Download presentation
Presentation is loading. Please wait.

1
Precancer, benign and malignant tumors of the uterus and ovary Eduard Kučera

2
UTERINE FIBROIDS

3
RISK FACTORS ● They are many risk factors 1 associated with the development of uterine fibroids 1.Flake GP et al, Environmental Health Perspectives 2003; 111(8):1037-54
:")
4
Mass effects related to the size and location of fibroids Pregnancy complications Bleeding complaints These symptoms and consequences have been shown to diminish quality of life 3 When symptomatic, fibroids can be linked to at least three major problems 3 WHAT ARE THE SYMPTOMS? ● Not all fibroids are symptomatic ● However, for the 50% of women with symptomatic fibroids, the condition is debilitating. 1 ● Symptoms can include: ● Abnormal or heavy menstrual bleeding 1, 2 ● Pain, 1,2 pressure symptoms 1,2 and urinary symptoms 2 ● Impairment of Quality of Life 2 1.Tropeano G, Amoroso S, Scambia G. Hum. Reprod. Update (2008) 14 (3): 259-274. 2.Downes E, Sikirica V, Gilabert-Estelles J. et al. Eur J Obstet Gynecol Reprod Biol. 2010; 152(1): 96-102. 3.Viswanathan M, Hartmann K, McKoy N. et al. Evid Rep Technol Assess (Full Rep). 2007 Jul;(154):1-122. Review.
 14 (3): Downes E, Sikirica V, Gilabert-Estelles J. et al. Eur J Obstet Gynecol Reprod Biol. 2010; 152(1): Viswanathan M, Hartmann K, McKoy N. et al. Evid Rep Technol Assess (Full Rep) Jul;(154): Review..")
5
MECHANISMS FOR FERTILITY IMPACT Mechanistic: space; abnormal contractions Local inflammation for sperm and embryo Inadequate blood supply

6
DIAGNOSIS - WHEN AND HOW? ● Physical examination may be the first signal that a woman might have uterine fibroids. 1 ● Imaging methods to evaluate these benign tumours: 1 ● Ultrasonography ● Hysteroscopy ● Magnetic resonance imaging (MRI) 1.Evans P, Brunsell S. Am Fam Physician. 2007 May 15;75(10):1503-1508.ian
 1.Evans P, Brunsell S. Am Fam Physician May 15;75(10): ian.")
7
TREATMENT Uterine Fibroids

8
THERAPEUTIC APPROACH Currently, therapies are intended to reduce or eliminate uterine fibroid symptoms through one of the following options 1 ● Reduction of the size of tumours ● Reduction of the amount of bleeding ● Removal of the uterine fibroids or uterus 1.Miller CE, Journal of Minimally Invasive Gynecology 2009; 16:11–21

9
THERAPEUTIC APPROACH The choice of therapy is influenced by the patient’s ● Symptom severity ● Tumour characteristics (e.g. volume, localisation) ● Age ● Uterine preservation wishes ● Fertility preservation wishes
 ● Age ● Uterine preservation wishes ● Fertility preservation wishes.")
10
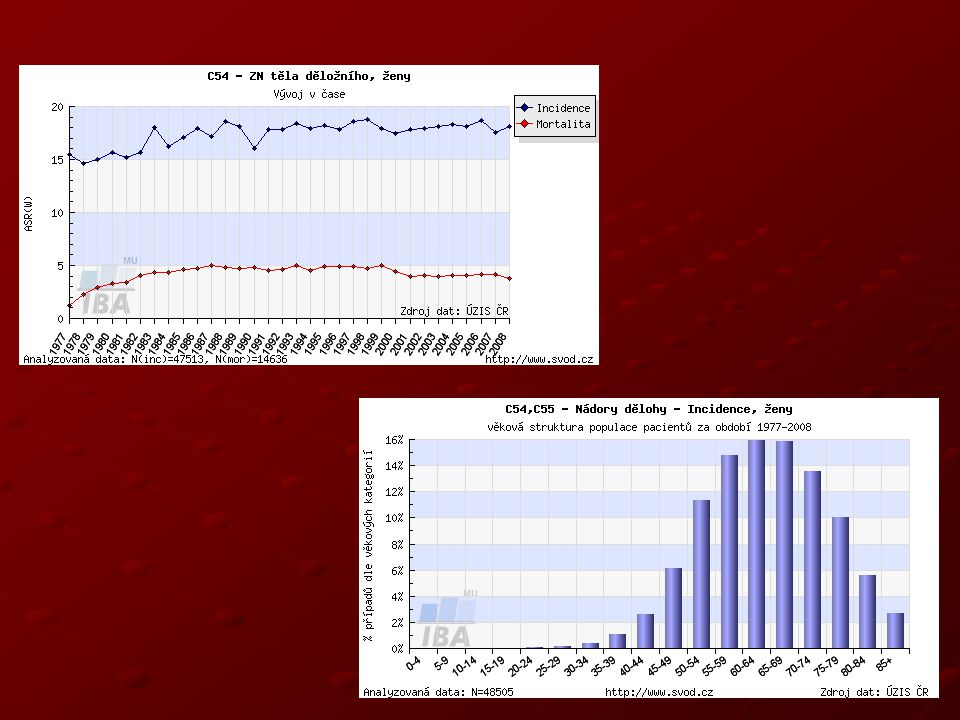
Endometrial cancer Endometrial cancer – most common gynecological malignancy 4th most frequent malignancy in women In Czech Rep. incidence 32/100 000 year 1500 new cases diagnosed per year (e.g. in UK 6,430) Maximum around 60 - 70 years Obesity of women – typical phenotype
 Maximum around years Obesity of women – typical phenotype.")
12
Etiology so called „endometrial carcinoma syndrome“: obesity, (DM, hypertension) - peripheral transformation of androgens - peripheral transformation of androgens - insufficiency of ShBG - insufficiency of ShBG recently often used so celled.: postmenopausal syndrome age: 6. - 7. decade nulliparity (RR=2,8) Infertility (RR=8) late menopause (RR= 2,4) estrogen producing ovarian cancers high intake of animal proteins and fats exogenous estrogens - unopposed gestagens (RR=2,3) tamoxifen (RR=2,4)
 Infertility (RR=8) late menopause (RR= 2,4) estrogen producing ovarian cancers high intake of animal proteins and fats exogenous estrogens - unopposed gestagens (RR=2,3) tamoxifen (RR=2,4).")
13
Carcinogenesis in peri- and postmenopausal women Carcinogenesis in peri- and postmenopausal women younger women older women complex hyperplasia de novo hyperplasia with atypia endometrial carcinoma ( Type I usually well diff. ) ( Type II usually poorly diff. ) endometroid carcinoma papillary serous clear cell carcinoma younger women older women complex hyperplasia de novo hyperplasia with atypia endometrial carcinoma ( Type I usually well diff. ) ( Type II usually poorly diff. ) endometroid carcinoma papillary serous clear cell carcinoma
 ( Type II usually poorly diff. ) endometroid carcinoma papillary serous clear cell carcinoma younger women older women complex hyperplasia de novo hyperplasia with atypia endometrial carcinoma ( Type I usually well diff. ) ( Type II usually poorly diff. ) endometroid carcinoma papillary serous clear cell carcinoma.")
14
Histological types Carcinoma (98%) endometroid adenocarcinoma adenocarcinoma with squamous cells clear cell carcinoma papillary serous spinocellular Sarcoma (2%) leiomyosarcoma endometrial stromal sarcoma mixed mesodermal cancers
 endometroid adenocarcinoma adenocarcinoma with squamous cells clear cell carcinoma papillary serous spinocellular Sarcoma (2%) leiomyosarcoma endometrial stromal sarcoma mixed mesodermal cancers")
15
Hyperplasia of endometrium Complex atypical hyperplasia = precancerosis of endometrial carcinoma ( especially endometroid type) Complex atypical hyperplasia = precancerosis of endometrial carcinoma ( especially endometroid type) - cell polymorphism, mitosis, nucleoplasmic index, hyperchromatosis -creation is independent on estrogen stimulation in atrophic endometrium -creation is independent on estrogen stimulation in atrophic endometrium Motlík,K, Živný,J.:Patologie v ženském lékařství,Grada,2001. Complex atypical hyperplasia = precancerosis of endometrial carcinoma ( especially endometroid type) Complex atypical hyperplasia = precancerosis of endometrial carcinoma ( especially endometroid type) - cell polymorphism, mitosis, nucleoplasmic index, hyperchromatosis -creation is independent on estrogen stimulation in atrophic endometrium -creation is independent on estrogen stimulation in atrophic endometrium Motlík,K, Živný,J.:Patologie v ženském lékařství,Grada,2001.
 Complex atypical hyperplasia = precancerosis of endometrial carcinoma ( especially endometroid type) - cell polymorphism, mitosis, nucleoplasmic index, hyperchromatosis -creation is independent on estrogen stimulation in atrophic endometrium -creation is independent on estrogen stimulation in atrophic endometrium Motlík,K, Živný,J.:Patologie v ženském lékařství,Grada,")
16
FIGO staging 2010 The 2010 FIGO staging system is as follows: Carcinoma of the Endometrium IA Tumor confined to the uterus, no or < ½ myometrial invasion IB Tumor confined to the uterus, > ½ myometrial invasion II Cervical stromal invasion, but not beyond uterus IIIA Tumor invades serosa or adnexa IIIB Vaginal and/or parametrial involvement IIIC1 Pelvic lymph node involvement IIIC2 Para-aortic lymph node involvement, with or without pelvic node involvement IVA Tumor invasion bladder mucosa and/or bowel mucosa IVB Distant metastases including abdominal metastases and/or inguinal lymph nodes

17
5 – year survival year Stage5 year survival rate I-A90% I-B88% I-C75% II69% III-A58% III-B50% III-C47% IV-A17% IV-B15%

18
Hysteroscopy and dg. curettage Curettage – frequent false negative results (10-50%) Curettage – in polyps up to 61% Hysteroscopy and targeted biopsy < 2% false negative results (Gimbelson, Loffer 1988, 1989, AJOG) Studies in 1383 histological findings obtained with D&C - 60% inadequate results (Smith, 1985) In 60% patients curetted < 1/2 cavity of the uterus (Stock, Obst.Gyn.,1975) Curettage – frequent false negative results (10-50%) Curettage – in polyps up to 61% Hysteroscopy and targeted biopsy < 2% false negative results (Gimbelson, Loffer 1988, 1989, AJOG) Studies in 1383 histological findings obtained with D&C - 60% inadequate results (Smith, 1985) In 60% patients curetted < 1/2 cavity of the uterus (Stock, Obst.Gyn.,1975)
 Curettage – in polyps up to 61% Hysteroscopy and targeted biopsy < 2% false negative results (Gimbelson, Loffer 1988, 1989, AJOG) Studies in 1383 histological findings obtained with D&C - 60% inadequate results (Smith, 1985) In 60% patients curetted < 1/2 cavity of the uterus (Stock, Obst.Gyn.,1975) Curettage – frequent false negative results (10-50%) Curettage – in polyps up to 61% Hysteroscopy and targeted biopsy < 2% false negative results (Gimbelson, Loffer 1988, 1989, AJOG) Studies in 1383 histological findings obtained with D&C - 60% inadequate results (Smith, 1985) In 60% patients curetted < 1/2 cavity of the uterus (Stock, Obst.Gyn.,1975).")
19
Diagnostic hysteroscopy - options Panoramatic view – magnified 1x conventional hysteroscopy allows viewing the whole uterine cavity and locate pathologies cavity and locate pathologies panoramatic macro-hysteroscopy – 20x magnification in distance < 1 cm Micro-contact hysteroscopy – 80x magnification allows evaluation of endometrial vascularisation, gland characteristic and their openness Panoramatic view – magnified 1x conventional hysteroscopy allows viewing the whole uterine cavity and locate pathologies cavity and locate pathologies panoramatic macro-hysteroscopy – 20x magnification in distance < 1 cm Micro-contact hysteroscopy – 80x magnification allows evaluation of endometrial vascularisation, gland characteristic and their openness

20
Tamoxifen a endometrium Nonsteroidal synthetic anti-estrogen Adjuvant therapy in breast carcinoma Accumulation of effective substance in basal endometrium Endometrial proliferative abnormality (up to 40% postmenopausal women) - polyps, hyperplasia as much as endometrial carcinoma (2-3/1000/year) Higher risk of endometrial carcinoma after using more then 5 (?) years (2-7.5x) Most safe and effective screening is hysteroscopy in yearly intervals Nonsteroidal synthetic anti-estrogen Adjuvant therapy in breast carcinoma Accumulation of effective substance in basal endometrium Endometrial proliferative abnormality (up to 40% postmenopausal women) - polyps, hyperplasia as much as endometrial carcinoma (2-3/1000/year) Higher risk of endometrial carcinoma after using more then 5 (?) years (2-7.5x) Most safe and effective screening is hysteroscopy in yearly intervals
 - polyps, hyperplasia as much as endometrial carcinoma (2-3/1000/year) Higher risk of endometrial carcinoma after using more then 5 ( ) years (2-7.5x) Most safe and effective screening is hysteroscopy in yearly intervals Nonsteroidal synthetic anti-estrogen Adjuvant therapy in breast carcinoma Accumulation of effective substance in basal endometrium Endometrial proliferative abnormality (up to 40% postmenopausal women) - polyps, hyperplasia as much as endometrial carcinoma (2-3/1000/year) Higher risk of endometrial carcinoma after using more then 5 ( ) years (2-7.5x) Most safe and effective screening is hysteroscopy in yearly intervals")
21
Tamoxifen – endometrium pathology Length of therapy not more then 5 years Metrorrhagia always indication to endometrial examination In asymptomatic women (cca 70%) HSK vs. UZ part of periodic yearly check ups High percentage of false positive results with ultrasound examination– stromal edema (vacuolar degeneration) Tamoxifen - 37 - 71% incidence of polyps – proliferative activity in epithelial and stromal part Incidence of endometrial carcinoma cca in 3% Length of therapy not more then 5 years Metrorrhagia always indication to endometrial examination In asymptomatic women (cca 70%) HSK vs. UZ part of periodic yearly check ups High percentage of false positive results with ultrasound examination– stromal edema (vacuolar degeneration) Tamoxifen - 37 - 71% incidence of polyps – proliferative activity in epithelial and stromal part Incidence of endometrial carcinoma cca in 3%
 Tamoxifen % incidence of polyps – proliferative activity in epithelial and stromal part Incidence of endometrial carcinoma cca in 3% Length of therapy not more then 5 years Metrorrhagia always indication to endometrial examination In asymptomatic women (cca 70%) HSK vs. UZ part of periodic yearly check ups High percentage of false positive results with ultrasound examination– stromal edema (vacuolar degeneration) Tamoxifen % incidence of polyps – proliferative activity in epithelial and stromal part Incidence of endometrial carcinoma cca in 3%.")
22
Tamoxifen and endometrium International agreement – 1997 Bioptical examination of the endometrium before beginning the therapy After 3 years of using observation in yearly intervals Lancet,1698-1711,2000. International agreement – 1997 Bioptical examination of the endometrium before beginning the therapy After 3 years of using observation in yearly intervals Lancet,1698-1711,2000.

23
Tamoxifen and endometrium Hysteroscopy with biopsy – first choice in patients with Tamoxifen therapy Symptomatic patients and therapy longer then 3 years Positive family history Taponeco,F et al. Indication of hysteroscopy in tamoxifen treated breast cancer patients. J.Exp.Clin.Cancer,21,2002 Hysteroscopy with biopsy – first choice in patients with Tamoxifen therapy Symptomatic patients and therapy longer then 3 years Positive family history Taponeco,F et al. Indication of hysteroscopy in tamoxifen treated breast cancer patients. J.Exp.Clin.Cancer,21,2002

24
Endometrial cancer - therapy Surgery - radical Radiotherapy Hormonal therapy

Similar presentations







 Stated as >")











>")