipients: 7 grafts were lost 15 grafts were successful WHY? Of the 22 IgG FCXM-Pos. Recipients: 7 grafts were lost 15 grafts were successful WHY? FCXM Results: Heart Recipient IgG FCXM Pos. 68% IgG FCXM Pos. 68% P<0.02

48
5 sera tested from lost grafts All 5 sera were Flow PRA reactive vs MHC I (Flow PRAs of 36%, 52%, 68%, 50% and 49%) 11 sera tested from successful recipients All 11 sera were Flow PRA non-reactive 5 sera tested from lost grafts All 5 sera were Flow PRA reactive vs MHC I (Flow PRAs of 36%, 52%, 68%, 50% and 49%) 11 sera tested from successful recipients All 11 sera were Flow PRA non-reactive We Flow PRA Tested the IgG FCXM-Pos. Sera

49
Graft Survival 12 mo. Graft Survival 12 mo. FCXM (+) Flow PRA I/II 51% 55% (5/9) FCXM (+) Flow PRA I/II 51% 55% (5/9) Rejection 0-12 mo. 89% (8/9) 31% (4/13) FCXM (-) Flow PRA I/II 51% 100% (13/13) FCXM (-) Flow PRA I/II 51% 100% (13/13) Both comparisons p<0.01
 Flow PRA I/II 51% 55% (5/9) FCXM (+) Flow PRA I/II 51% 55% (5/9) Rejection 0-12 mo. 89% (8/9) 31% (4/13) FCXM (-) Flow PRA I/II 51% 100% (13/13) FCXM (-) Flow PRA I/II 51% 100% (13/13) Both comparisons p<0.01.")
50
1. HLA Ab negative, FCXM negative (at risk for reversible, cellular rejection) 2. HLA Ab negative, FCXM positive (non-HLA allo-Ab - at risk for reversible, cellular rejection) 1. HLA Ab negative, FCXM negative (at risk for reversible, cellular rejection) 2. HLA Ab negative, FCXM positive (non-HLA allo-Ab - at risk for reversible, cellular rejection) HLA Ab and Donor Specific Reactivity Rank Order of Risk HLA Ab and Donor Specific Reactivity Rank Order of Risk
 1. HLA Ab negative, FCXM negative (at risk for reversible, cellular rejection) 2. HLA Ab negative, FCXM positive (non-HLA allo-Ab - at risk for reversible, cellular rejection) HLA Ab and Donor Specific Reactivity Rank Order of Risk HLA Ab and Donor Specific Reactivity Rank Order of Risk.")
51
3. HLA Ab positive, FCXM negative (at risk for reversible, cellular, +/- HLA Ab, rejection) 4. HLA Ab positive, FCXM positive (at risk for humoral/cellular rejection and graft loss) 3. HLA Ab positive, FCXM negative (at risk for reversible, cellular, +/- HLA Ab, rejection) 4. HLA Ab positive, FCXM positive (at risk for humoral/cellular rejection and graft loss) HLA Ab and Donor Specific Reactivity Rank Order of Risk HLA Ab and Donor Specific Reactivity Rank Order of Risk
 3. HLA Ab positive, FCXM negative (at risk for reversible, cellular, +/- HLA Ab, rejection) 4. HLA Ab positive, FCXM positive (at risk for humoral/cellular rejection and graft loss) HLA Ab and Donor Specific Reactivity Rank Order of Risk HLA Ab and Donor Specific Reactivity Rank Order of Risk.")
52
To transplant or not to transplant, that is the question! Whether it is nobler in the minds of transplant surgeons to treat with thymoglobulin, OKT3, Plasmapheresis, IVIg, or the kitchen sink!

53
1. Pre-transplant identification of immunologically high risk patients. Consideration of induction and/or maintenance immunosuppression. 2. Clarify the role of HLA antibody in rejection episodes (including the role of C4d ). 1. Pre-transplant identification of immunologically high risk patients. Consideration of induction and/or maintenance immunosuppression. 2. Clarify the role of HLA antibody in rejection episodes (including the role of C4d ). Applications
. 1. Pre-transplant identification of immunologically high risk patients. Consideration of induction and/or maintenance immunosuppression. 2. Clarify the role of HLA antibody in rejection episodes (including the role of C4d ). Applications.")
54
3. Transplantation of highly sensitized and/or positive crossmatch recipients. 4. Long term monitoring of the presence of HLA antibody and graft outcome. 3. Transplantation of highly sensitized and/or positive crossmatch recipients. 4. Long term monitoring of the presence of HLA antibody and graft outcome. Applications

55
“I have never let my schooling interfere with my education.” -Mark Twain “I have never let my schooling interfere with my education.” -Mark Twain

Similar presentations


 Anti-A11 and B44.>")






: 1045-1095.>")









