Download presentation
Presentation is loading. Please wait.

1
Chronic Constipation: Update in Management Abdulwahab Telmesani FRCPC,FAAP Faculty of Medicine and Medical Science Umm Al-Qura University

2
Chronic constipation 3% of the visits to general pediatrics. 25% of the visits to pediatrics G.I.

3
Definition Infrequent stool Hard stool Large stool

4
Definition NASPGAN: A delay or difficulty in defecation present for 2 or more weeks and sufficient to cause significant distress to the patient.

5
Normal frequency of bowel movement

6
Epidemiology: The prevalence of childhood constipation in the general population ranged from 0.7% to 29.6% Maartje M. et al Am J Gastroenterol 2006

7
Epidemiology: constipation correlated with low maternal education, female sex, living in a large community and having no older siblings. JONAS F et. al. Acta Pædiatrica, 2006

8
Exclusive breast fed babies In conclusion, infrequent bowel movements in young infants fed exclusively breast milk can be a harmless phenomenon that can easily diagnosed by history and careful examination of the infant. Yon Ho Choe et al Eur J Pediatr (2004)
.")
9
Functional constipation in infants: a follow-up study We conclude that most infants with severe constipation evaluated at a tertiary center are recovered after 6 months. Early therapeutic intervention may beneficially contribute to the resolution of constipation. van den Berg MM et al J Pediatr 2005

10
Trend in family / Genetic Prominent family history of constipation. Identical twins have 6 times folds possibility than non identicals.

12
Chronic constipation Functional / non organic is most common Organic is rare ( except in infancy)
")
13
Functional / non organic constipation What cause it / start it?

14
Functional / non organic constipation Inappropriate toilet training Anal fissure / Anusitis Avoidance of response to nature call Inconvenient / uncomfortable places Behavioral Vicious cycle of retention development.

19
Encopresis: Incontinence of stool of non organic Origin (rare before 3 years)
")
20
Organic Causes of Chronic constipation: What are the causes?

22
Chronic constipation in children: Organic disorders are a major cause A significant number of the children with chronic treatment-resistant constipation may have organic causes (slow colonic transit and outlet obstruction) and suggests new approaches to the management of children with chronic treatment-resistant constipation. BR Southwell et al J. Paediatr. Child Health (2005)
.")
23
Stool withholding presenting as a cause of non-epileptic seizures Anthony Cohn Developmental Medicine and Child Neurology; Oct 2005

24
chronic constipation and food hypersensitivity An increasing number of reports suggest a relationship between refractory chronic constipation and food allergy in children. CARROCCIO & G. IACONO Alimentary Pharmacology & Therapeutics 2006

26
Evaluation

27
History. Physical examination.

28
History: Meconium passage. Frequency of bowel movement. Diet. School / travel. Painful defecation. Family history. FTT. Clogging of the commode.

29
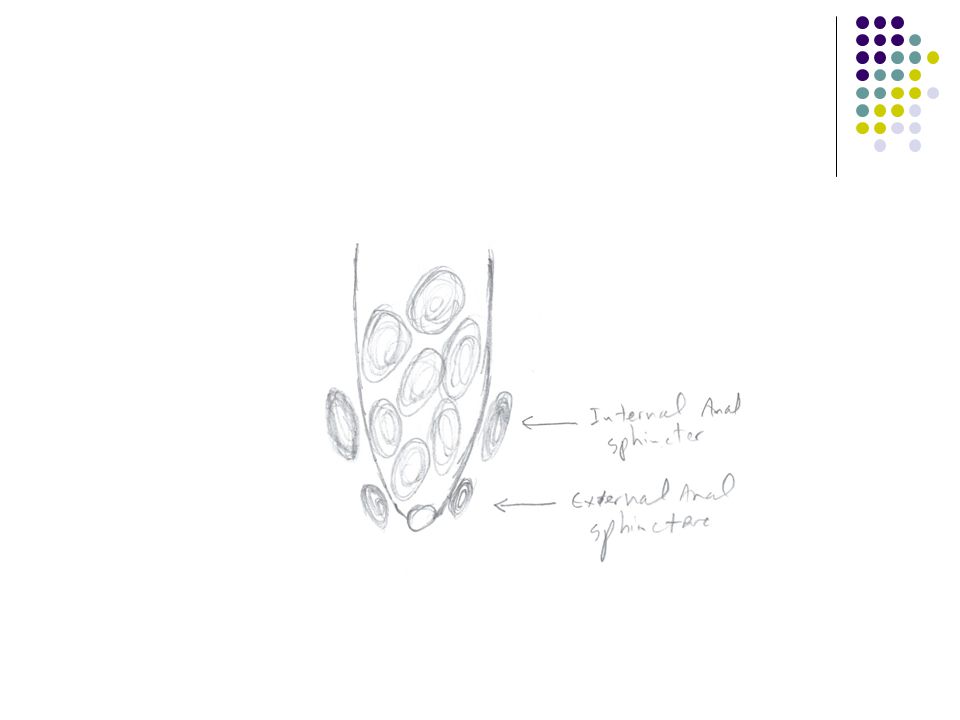
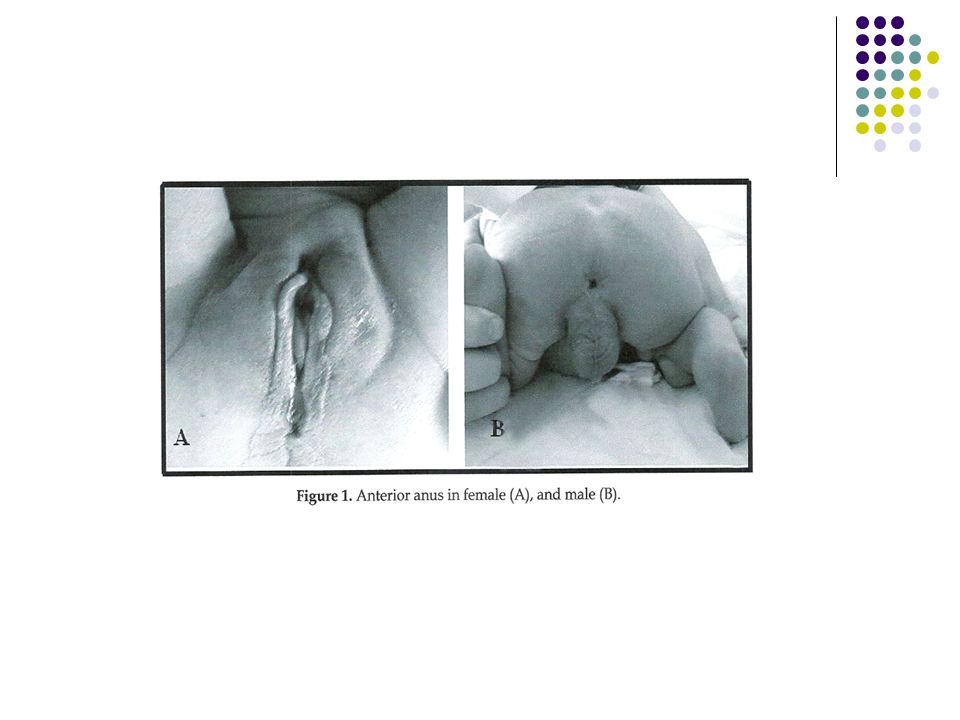
Physical examination: Growth Abd. Distention Fecal mass felt on abd. exam. Rectum full of stool Fecal soiling. Anogenital index

31
Anogenital index: Distance in centimeters: from the vagina or scrotum to the anus _______________________________ from the vagina or scrotum to the coccyx. Females: 0.39 ± 0.09, Males: 0.56 ± 0.2.

33
Physical examination: Anal fissure / anusitis. Signs of trauma (abuse). Signs of spinal defects( spina bifida) Neurological assessment of L.L. and anal wenk
 Neurological assessment of L.L. and anal wenk.")
34
Myelomeningocele

35
Spina bifida

36
Tethered cord syndrome

37
Neurofibromatosis

39
Investigations

40
Investigations: Non is required routinely.

41
Investigations: Stool analysis ??? Whyyyy

42
Investigations: Plain abdominal X RAY. ( obese child or refusing exam) Lumbosacral X RAY / MRI Ba. Enema Rectal biopsy. T4, Na, K, Osmolality.

43
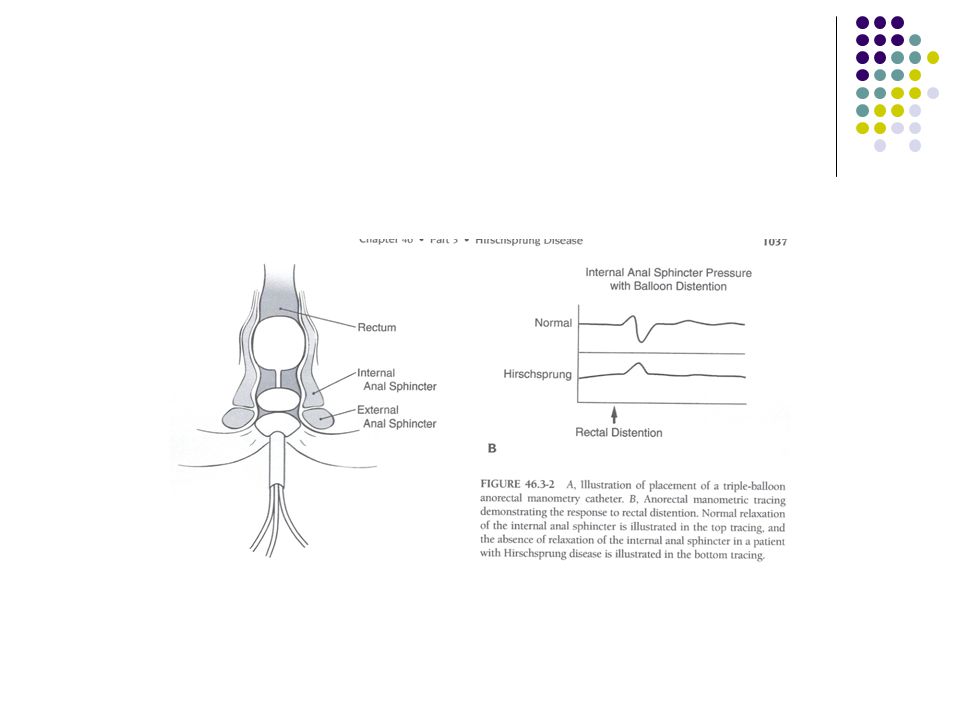
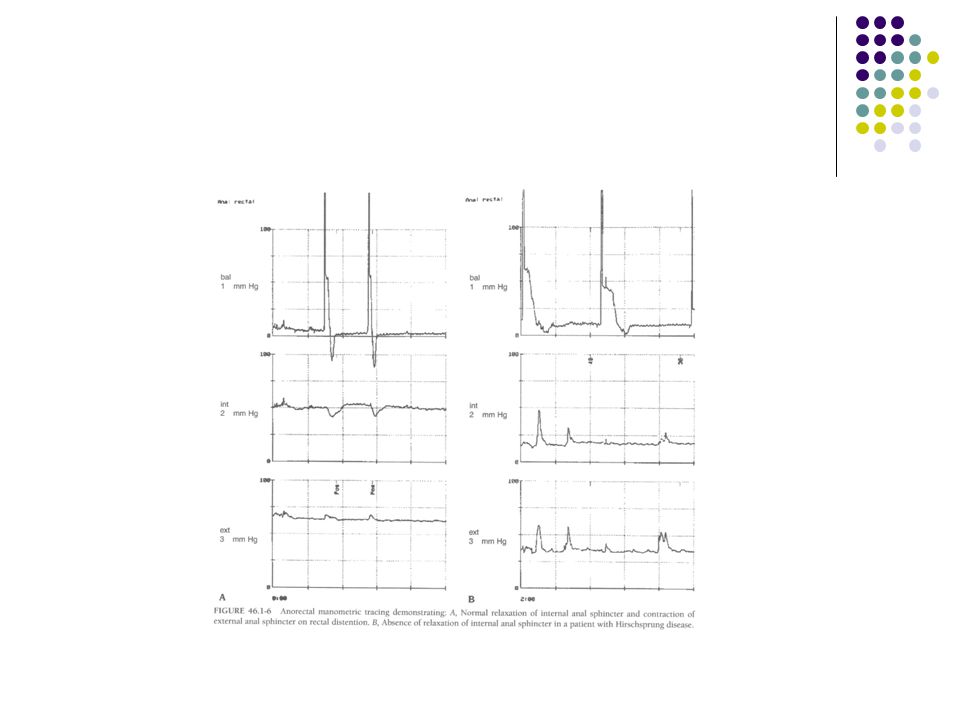
Investigations: Anorectal manometry. Anal sphincter EMG. Defecography. Colorectal transit study.

45
Management

46
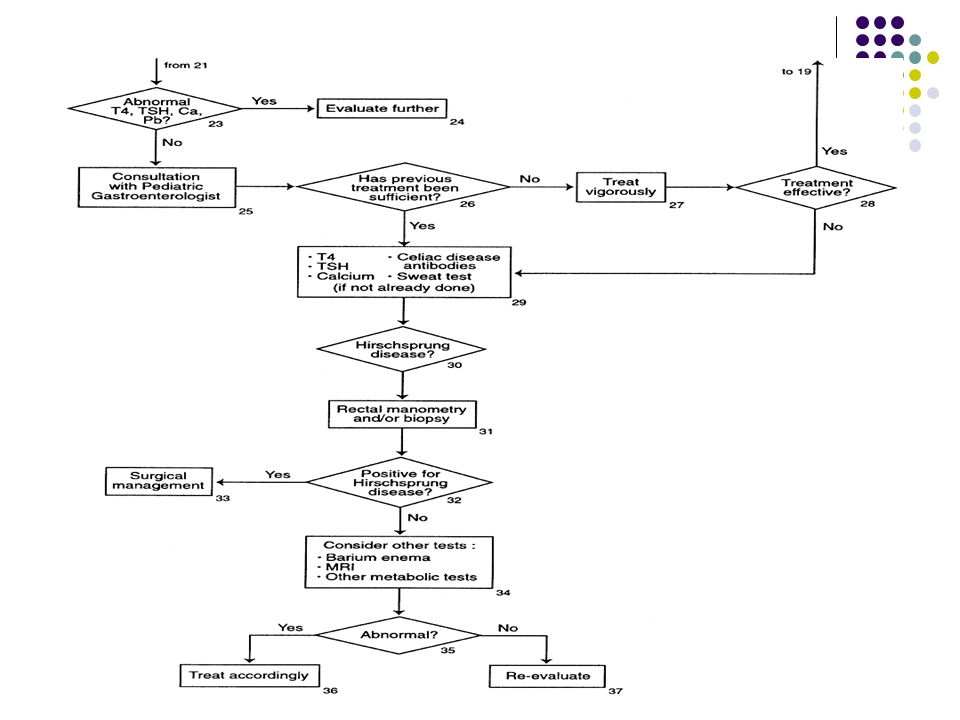
Management: Evaluation and Treatment of Constipation in Infants and Children: Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition [Clinical Practice Guideline] J Pediatr Gastroenterol Nutr 2006 Sep; Vol. 43 (3), pp. e1-13.
![Management: Evaluation and Treatment of Constipation in Infants and Children: Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition [Clinical Practice Guideline] J Pediatr Gastroenterol Nutr 2006 Sep; Vol.](http://images.slideplayer.com/15/4777873/slides/slide_46.jpg "43 (3), pp. e")
47
Management: Education. Disimpaction. Maintenance. Behavioral modification.

48
Education: Educate the family and the child if possible: Pathophysiology That incontinence is not willful. Use drawings to explain.

50
Disimpaction: Fecal impact evacuation: Phosphate enema (fleet enema) Oral medication e.g. mineral oil (paraffin oil), polyethylene glycol (PEG3350) or both
, polyethylene glycol (PEG3350) or both.")
51
Maintenance: Mieral oil (paraffin oil); 1-3 ml/kg/day Polyethylene glycol (PEG 3350) electrolyte free; 1 g/kg/day
; 1-3 ml/kg/day Polyethylene glycol (PEG 3350) electrolyte free; 1 g/kg/day")
52
Maintenance: Lactulose, Mg hydroxide, Sorbitol, others have been used On and off laxatives e.g. Senna

53
Maintenance: In case of anal fissure, apply petroleum gel to anal area frequently

54
Maintenance: Increase dietary fibers Prune ((قراصيه Pear juice Apple juice

55
A comparative study: The efficacy of liquid paraffin and Lactulose in management of chronic functional constipation Liquid paraffin is more effective in the treatment of children with constipation. NAFIYE URGANCI et al Pediatrics International (2005)
.")
56
Behavioral modification: Regular toilet habit (after meals) Keep diary and record (use calendar and stars) Motivation (avoid negative comments)
 Keep diary and record (use calendar and stars) Motivation (avoid negative comments)")
57
Consultation with specialist: Pediatric G.I. (Celiac disease, etc.) Endocrine (hypothyroidism, etc.) Nephrology (diabetes insipidus) Pediatric surgery (Herschsprung)
 Endocrine (hypothyroidism, etc.) Nephrology (diabetes insipidus) Pediatric surgery (Herschsprung).")
58
Biofeedback: Lack of coordinated relaxation of external sphincter while defecation On manometry

61
Biofeedback: There is no evidence that biofeedback training adds any benefit to conventional treatment in the management of functional fecal incontinence in children Brazzelli, M et al The Cochrane Library, Copyright 2006

62
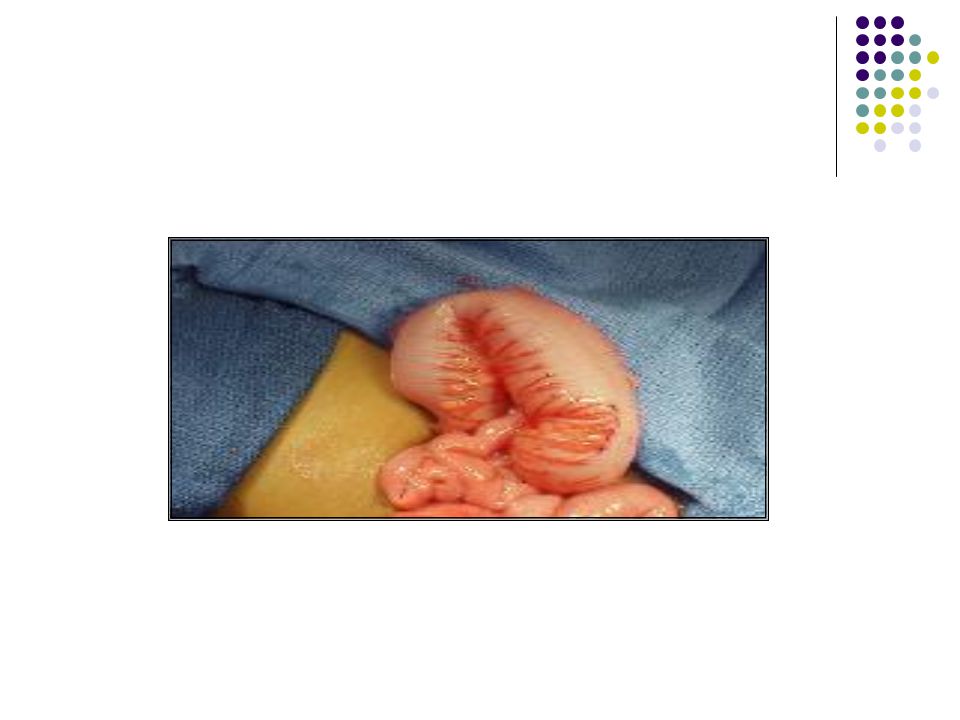
Surgical Treatment: Anorectal myectomy The Malone appendicocecosomy (for retrograde irrigation)
")
63
Long-Term Outcome of Functional Childhood Constipation Childhood constipation appears to be a predictor of IBS in adulthood. Seema Khan et al Digestive Diseases & Sciences; Jan 2007

67
Thank you

68
Hirschsprung Disease Frequency In the US: Hirschsprung disease occurs in approximately 1 per 5000 live births. Pathophysiology: Hirschsprung disease results from the absence of parasympathetic ganglion cells in the myenteric and submucosal plexus of the rectum and/or colon.

Similar presentations





















 Adequate, but not excessive, fibre intake.>")








