Download presentation
Presentation is loading. Please wait.

1
PATHOLOGY Chronic Renal Failure 2015

2
Objectives Recognize the clinical pathological correlation of biological progression and gross and microscopic features of Polycystic disease. List the commonest disease processes leading to obstruction or reflux and describe the gross features of these diseases and their complications. Describe the gross and microscopic features of renal vascular disease (hypertension, atherosclerosis). Recognize the general principles of a chronic immune complex mediated glomerulonephritis as illustrated by Systemic Lupus Erythematosis (SLE). Recognize the features of segmental fibrosis in glomeruli that occur as a result of increased single nephron perfusion in remaining nephrons in states of chronic loss of total nephron number.
. Recognize the general principles of a chronic immune complex mediated glomerulonephritis as illustrated by Systemic Lupus Erythematosis (SLE). Recognize the features of segmental fibrosis in glomeruli that occur as a result of increased single nephron perfusion in remaining nephrons in states of chronic loss of total nephron number..")
3
Pathology of Chronic Renal Disease *Progressive loss renal function * Associated with compensatory hyperfiltration *Over time hyperfiltration causes further damage (maladaptive) *With progressive damage the original etiology can be obscured by non specific scarring
 *With progressive damage the original etiology can be obscured by non specific scarring")
4
Review of pathology of common causes of Chronic renal failure Pre:(chronic hypoperfusion/ Ischemic Post: obstruction/ backpresssure Renal: hereditary,chronic glomerulonephritis, metabolic abnormalities, tubulointerstitial diseases

5
Review of pathology of common causes of Chronic renal failure Congenital / hereditary (10%) Obstructive/ chronic pyelonephritis/ other tubulointerstitial diseases (10%) Diabetes (30%) Hypertension/ vascular (25%) Glomerulonephritis (15-20%)
 Obstructive/ chronic pyelonephritis/ other tubulointerstitial diseases (10%) Diabetes (30%) Hypertension/ vascular (25%) Glomerulonephritis (15-20%)")
6
CASE #1 Adult Polycystic Disease Example of Hereditary disease leading to CRF 52 year old man Presented at 35 years of age with flank pain and gross hematuria Kidneys enlarged by palpation bilaterally Also hypertensive Mother died of an intracerebral hemorrhage Mother had kidney disease of uncertain type Prior to death the patient was dialysis dependent then received a renal transplant He died of infectious complications at 52 years old Kidneys are from autopsy

7
Adult Polycystic disease Overview Relatively common (4-10% CRF) Autosomal dominant PKD 1 and 2 most common PKD1 on chromosome 16 represents 85% abnormal protein polycystin 1 Protein thought to be important for cell interaction and tubular growth and differentiation There is active secretion into the cysts PKD2 usually less severe Individual cases can be unpredictable as to age of CRF Other abnormalities Cysts of liver spleen pancreas. Mitral valve prolapse, intracranial berry aneurysm, hypertension, diverticulosis

9
Normal kidney

10
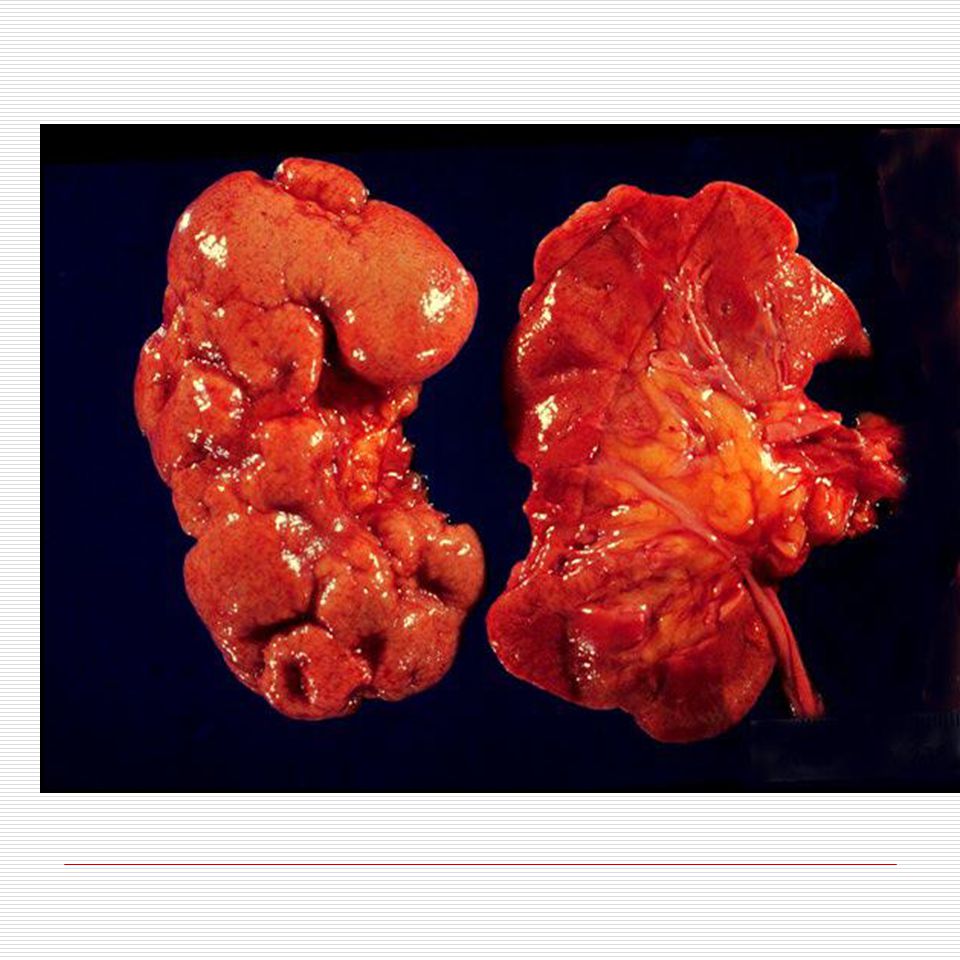
Bilaterally enlarged kidneys distorted by numerous cysts

11
Cut surface shows cysts leaving little residual kidney Some cysts show hemorrhage within them

12
Histological section and corresponding schematic

13
Cysts can occur at various levels Pressure results in atrophy of adjacent tissue

14
Screening Ultrasound need to have cysts big enough No need to diagnose early as no treatment unless decision re having children or donating a kidney from transplant Genetic screening available but cannot predict severity or age of onset

15
Child, MVA victim with early changes of Adult Polycystic Kidney Disease

16
Ultrasound

17
MRI Liver Cystic kidney cysts

18
CASE #2 Obstruction with hydronephrosis 44 year old woman with past history of Invasive carcinoma of cervix Rx with radiotherapy Prior to death developed progressive renal failure

19
tumour

20
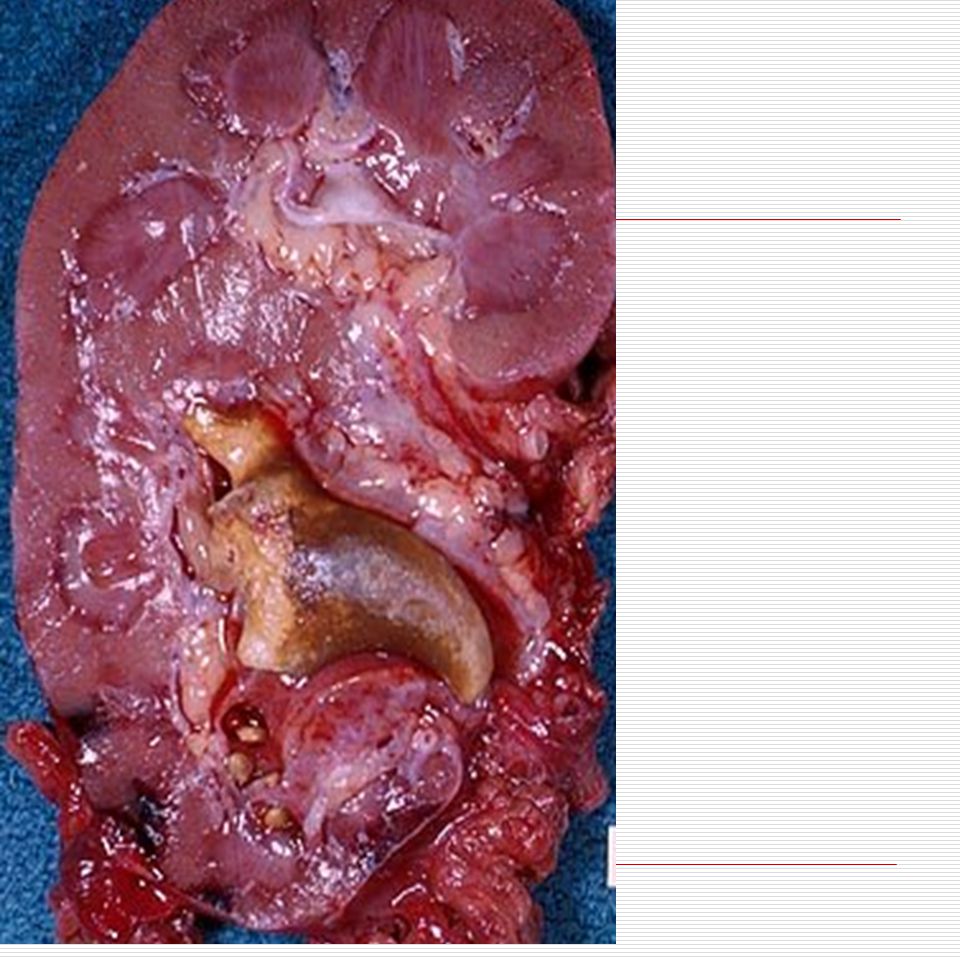
Hydroureter and hydronephrosis

21
Normal Hydronephrosis

22
Features: - Interstitial fibrosis -Atrophic and dilated tubules -Secondary effects on glomeruli

24
End Stage Hydronephrosis Progression to end stage

25
Histology of end stage kidney is similar no matter initial cause. Fibrosis, atrophy and non specific inflammation Often with thickened arteries. Dilated tubules may look thyroidized Clues may still be seen focally or on gross

26
Other causes of mechanical obstruction - calculi - tumours - congenital - inflammation

27
Renal Calculi

28
Renal calculi in ureter

30
primary Tumour within ureter with obstruction

33
Posterior urethral web

34
Retroperitoneal fibrosis

35
ill defined inflammation and fibrosis

36
Case #3 Pseudo obstructive/ non mechanical Complications of obstruction Patient with history of Multiple sclerosis As a sequela developed a neurogenic bladder (did not contract and empty properly) Complicated by numerous episodes of infection.
 Complicated by numerous episodes of infection.")
37
Scarring Chronic pyelonephritis

38
Renal pelvis Cortical abcesses Infected medulla with linear streaks Infection can be a complication of obstruction

39
Acute inflammatory cells in tubules

40
Collecting ducts White blood cell cast Interstitial inflammation Repeated episodes of acute inflammation can result in chronic inflammation fibrosis and loss of function

41
End result is Chronic Pyelonephritis With deep scars “U” shaped involving cortex and medulla

44
Deep “U “ shaped scar involving cortex down to renal pelvis

45
Chronic active inflammation extending to and involving calyceal transitional mucosa

46
Scar with Hyalinized scarred glomeruli and atrophic tubules “so called Thyroidization”

47
Ureteropelvic junction “stricture ””

49
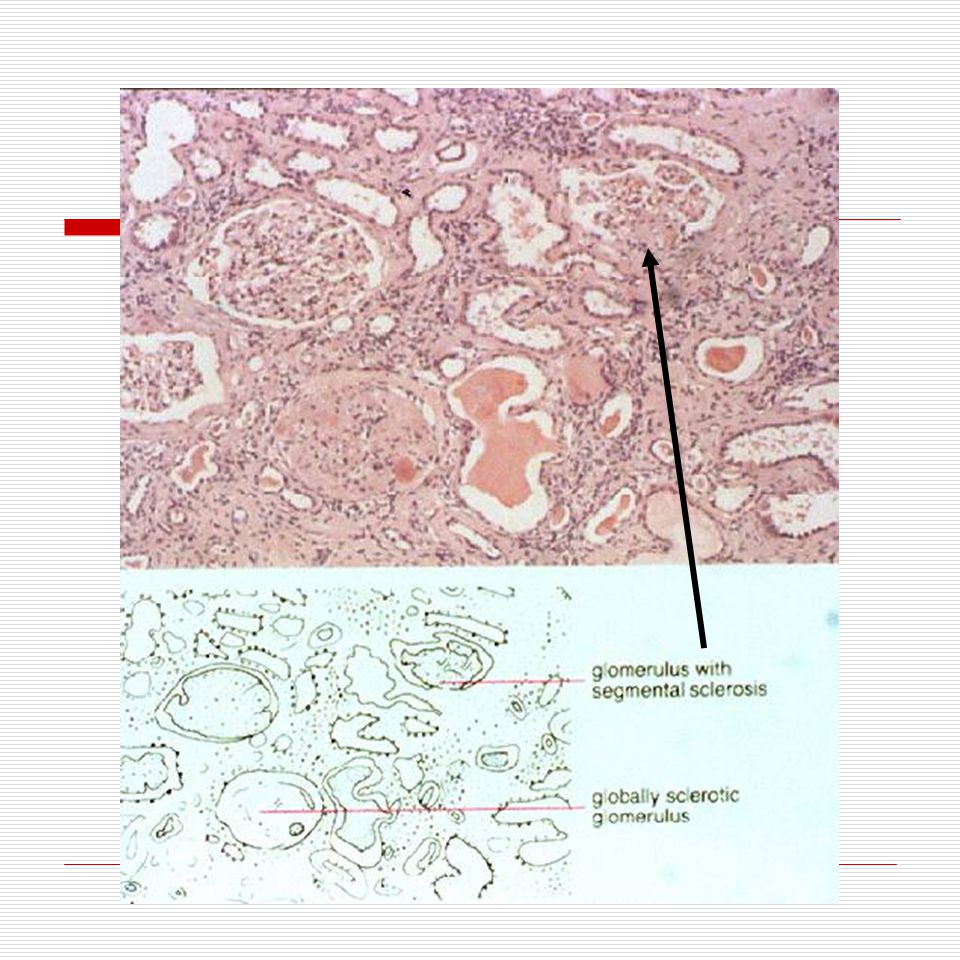
#4 Vascular causes of Chronic renal failure: Arteriosclerosis due to atherosclerosis and arteriolar changes in hypertension As arteries and arterioles become narrow decreased blood delivery results in ischemic changes Glomeruli Ischemic change with wrinkling shrinkage and fibrosis Tubules - atrophic Interstitium Fibrosis and non specific chronic inflammation

50
Arterio and arteriolar Nephrosclerosis Gross -Small kidney Arteriosclerotic scarring with cortical scars small and large but shallower than those of pyelonephritis

52
Microscopy of arteriosclerotic scar Fibrosis of interstitium and glomeruli with associated vessel changes

53
Arteriosclerotic scarring with non specific interstitial inflammation Marked arteriosclerosis with vessel lumen narrowed Periglomerular fibrosis

54
Vascular changes can also result in acute renal failure especially in those already compromised

55
1. Cholesterol emboli Embolic atherosclerotic plaque dislodged from Aorta Risk factors include surgery on atherosclerotic aorta or arteriography Can result in showers of emboli that can lodge in small vessels of kidney and result in acute decrease in renal function in kidneys already borderline in function

56
2. Hypertensive effects can become accelerated (malignant) usually on top of preexisting benign hypertension (1-5% of hypertensive patients) Interlobular arteries and arterioles similar to those in retina can show vessel wall damage that is necrotizing (fibrinoid necrosis) especially at branches & as enters glomerulus There can also be a proliferation of intimal myofibroblasts with narrowed lumen (onion skin) This can result in rapid obstruction or narrowing of blood flow to glomeruli and an ACUTE decrease in renal function
 usually on top of preexisting benign hypertension (1-5% of hypertensive patients) Interlobular arteries and arterioles similar to those in retina can show vessel wall damage that is necrotizing (fibrinoid necrosis) especially at branches & as enters glomerulus There can also be a proliferation of intimal myofibroblasts with narrowed lumen (onion skin) This can result in rapid obstruction or narrowing of blood flow to glomeruli and an ACUTE decrease in renal function.")
57
Gross changes are so called flea bitten kidney with small hemorrhages

58
onion skin" change caused by lamellation mucoid change with swelling of the intimal layer.

59
Fibrinoid necrosis vessel wall damage with fibrinoid eosinophilic material (and red cells) moving into damaged vessel wall.
 moving into damaged vessel wall.")
60
Onion skinning Fibrinoid necrosis vessel wall damage with fibrin (and red cells) moving into damaged vessel wall.
 moving into damaged vessel wall.")
61
Case #5 Glomerulonephritis progressing to chronic phase 30 year old woman with SLE Presented with a diffuse proliferative Glomerulonephritris associated with nephritic picture and decreased serum complement Over three years some exacerbations of disease Now in chronic renal failure with GFR about 30% normal and has a normochromic normocytic anemia

62
Compare to normal http ://www.uptodate.com/contents/image.do?imageKey=NEPH%252F14385

63
Diffuse proliferative glomerulonephritis

65
Proliferation and “Wire Loops ”

66
Small crescent

67
Effective capillary lumen is narrowed by proliferation of cells and deposit of immune complexes and reaction to them

68
Immunofluorescence was positive for IgG, IgA, IGM, C3

69
Multiple deposition sites for Immune complexes seen on EM

70
SLE IV wireloop Large subendothelial deposits There are subepithelial ones also There is an occluding thrombus like structure in lumen Immune complexes fix complement and damage proceeds

71
S00-12090 With continuing damage areas of scarring develop highlighted by this stain which shows collagen in blue-green

72
Interstitial inflammation can also occur with tubular damage fibrosis and tubular atrophy

73
Gross fearures of chronic glomerulonephritis are not specific

Similar presentations


















 RENAL DISEASE: OVERVIEW AND ACUTE RENAL FAILURE Pathophysiology of Disease: Chapter 16 (388-394) Jack.>")
![Case Report # [] Submitted by:Kandra Vogt, MSIV Faculty reviewer:Sandra A. A. Oldham, M.D. Date accepted:31 August 2007 Radiological Category:Principal.](/18/5671912/big_thumb.jpg "Case Report # [] Submitted by:Kandra Vogt, MSIV Faculty reviewer:Sandra A. A. Oldham, M.D. Date accepted:31 August 2007 Radiological Category:Principal.>")






