Download presentation
Presentation is loading. Please wait.

1
Trilogy: Three Initiatives Working Together For Access to the HIV Continuum Amber Rossman, LMSW Kansas City Free Health Clinic 1

2
RUSH-Link 1. Need: for opt-out testing 2. Background: Updated CDC Recommendations 3. Background: CDC: ARTAS & ARTAS II 4. Need: link people to care 5. RUSH: rapid HIV testing in medical settings 6. Link: linking patients to care 7. Future of RUSH-Link

3
3 Video Link: http://www.incarecampaign.org/video/campaign.mp4

4
Getting To Zero... working toward Zero New Infections Zero Deaths due to AIDS 5/19/2015 4 Zero missed opportunities for access

5
Concept: Trilogy Three successful programs each: + tell their own story of daily activity + working toward the same epic tale _____________ = successful access to care

6
1.Expanded Testing Initiative* Funded through Missouri Department of Health by the CDC to expanded HIV testing into medical settings, using opt-out methods 2.Linkage to Care* Funded by Ryan White for early engagement into HIV treatment, immediately after HIV diagnosis 3.MATEC Funded by HRSA as part of the AETC network, providing AIDS and HIV clinical training and support to health care professionals *#1, #2 are collectively known as RUSH-Link The Three Initiatives

7
RUSH-Link Marrying two concepts for one super program: Routine Universal Screening for HIV and Linkage to Care

8
RUSH-Link & MATEC training on HIV 101 training on HIV rapid testing, delivering results, utilizing LTC positive result and beyond continuing education (1+1) + 1 = perfect marriage!
 + 1 = perfect marriage!")
9
Motivation for Scaling Up HIV Testing Unidentified infection: 1,200,000 people in the US living with HIV 280,000 undiagnosed 56,000 new infections per year Poor follow-up: 25% of those testing HIV+ fail to return for results Inadequate linkage to care: only 2/3 of HIV-infected persons receive appropriate care Too little, too late: 40% learn there are HIV-infected in the year prior to AIDS 5% learn it within the month prior to death

10
2006 CDC Revised Recommendations New recommendations for HIV testing are for health care sites only. Including: hospital emergency departments urgent care clinics inpatient services substance abuse treatment clinics public health clinics correctional health-care facilities primary care settings community clinics

11
Updated CDC Recommendations of HIV testing September 22, 2006 Routine voluntary testing for patients 13-64 in all healthcare settings, not based on patient risk – Exception if HIV rates are less than 0.1% Opt-out testing No separate consent for HIV testing Prevention counseling not required Repeat testing at discretion of provider, based on patient risk MMWR Rec Reports 2006 Sep 22; 55(RR-14): 1-17.
: 1-17.")
12
Concept 1: Opt- Out HIV testing Point-of-care testing (POCT) medical testing at site of patient receives the results quicker, allows for immediate clinical management decisions Opt Out patient notified HIV testing will be performed as with other routine screenings patient may decline (opt-out)
 medical testing at site of patient receives the results quicker, allows for immediate clinical management decisions Opt Out patient notified HIV testing will be performed as with other routine screenings patient may decline (opt-out)")
13
Concept 1: Opt- Out HIV testing Point-of-care testing (POCT) medical testing at site of patient receives the results quicker, allows for immediate clinical management decisions Opt Out patient notified HIV testing will be performed as with other routine screenings patient may decline (opt-out)
 medical testing at site of patient receives the results quicker, allows for immediate clinical management decisions Opt Out patient notified HIV testing will be performed as with other routine screenings patient may decline (opt-out)")
14
Primary Care Provider Training Needed Lack of awareness of potential risks of HIV infection in patients by providers Education on CDC guidelines and benefits of early HIV diagnosis with linkage to care Tools for disclosing positive diagnosis and discussing risk behaviors 1. Jain et al. Knowledge of the Centers for Disease Control and Prevention's 2006 routine HIV testing recommendations among New York City internal medicine residents. AIDS Patient Care STDS. 2009 Mar;23(3):167-76. 2.Goetz et al. Evaluation of the sustainability of an intervention to increase HIV testing. J Gen Intern Med. 2009 Dec;24(12):1275-80. 3.Mimiaga et al. Health system and personal barriers resulting in decreased utilization of HIV and STD testing services among at-risk black men who have sex with men in Massachusetts. AIDS Patient Care STDS. 2009 Oct;23(10):825-35.
: Goetz et al. Evaluation of the sustainability of an intervention to increase HIV testing. J Gen Intern Med Dec;24(12): Mimiaga et al. Health system and personal barriers resulting in decreased utilization of HIV and STD testing services among at-risk black men who have sex with men in Massachusetts. AIDS Patient Care STDS Oct;23(10):")
15
Primary Care Provider Training Needed Technical training on rapid HIV tests Knowledge of state laws regarding consent and counseling Education on availability of HIV care resources in the community, e.g., Ryan White grantees 1. Jain et al. Knowledge of the Centers for Disease Control and Prevention's 2006 routine HIV testing recommendations among New York City internal medicine residents. AIDS Patient Care STDS. 2009 Mar;23(3):167-76. 2.Goetz et al. Evaluation of the sustainability of an intervention to increase HIV testing. J Gen Intern Med. 2009 Dec;24(12):1275-80. 3.Mimiaga et al. Health system and personal barriers resulting in decreased utilization of HIV and STD testing services among at-risk black men who have sex with men in Massachusetts. AIDS Patient Care STDS. 2009 Oct;23(10):825-35. Continued:
: Goetz et al. Evaluation of the sustainability of an intervention to increase HIV testing. J Gen Intern Med Dec;24(12): Mimiaga et al. Health system and personal barriers resulting in decreased utilization of HIV and STD testing services among at-risk black men who have sex with men in Massachusetts. AIDS Patient Care STDS Oct;23(10): Continued:.")
16
Kansas City Free Health Clinic

17
Truman Medical Centers: Emergency Dept.

18
Swope Health Services

19
Other Testing Sites

20
2011 RUSH-Link Positivity Rate.33% across all sites TMC @.46% Cabot Westside @.25% KCFHC combined General Medicine and Dental clinics @.25%

21
HIV Testing is important but not sufficient: linkage to care and retention in care are key Cheever LW. Clin Infect Dis 2007; 44: 1500-2

22
Concept 2: linkage to care Early vs. Late Diagnosis and Care AIDS diagnosis within one year of HIV diagnosis is often used as metric for late diagnosis Linkage Completion of one visit with a provider (prescribing), ideally within 90 days of diagnosis
, ideally within 90 days of diagnosis.")
23
Concept 2: linkage to care Early vs. Late Diagnosis and Care AIDS diagnosis within one year of HIV diagnosis is often used as metric for late diagnosis Linkage Completion of one visit with a provider (prescribing), ideally within 90 days of diagnosis
, ideally within 90 days of diagnosis.")
24
RUSH-Link: Linkage to Care Activities 90 Day, Intensive Intervention: Health Literacy, Disease & Treatment 101 Identify patient strengths that facilitate care Identify barriers to care Set goals for HIV tx Negotiate complicated care system Attend appointments; debrief with patient; identify long term payer source “Graduated Disengagement” & “Active Handoff” Person Newly Diagnosed HIV+ LINKAGE: Access to Medical Care ENGAGEMENT: Long term engagement in medical care BARRIERS TO CARE Personal: Support Health literacy Personal priorities Poverty System: Complicated systems Availability Costs

25
2011 RUSH-Link Referred to Care Referrals into LTC: 199 – about17 per month – 44 from ETI sites – 155 from general community

26
Typical LTC Case HIV Diagnosis Page Linkage to Care – 20m response Initial Response – meet with patient and diagnosing provider Linkage to Care - 90 Day, intensive intervention of LTC Case Management 87% COMPLETE: Graduate to long term HIV Case Management Services, continue engagement in care 5% NOT COMPLETE: Lost to Care, Unable to Contact, Disengaged from Program; continued attempts to reach client for re-engagement 8% COMPLETE: Graduate to self-sufficiency, continued HIV care with own resources 84% of graduates still in care after 12 months. Referring Sites Hospitals Health Depts (KC, Jx, Jo, Wy, MO) Publicly Funded Testing Sites KCFHC Med Offices/Other Self Referral Intervention - Enrollment or Referrals
 Publicly Funded Testing Sites KCFHC Med Offices/Other Self Referral Intervention - Enrollment or Referrals.")
27
Referrals 1. Kansas City Health Department 2. Medical Centers/Physicians Offices 3. Other Health Departments 4. Community Testing initiatives 5. Self Referrals, Partner Referrals

28
Race & Ethnicity Black/African American – 51% Caucasian (Non-H) – 35% Hispanic – 8% Other - <3%
 – 35% Hispanic – 8% Other - <3%")
29
Gender Male – 82% Female – 17% Transgender – 1%

30
Future of RUSH-Link Opt-out testing – funded by MODHSS (ETI) Linkage to Care – Funded by KCHD + MODHSS Provider Training – Funded by AETC
 Linkage to Care – Funded by KCHD + MODHSS Provider Training – Funded by AETC")
31
Who will pay? Medicaid: Coverage for HIV serology screening is optional based on state. Medicare: On Dec 8, 2009 CMS ruled that Medicare Part B cover HIV testing for people at risk of infection (defined as anyone who asks for the test). But current CDC screening recommendations are for age 13-64 so would not be relevant. Private insurance: Don’t want HIV testing (don’t want to know)
. But current CDC screening recommendations are for age so would not be relevant. Private insurance: Don’t want HIV testing (don’t want to know).")
32
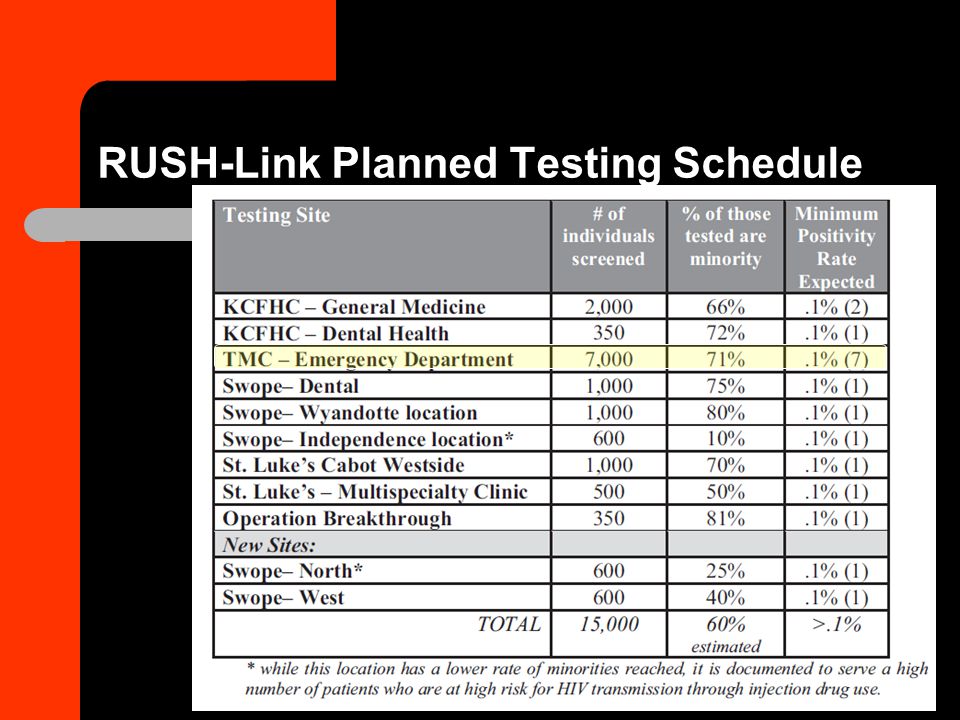
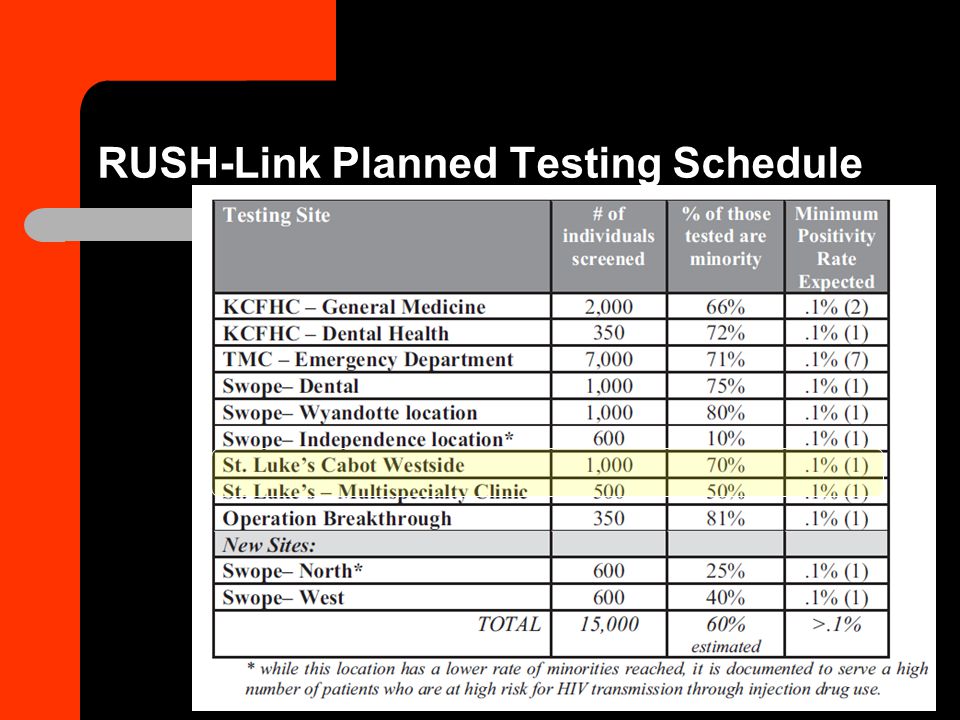
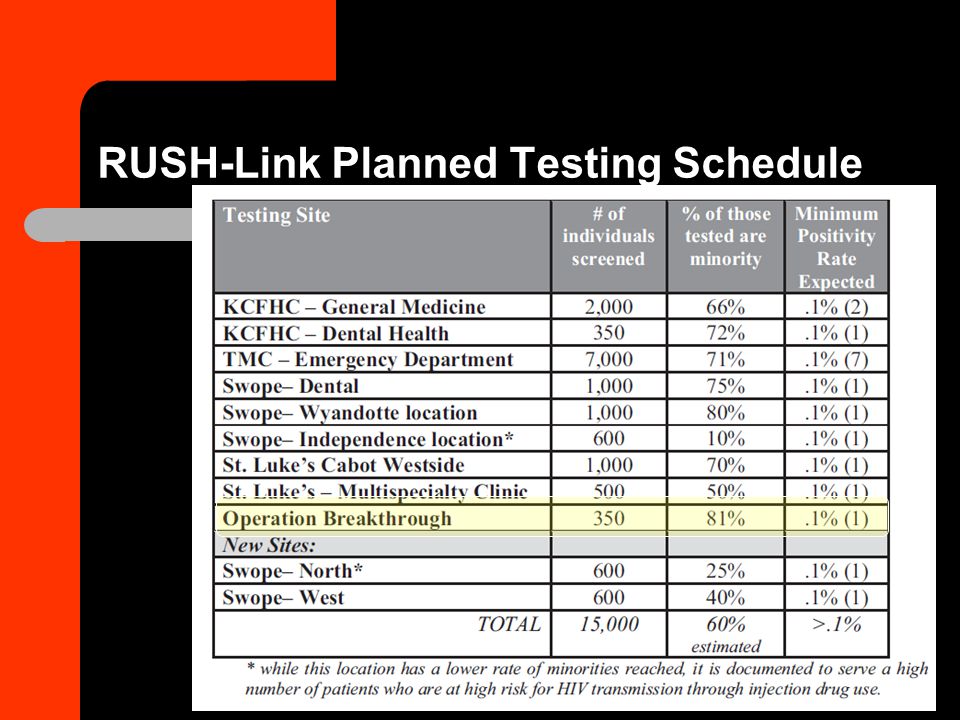
RUSH-Link Planned Testing Schedule

37
Passed Out! Even TB and HIV hit the point of exhaustion from all of the great information at a conference!

38
Appreciation for concepts, inspirations and materials borrowed and expanded upon. Thanks & Appreciation to Many Other Programs www.kcfree.org Amber Rossman, LMSW Program Manager Kansas City Free Health Clinic (soon to be Kansas City CARE Clinic) amberr@kcfree.org 816-777-2729
")
39
Amber Rossman, LMSW Fighting HIV/AIDS?

Similar presentations




 Amber Rossman, LMSW Kansas.>")


 Legislative References: Ryan White Part B Legislation:Ryan White Part B Legislation: “develop.>")












