Download presentation
Presentation is loading. Please wait.

1
Enoch Omonge University of Nairobi
Antibiotic Stewardship Programme at the Kenyatta National Hospital , Nairobi , Kenya Enoch Omonge University of Nairobi

2
Genesis of antibiotic stewardship initiatives at the Kenyatta National Hospital
National Medicines and Therapeutic Committee (Ministry of Health) - AMU Kenyatta National Hospital (KNH)Medicines and Therapeutic Committee KNH Formulary Committee KNH Infection Prevention and Control Unit Kenya Antibiotic Consensus Group (Education)
 - AMU. Kenyatta National Hospital (KNH)Medicines and Therapeutic Committee. KNH Formulary Committee. KNH Infection Prevention and Control Unit. Kenya Antibiotic Consensus Group (Education)")
5
Challenges of infection prevention and Antimicrobial resistance
Referral hospital - large patient population, inadequate patient isolation space and protocol Liberal use of antimicrobials . No preauthorisation policy Delay microbiological sample collection and predominant empiric antibiotic therapy Absence of treatment protocols and guidelines Inadequate local PK/PD data Inappropriate OPAT and easy access to antibiotics

10
Antibiotic protocols as strategy to appropriate antimicrobial use
Providing safe use of antimicrobial Managing antimicrobial resistance Improving quality of care by enhancing appropriate antimicrobial selection Ensuring cost effectiveness

11
Therapeutic options HOST EVIDENCE STANDARDS BUG DRUG AUDITS GUIDELINES
Clinical Laboratory Imaging EVIDENCE EBM STANDARDS BUG DRUG AUDITS GUIDELINES INTERVENTION Rational Cost effective Evolve Omonge e

12
Composition of the multidisciplinary protocol development team
Medical specialists Microbiologists Clinical pharmacists Infection prevention and control team Medicine and therapeutic committee Representative of the hospital administration

13
Process of protocol development
KNH antibiogram used to establish the antibiotic susceptibility pattern Similar protocols to be developed for other hospital units Periodic revision envisaged every two years Modifications in special groups e.g pregnant/lactating mother, renal/hepatic failure, recent antimicrobial therapy, hypersensitivity , drug interactions

14
Antimicrobial stewardship
Selecting appropriate antibiotic Optimising dose and duration of therapy Minimising toxicity Reducing resistance selection

16
Principles of AAU Principles for appropriate prescribing
and effective (locally compliant) guidelines: TREAT bacterial infection only OPTIMIZE diagnosis / severity assessment MAXIMIZE bacterial eradication RECOGNIZE (local) resistance prevalence UTILIZE pharmacodynamics - for effective agents and dosage INTEGRATE local resistance, efficacy and cost-effectiveness Appropriate prescribing conforms to these criteria Ball et al. Antibiotic therapy of community respiratory tract infections: strategies for optimal outcomes and minimized resistance emergence. J Antimicrob Chemother 2002; 49:31–40
 guidelines: TREAT bacterial infection only. OPTIMIZE diagnosis / severity assessment. MAXIMIZE bacterial eradication. RECOGNIZE (local) resistance prevalence. UTILIZE pharmacodynamics - for effective agents and dosage. INTEGRATE local resistance, efficacy and cost-effectiveness. Appropriate prescribing conforms to these criteria. Ball et al. Antibiotic therapy of community respiratory tract infections: strategies for optimal outcomes and minimized resistance emergence. J Antimicrob Chemother 2002; 49:31–40.")
18
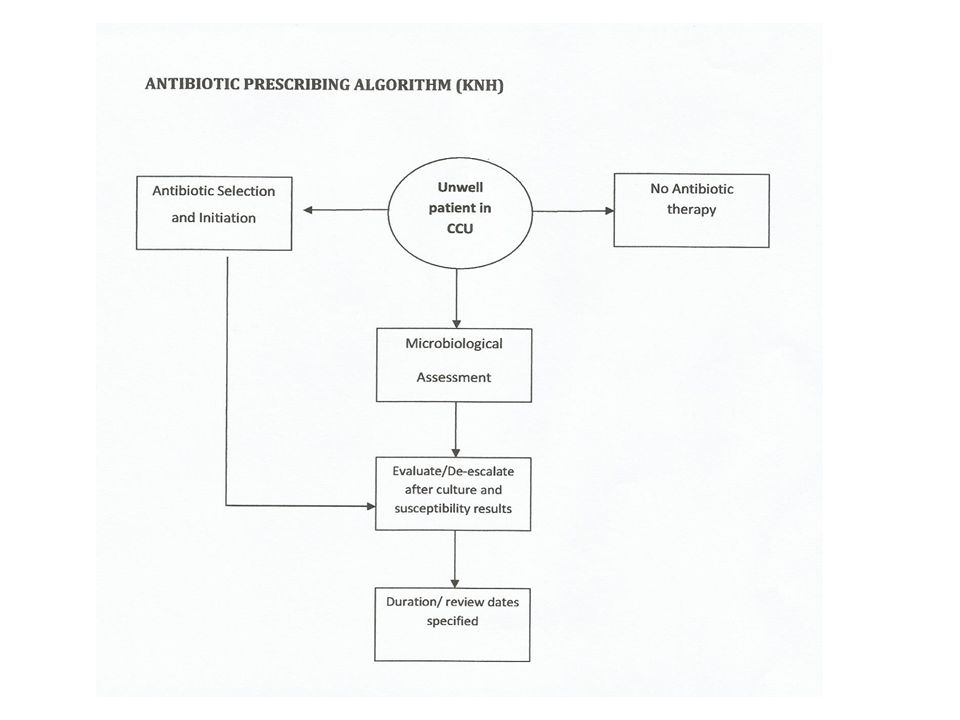
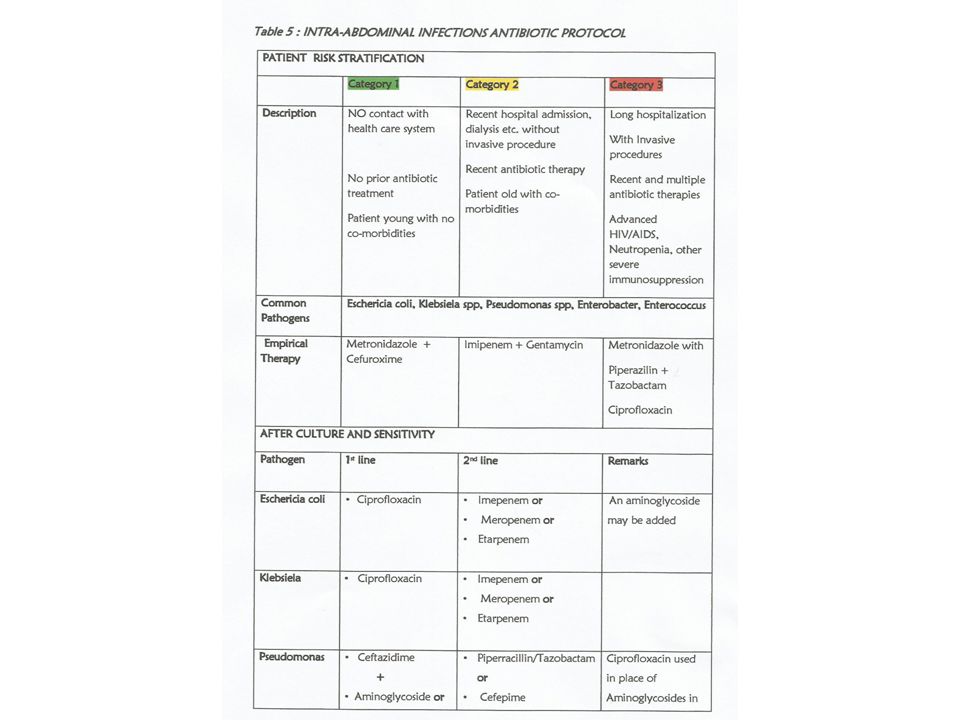
How to use the protocol Identify type of infection – bloodstream, respiratory, intra-abdominal, urinary tract, SSTI Identify location- CCU Risk stratify the patient- category 1,2 or 3 Refer to the empiric therapy column Send respective cultures before starting antibiotics De-escalate with culture reports

20
Data from Jones RN. Clin Infect Dis. 2010;51(S1):S81–7.
Incidence of pathogens isolated in aspirates of patients hospitalised with pneumonia in 2012 at the KNH CCU Incidence of pathogens isolated from patients hospitalised with pneumonia in the United States in the last 5 years of the SENTRY Antimicrobial Surveillance Program Pathogen Incidence (%) n=197 K. pneumonia 22.3 Citrobacter spp. 16.2 Ps. aeruginosa 12.7 E. coli 9.6 Acinetobacter spp. Enterococcus S. pneumoniae 8.1 Proteus spp. 6.6 Enterobacter spp. 5.1 Incidence (%) Pathogen n = 31,346 S.aureus 36.3 Ps. aeruginosa 19.7 Klebsiella spp 8.5 Enterobacter spp 6.5 Acinetobacter spp 4.8 E. coli 4.6 Serratia spp 4.1 Stenotrophomonas maltophilia 3.1 S. pneumoniae 2.5 H. influenzae Data from Jones RN. Clin Infect Dis. 2010;51(S1):S81–7. Data from KNH
 n=197. K. pneumonia Citrobacter spp Ps. aeruginosa E. coli Acinetobacter spp. Enterococcus. S. pneumoniae Proteus spp Enterobacter spp Incidence (%) Pathogen. n = 31,346. S.aureus Ps. aeruginosa Klebsiella spp Enterobacter spp Acinetobacter spp E. coli Serratia spp Stenotrophomonas maltophilia S. pneumoniae H. influenzae. Data from Jones RN. Clin Infect Dis. 2010;51(S1):S81–7. Data from KNH.")
21
Algorithm for classifying patients with hospital-acquired pneumonia according to the Consensus Statement of the American Thoracic Society. Adapted with permission of the American Thoracic Society. Copyright 1996 American Thoracic Society. Hospital-acquired pneumonia in adults: diagnosis, assessment of severity, initial antimicrobial therapy, and preventative strategies. A consensus statement. Am J Respir Crit Care Med 1996; 153:1711–1725.

22
ATS/IDSA algorithm for initiating empirical antibiotic therapy for hospital- acquired pneumonia (HAP), ventilator-associated pneumonia (VAP), and health care–associated pneumonia (HCAP) *Prior antimicrobial therapy (within 90 days), hospitalization for 5 days, high frequency of antibiotic resistance in the community or the hospital unit, immunosuppressive disease or therapy. Adapted with permission of the American Thoracic Society. Copyright American Thoracic Society. Am J Respir Crit Care Med. 2005; 171:388–416.

23
Potential Microorganisms in Each Group According to the 1996 Consensus Statement of the American Thoracic Society. Group 1 Group 2 Group 3 Enteric gram-negative bacilli E. coli Enterobacter spp. Klebsiella spp. Proteus spp. Serratia marcescens H. influenzae MSSA S. pneumoniae Anaerobes MSSA and MRSA Legionella spp. Ps. aeruginosa Acinetobacter spp. MRSA MRSA: methicillin-resistant Staphylococcus aureus; MSSA: methicillin-susceptible Staphylococcus aureus. Am J Respir Crit Care Med 1996; 153:1711–1725

24
Recommended treatment
Initial Empirical Antimicrobial Treatment for Patients with Hospital-Acquired, Ventilator-Associated, or Healthcare–Associated Pneumonia Potential pathogen Recommended treatment No risk factors for MDR, early onset and any disease severity Ceftriaxone; levofloxacin, moxifloxacin, ciprofloxacin; ampicillin-sulbactam or ertapenem S. pneumoniae H. Influenzae MSSA Antibiotic susceptible, enteric gram-negative bacilli E. coli Klebsiella pneumoniae Enterobacter spp. Proteus spp. Serratia marcescens ESBL, extended-spectrum b-lactamase; MDR, multidrug resistant; MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-susceptible S. aureus.

25
Initial Empirical Antimicrobial Treatment for Patients with Hospital-Acquired, Ventilator-Associated, or Healthcare–Associated Pneumonia, Potential pathogen Recommended treatment Late onset disease or risk factors for MDR pathogens and all disease severity Combination antibiotic therapy: antipseudomonal cephalosporin (cefepime or ceftazidime); antipseudomonal carbapenem (imipenem or meropenem) or b-lactam or b-lactamase inhibitor (piperacillin-tazobactam) plus antipseudomonal); fluoroquinolone (ciprofloxacin or levofloxacin) plus linezolid or vancomycin (if risk factors) Ps. aeruginosa K. pneumoniae (ESBL) Acinetobacter spp. Legionella pneumophila MRSA ESBL, extended-spectrum b-lactamase; MDR, multidrug resistant; MRSA, methicillin-resistant Staphylococcus aureus;
; antipseudomonal carbapenem (imipenem or meropenem) or b-lactam or b-lactamase inhibitor (piperacillin-tazobactam) plus antipseudomonal); fluoroquinolone (ciprofloxacin or levofloxacin) plus linezolid or vancomycin (if risk factors) Ps. aeruginosa. K. pneumoniae (ESBL) Acinetobacter spp. Legionella pneumophila. MRSA. ESBL, extended-spectrum b-lactamase; MDR, multidrug resistant; MRSA, methicillin-resistant Staphylococcus aureus;")
Similar presentations