Download presentation
Presentation is loading. Please wait.

1
Simulation training Curriculum Pericardial Disease

2
Constrictive Pericarditis Etiology Idiopathic Irradiation Post-surgical Infectious Neoplastic Connective tissue disorder Uremia Trauma Sarcoid Methysergide therapy Epicardial implantable defibrillator patches CATHSAP6: Coronary Angiography and Intervention

7
Kussmaul’s Sign CATHSAP6: Coronary Angiography and Intervention

10
Cardiac Tamponade 20 0 40 CATHSAP6: Coronary Angiography and Intervention

11
Balloon Pericardiotomy

12
Case 1: Constrictive Pericarditis 64 year old female 1 Year s/p 3-vessel CABG Presents with 6 months of progressive dyspnea and atypical chest pain At angiography, all grafts are patent Hemodynamics

13
Right atrium 0 20 40

14
LV vs. RV 20 0 40

15
LV vs. RV with Valsalva 20 40 0

16
Constrictive Pericarditis Right Atrial Tracing X-descent y-descent

17
Constrictive Pericarditis – LV vs. RV. Tachycardia Obscures Evaluation PVB

18
Kussmaul sign

19
Case 2: Restrictive Cardiomyopathy 43 year old female presented with predominant right heart failure (peripheral edema, ascites) Hemodynamic tracings suggest constrictive- restrictive physiology Exploratory thoracotomy excluded the presence of constrictive pericarditis
 Hemodynamic tracings suggest constrictive- restrictive physiology Exploratory thoracotomy excluded the presence of constrictive pericarditis")
20
CATHSAP6: Coronary Angiography and Intervention

23
Restrictive Cardiomyopathy

24
Ventricular Interdependence During Respirations Differentiates Constrictive Pericarditis from Restrictive Cardiomyopathy Constrictive Pericarditis (LV and RV discordant) Restrictive Cardiomyopathy (LV and RV concordant) Hurrell et al, Circulation 1996; 93:2007
 Restrictive Cardiomyopathy (LV and RV concordant) Hurrell et al, Circulation 1996; 93:2007")
25
Sensitivities, Specificities, Positive Predictive Values, and Negative Predictive Values as a Function of Criteria Hurrell et al, Circulation 1996; 93:2007

26
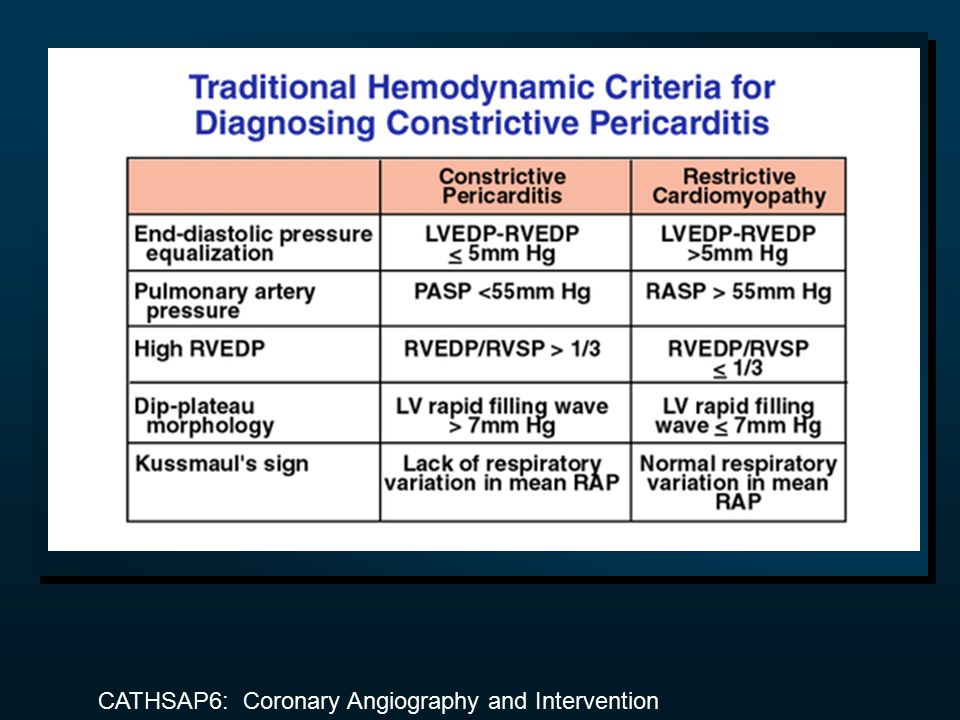
Constrictive Pericarditis vs. Restrictive Cardiomyopathy Greater ventricular interdependence in constrictive pericarditis Greater separation of diastolic pressure in restrictive cardiomyopathy LV and RV diastolic filling more rapid in constrictive pericarditis Pulmonary pressures higher in restrictive cardiomyopathy Adjunctive tests: evidence of pericardial thickening (normal 1-2 mm; thickening ≥ 3 mm); pericardial calcification, RV biopsy, exploratory thoracotomy
; pericardial calcification, RV biopsy, exploratory thoracotomy.")
27
Case 3: Pericardial Tamponade 37 year old female 2 day history of dyspnea, fatigue and dizziness Mastectomy for breast cancer 3 years ago Echocardiogram suggests pericardial tamponade Hemodynamics

28
inspirationexpiration Femoral artery 0 100 200 Cardiac Tamponade Pulsus Paradoxus

29
Right atrium 20 0 40

30
Right ventricle 20 0 40

31
Pulmonary artery 20 0 40

32
Pulmonary capillary wedge 20 0 40

33
Before Pericardiocentesis; Pericardium vs. RA 20 0 40

34
After Pericardiocentesis 20 0 40 Right atrium Pericardium

35
After Pericardiocentesis Right ventricle 20 0 40

36
After Pericardiocentesis Pulmonary capillary wedge 20 0 40

37
Long-Term Effectiveness of Pericardiocentesis 2/3 of patients with malignant pericardial effusions redevelop tamponade after a median of 7 days More than 80% of patients with non-malignant pericardial effusion require no further intervention Laham et al, Heart 1996; 75:67

38
Variants on Constrictive-Restrictive Physiology Acute enlargement of the heart with constriction by normal pericardium –right ventricular infarct, tricuspid regurgitation, mitral regurgitation Low pressure tamponade Effusive-constrictive pericarditis Single chamber tamponade Localized constriction Occult constrictive pericarditis

39
Severe, Acute Tricuspid Regurgitation Associated With Constrictive- Restrictive Physiology

40
Severe, Acute Mitral Regurgitation Associated With Constrictive-Restrictive Physiology

41
Variants on Constrictive-Restrictive Physiology Acute enlargement of the heart with constriction by normal pericardium –right ventricular infarct, tricuspid regurgitation, mitral regurgitation Low pressure tamponade Effusive-constrictive pericarditis Single chamber tamponade Localized constriction Occult constrictive pericarditis

Similar presentations