Download presentation
Presentation is loading. Please wait.

1
Malaria Dept. of Infectious Disease Shengjing Hospital CMU

2
Definition Definition Malaria is a parasitosis caused by plasmodia. It is transmitted to human by the mosquito. Clinical feature: cyclic chill, high fever & profuse sweating. In chronic illness, there are anemia & splenomegaly.

3
Etiology Etiology Causative organism: Plasmodia P. Vivax: tertian malaria P. Malariae: quartan malaria P. Falciparum: malignant malaria P. Ovale: tertian malaria Pathogenicity: merozoite, malarial pigment & products of metabolism

4
Etiology Etiology Tachysporozoite Bradysporozoite Merozoite Sporozoite Parasitemia

5
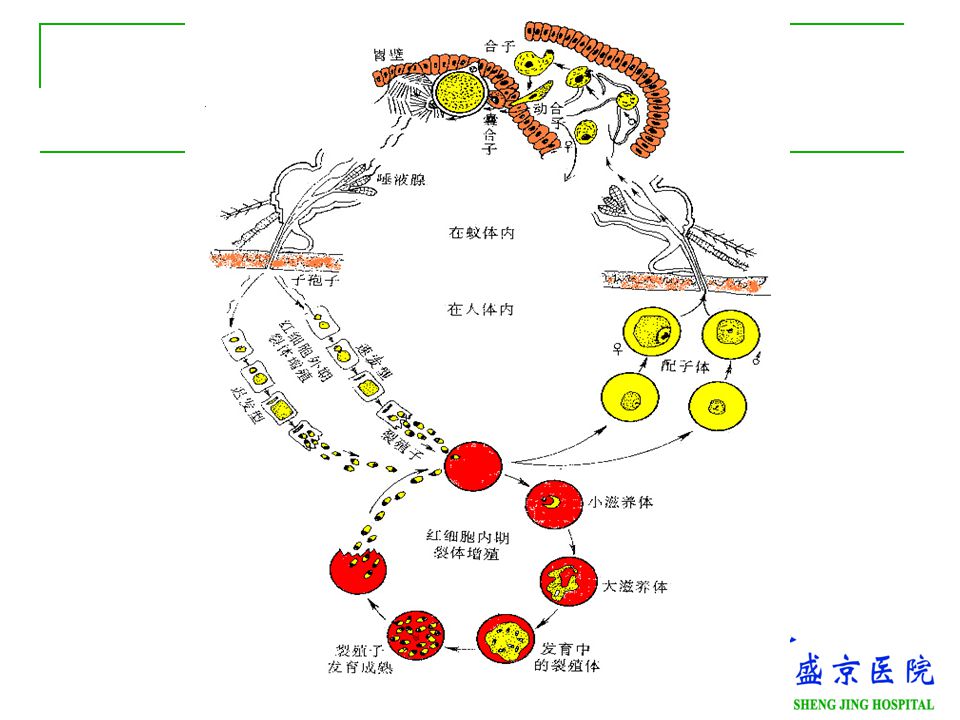
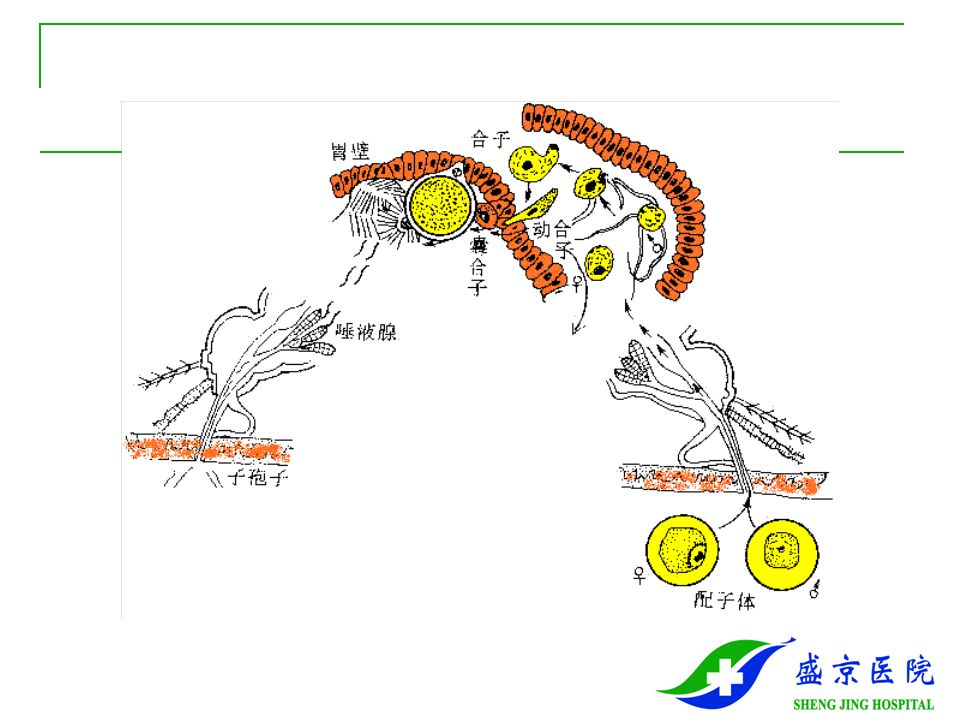
Etiology Etiology Two periods: human - whole asexual reproduction mosquito - sexual parasitic stage Two hosts: human - intermediate host mosquito - final host notes: clinical symptoms: erythrocytic stage relapse: exerythrocytic stage infectivity: sporozoite

6
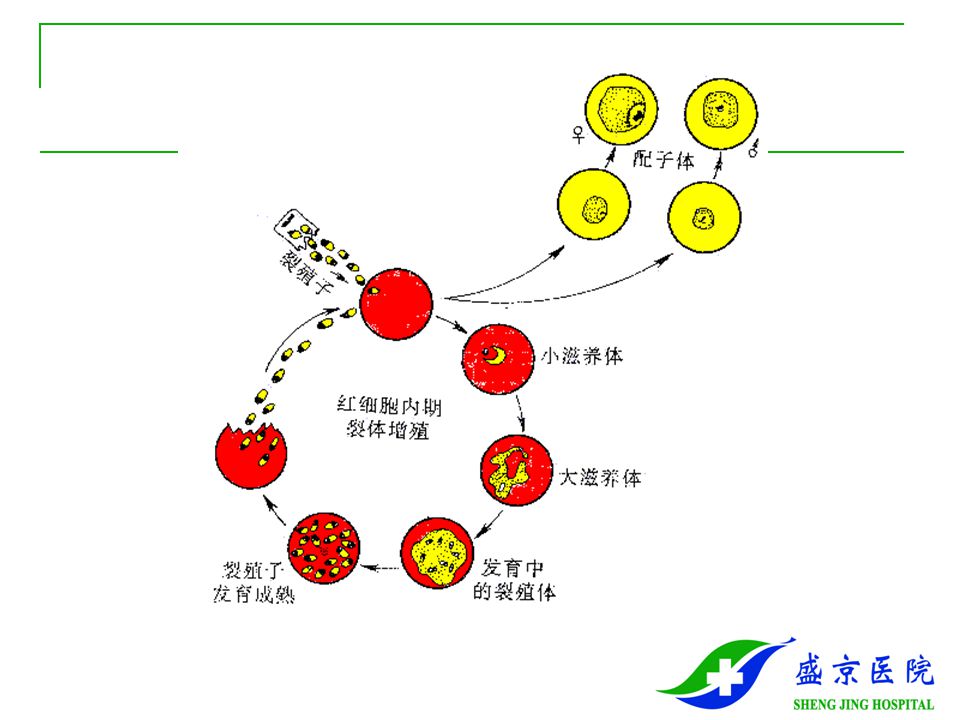
Life cycle of the malaria parasite mosquito microgametocyte zygote oocyst sporozoite Blood stream tachysporozoite merozoite maturerupture Bradysporozoite Blood stream reenter phagocyte merozoite trophzoite shizont mature release merozoite gametocyte Erythrocytic phase Exoerythrocytic stage human

10
Epidemiology Source of infection Patient, parasite carrier Route of transmission female mosquito biting person blood transfusion Susceptibility: universal susceptibility no-cross-immunity re-infection Epidemic features: sporadic or endemic, tropic or subtropic

11
Pathogenesis Pathogenesis Mechanism of attack merozoite RBC rupture malaria pigment products of metabolism blood stream allergy P. Faciparam: produce microvascular disease magnitude of the parasitemia & age of patient no specific Ab or cell -mediated response

12
Pathology Pathology Anemia: P. Vivax - retiform RBC P. Malariae - mature RBC P. Falciparum - every RBC Prolifeation of mononuclear phagocyte hepatomegaly splenomegaly Cerebral edema & congestion

13
Clinical manifestation Clinical manifestation Incubation period: quartan malaria: 24-30 day tertian malaria: 13~15 day malignant malaria: 7~12 day

14
Clinical manifestation Typical attack Chill: abrupt onset, shivering, pale face,cyanosis. Last 10 min or 1~2hr. High fever: T rise to 40 o C with malaise, myalgia, thirsty. Last 2~6 hr. Sweating: profuse sweating with restlessness regular 48 hr. or 72 hr. Cycle

15
Clinical manifestation Sings anemia splenomegaly hepatomegaly, ALT elevate

16
Clinical manifestation Pernicious attack: caused by P. Falciparum cerebral malaria high fever, headache, vomiting, convulsion delirium, respiratory failure hyperpyrexia type T> 42 0 C, convulsion, delirium Relapse: early relapse - <3m, later relapse - >6m

17
Clinical manifestation Malaria caused by transfusion incubation period: 7~10 day no exoerythrogenic phase, no relapse

18
Complications Complications Black- water- fever: cause: 1/inadequate G-6-PD 2/The toxin release by malarial parasite 3/Allergic reaction to anti-malarial drugs feature:1/chill & fever 2/dark red or black urine 3/severe hemolytic anemia Acute glomerulonephritis

19
Laboratory Findings Laboratory Findings Blood picture: decrease in RBC & Hb blood film for parasite serological examination ELISA for P. antigen DNA hybridization

20
Diagnosis Diagnosis Epidemiological data endemic zone blood transfusion Clinical manifestation Laboratory findings Diagnostic treatment: chloroqunine for 3 days

21
Differential Diagnosis Differential Diagnosis Typhoid fever Septicemia Leptospirosis Encephalitis B

22
Treatment Treatment Anti-malarial drugs Chloroquine-susceptable infection chloroquine : 1g /d, for 3 day, p.o. primaquine: for 8day, p.o. Chloroquine-resistant infection mefloguine: artemisinine

23
Treatment Treatment Pernicious attack Chloroquine: 10mg/kg iv drop in 4 hr. Then 5mg/kg, iv drop in 2 hr. Quinine: 500mg iv drop in 4 hr. Radical therapy Chloroquine (3 day) + primaquine ( 8 day )
 + primaquine ( 8 day ).")
24
Prevention Prevention Drug prophylaxis chloroquine: 0.3g once a week doxycycline Kill mosquito Vaccination

Similar presentations








 Symptoms and Diagnosis Treatment Preventive measures Where malaria occurs in the world.>")
 Pathogen of malaria P.vivax ; P.falciparum ;P.malariae ; P.ovale P.vivax ; P.falciparum are more common Plasmodium.>")






. IT REMAINS A MAJOR BURDEN IN TROPICAL COUNTRIES. MALARIA MEANS MAL AIR NEAR.>")

>")
